 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 5, No. 19, October-December 2006, pp. 1226- 1231 Association between dental prosthesis and periodontal disease in a rural Brazilian community Suzely Adas Saliba Moimaz * , Nemre Adas Saliba * , Orlando Saliba* , Lívia Guimarães Zina* , Márcio Rogério Curtis Bolonhez* *Preventive and Social Dentistry Post-Graduation Program, Department of
Pediatric and Social Dentistry, Araçatuba School
of Dentistry, São Paulo State University -
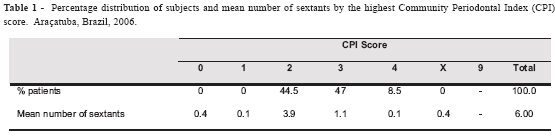
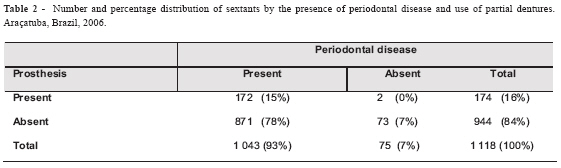
UNESP, Brazil Received for publication: August 13, 2006 Code Number: os06041 Abstract The aim of this study was to describe the periodontal conditions and to analyze the association between the wearing of fixed/removable partial dentures and periodontal disease in a representative adult rural population in southeast Brazil. Cross-sectional study of a representative sample comprising 200 individual aged 34-44 years. Data were collected by clinical examinations in accordance with the World Health Organization Basic Methods Criteria, which included the Community Periodontal Index and dental prosthesis exam. A descriptive analysis and the chi-square statistic were performed. In total, 40.5% of the individuals wore partial denture and 59.5% were non-users of denture. The prevalence of periodontal disease was 100%. The subjects scored either calculus (44.5%) or shallow pockets (47%), and only a small proportion was recorded as having deep pockets (8.5%). All denture wearer displayed periodontal problem in the sextant where the denture were recorded. The statistical analysis indicated that wearing partial dentures was found to be associated with considerable periodontal disease (X2 = 10.75; p=0.0014). The periodontal condition of the study population can be considered unsatisfactory. The wearing of partial dental prosthesis was associated with periodontal disease, and a significant percentage of cases might have been prevented if plaque control interventions had been implemented. Key Words: periodontal diseases, dental prosthesis, oral health, periodontal index, epidemiology Introduction Dental caries and periodontal diseases have been historically considered the most important global oral health burdens. At present, the distribution and severity of oral diseases vary in different parts of the world and within the same country or region. In Brazil, 48.3% of people aged 35-44 years wear at least one dental prosthesis; at 65-74 years-old this rate go up to 66.5%1. The significant role of local, socio-behavioural and environmental factors in oral disease and health is demonstrated in a large number of epidemiological surveys2-6. A global database was established and over a number of years an increasing number of oral epidemiological studies have been conducted applying World Health Organization (WHO) methodology and criteria7. To assess the periodontal status of populations, the WHO recommended the Community Periodontal Index (CPI) application, which verifies the state of periodontal health in view of gingival bleeding, periodontal calculus and pocket. The CPI has been widely used to measure the level of periodontal diseases and treatment needs in populations, and it allows for international comparisons7. Severe periodontitis which may result in tooth loss is found in 5-15% of most populations5-6. A classic study on experimental gingivitis in humans proved that bacterial plaque or biofilm represents the main etiologic factor of periodontal diseases8. Other researches also confirm the importance of controlling biofilm in order to maintain individual oral health9-12. Acting jointly with biofilm, local and systemic factors may modify the pathogeny of periodontal disease, like dental morphology, shape and site of furcation, level and amount of dental restoration, trauma, diabetes mellitus, genetic factors and viruses12. Dental prosthesis may influence the periodontal conditions, the risk of caries and the amount of stress on natural teeth10,13-15. Various investigations have shown that there is an increase in the mobility of the supporting teeth, gingival inflammation and formation of periodontal pocket after dental prosthesis are fitted in16-21. According to some authors22-24, the removable partial denture were associated with increased plaque accumulation, not only on tooth surfaces in direct contact with the denture, but also on teeth in the opposing arch, and in some cases, even on buccal surfaces of teeth. These alterations are attributed to poor oral hygiene, increased plaque and calculus accumulation, and transmission of excessive forces to the periodontal structures from occlusal surfaces of the framework of dentures. Many partial dentures framework designs contribute to increased or altered oral bacterial flora and formation of dental plaque20. In a large case-control study conducted by the University of Zagreb, Croatia, in 2002, 205 partial denture wearers were examined; abutment teeth had higher scores related to periodontal disease than non-abutment teeth, with significant differences (p<0.01) for plaque, calculus and gingival index, probing depth, tooth mobility and gingival recession20. The gingival health is adversely affected by removable partial dentures, with it being most severe where the appliance closely contacted the gingival margin16. The differences in gingival inflammation between the plate and dental bar designs suggest that covering more gingival tissue promotes development of gingivitis, which may subsequently predispose the area to periodontal disease25. In a three-year study with patients wearing fixed partial dentures with advanced periodontal disease, carried out by the researches of the Yonsei University, Korea, it was observed good results regarding the periodontal health situation26. Continuing surveillance of levels and patterns of risk factors of periodontal disease is of fundamental importance to planning and evaluating community preventive activities and oral health promotion. Studies suggest that the use of partial dentures may constitute a risk factor for periodontium health. The aim of this study was to describe the periodontal conditions and to analyze the association between the wearing of fixed/removable partial dentures and periodontal disease in a representative adult rural population in southeast Brazil. Material and Methods Study methodology The target population of the present study was adults living in the rural area of Araçatuba in the Brazilian state of São Paulo. This state is located in the southeast part of Brazil, and is one of the most important states of the country. Two hundred patients aged 35-44 years were examined between August 2004 and January 2005. The sample was randomly selected and weighted to represent the 35-44 year old adult population of rural area of Araçatuba. The specific area where the data were collected has approximately 600 inhabitants (Information provided by Araçatuba Health Municipal Department and the Brazilian Institute of Geography and Statistics - IBGE). The study sample included 80 (40%) males and 120 (60%) females. The sample size was obtained allowing 10% of sampling error27. The sample calculus was derived based on the prevalence of periodontal disease in the region. The prevalence of periodontal disease in São Paulo State was considered 55%, in accordance with research carried out by the University of São Paulo in 199828. The following formula was used for the sample calculus27: N = p q / E2 p is the probability of individuals of the sample having this characteristic; q is the probability of individuals of the sample not having this characteristic. The patients were chosen at random, using the census data and other relevant municipal information. Exclusion criteria were presence of diseases/conditions that may interfere with the clinical examination and the results. Hence, subjects were excluded if they were diagnosed with psychiatric problems, intoxicated with alcohol or dugs, pregnant women and smokers. Clinical examinations Examinations were performed by one dentist, assisted by a recorder, and they were conducted in a health center located in the rural area. Letters were sent to selected individuals and explained the aims of the study and solicited participation. A few days later, the researchers visited the individual and provided more information about the study and encouraged participation. Eligible subjects who consent to participation were invited to go to the local health center in a specific day. Clinical examinations were carried out in natural light. Gauze squares, cotton buds, sterile sets of plane mouth mirrors and Community Periodontal Index (CPI) probes were packed in sufficient quantities for each working day. Strict procedures for infection control were followed. The clinical examination lasted an average of 10 minutes per adult. The Community Periodontal Index (CPI) was recorded for each sextant. Ten index teeth (17, 16, 11, 26, and 27 in the maxilla, and 47, 46, 31, 36, and 37 in the mandible) in six sextants (17-14, 13-23, 24-27, 37-34, 33-43, and 44-47) were probed and scores ascribed to each sextant on the following basis: score 0 - no signs of disease; score 1 - gingival bleeding after gentle probing; score 2 - presence of supra or subgingival calculus or other plaque retentive factors; score 3 - 4 or 5 mm deep periodontal pockets; score 4 - 6 mm or deeper periodontal pockets7. Molars were examined in pairs and the highest score was recorded for each sextant. A sextant was examined if at least 2 teeth are present. A 0.5 mm ball-ended probe with color markers at 3.5 and 5.5 mm was used to measure the CPI. The WHO recommends that the pressure applied in probe should not exceed 20 grams. For each tooth, 6 sites were examined: mesial, midline and distal on both vestibular and lingual/palatal surfaces. Probing depth was defined as the distance from the free gingival margin to the bottom of the pocket/sulcus7. The use of dental prosthesis was evaluated according to criteria recommend by WHO7: score 0: don't wear dental prosthesis; score 1: fixed partial denture wearer; score 2: removable partial denture wearer; score 3: combined dentures (fixed/removable) wearer. Pilot study and calibration Dental examiners participated in a 5-day training and calibration session. The session focused on the interpretation of indexes measuring pathologies sought during examinations and identification of dental prosthesis. Intra-rater reliability and agreement with gold standard dentist were assessed during and at the end of session. The level of concordance for measures relative to periodontal conditions and denture identification was good (mean [kappa] index was 0.80). Later, a pilot study was carried out on adults aged 35-44 years who attended the Araçatuba School of Dentistry Clinic to test the feasibility of the study and dental examination. There was no need to change the methodology previously proposed. Ten percent of the sample (N=20) was re-examined to test for reliability during the fieldwork. Ethical considerations This study was aware of the Code of Ethics of the World Medical Association (Declaration of Helsinki) and it received ethical approval from the Research Ethics Committee of the Araçatuba School of Dentistry (file: FOA 2178/2003). The exams were undertaken with the understanding and written consent of each subject. Confidentiality was assured to participants and all recording forms were numbered, but not named. Data analysis For the descriptive statistical analysis of the periodontal parameters, mean values were calculated for each patient and for sextant, since all patients present alterations in their periodontal condition. The presence or absence of disease and the identification of partial denture in the same sextant were compared, for which the chi-square test were used. Level of statistical significance was chosen at p<0.05. Results Of the 200 subjects recruited into the survey, 81 (40.5%) wore dental prosthesis, fixed and/or removable, and 119 (59.5%) were non-users of denture. Table 1 and Figure 1 show the prevalence of periodontal condition measured by the Community Periodontal Index (CPI) on the subjects who underwent the periodontal examination. Among these subjects, 100% presented some periodontal problem, recorded by the sum of scores 2, 3 and 4, independently of wearing of dentures. The subjects scored either calculus (score 2) or shallow pockets (score 3), and only a small proportion was recorded as having deep pockets (score 4). All denture wearer displayed periodontal problem, as calculus and periodontal pocket, in the sextant where the dentures were recorded. A mean number of 4 sextants presented bleeding and calculus as worse condition, and the sum of these conditions (score 1 and 2) represented 67.13% of total of sextants, whereas only 1 sextant were found to have a pocket of 4 mm or more, score 3 and 4 represented by 19.71% of sextants. The mean number of sextants with healthy periodontal tissues was 0.4, which represents 6.25% of the total. Excluded sextant (score x), due to there remaining less than 2 teeth, were less prevalent (6.83%). The relationship between subjects categorized as exhibiting considerable periodontal disease (score 3 and 4 as worse condition) and those categorized as partial denture wearer is demonstrated in table 2. For the 35- to 44-year-olds rural population, being a partial denture wearer was significantly associated with an increased likelihood of being categorized as exhibiting considerable periodontal disease (X2 = 10.75; p=0.0014). Discussion This paper set out to address the hypothesis that there was an association between the wearing of fixed/removable partial dentures and periodontal condition in a Brazilian adult rural population. The results of this analysis suggest that partial dentures may play an important role in the development of periodontal disease. In this study, all subjects presented signs of periodontal disease. The percentage of patients with periodontal pockets was relatively high (55.5%), but when only deep pockets were considered, the percentage found was much lower (8.5%). A mean number of 5.2 sextant presented bleeding or more severe problems; however, only 1.2 sextants had 4 mm or deeper periodontal pockets. This means that the periodontal alterations were more generalized, affecting more sextants, and having a few severely involved teeth. Thus, gingivitis was the principal clinical manifestation of periodontal disease in the subjects examined. In 2003, a National epidemiological survey showed a percentage of 46.2%, 21.9% and 7.9%, respectively, of individuals with no periodontal problem within the age range of 15 to 19, 35 to 44 and 65 to 74 years1. On comparing the 1986 and 2003 national surveys, the decrease in the rates of periodontal disease prevalence in the Brazilian population is most likely due to conditions such as the consolidation of the National Public Health System and the greater care given to oral health. A study verified the periodontal conditions and treatment needs according to the Community Periodontal Index of Treatment Needs (CPITN) in a worker population in Brazil29. The results showed a mean number of 0.1 healthy sextants, and calculus and shallow pocket were the most prevalent periodontal condition, similar to our findings. Among the factors that account for poor periodontal condition are the lack of professional advice regarding oral health maintenance and the low rate of follow-up19. Besides, the prevalence of periodontal diseases in rural populations seems to be higher than in urban populations. A research performed in rural and urban areas of a Brazilian city compared the oral health condition of these regions, including the main oral diseases as dental decay and periodontal disease, and the authors observed that rural residents had worse index than urban residents30. Another study carried out in a rural area of São Paulo State, Brazil, found values as 99.5% of children aged 6 to 14 years presenting signs of periodontal disease31. Despite some methodological differences among surveys performed with rural populations, it is distinguished the worse periodontal conditions of these populations. To understand these differences, it is necessary to know the social determinants of health involved in the health-disease process of periodontal disease, like income, education, habitation conditions, work, transport, sanitation and environment. In developing countries as Brazil, the iniquities are present in many sections and regions, and the social difficulties can be higher to the population of rural areas, with small wages, worse habitation condition, difficulties in the access of children to school and of people to health services. Various researches18-20 have shown that, on comparing the periodontal condition of abutment teeth and natural teeth, a statistically significant difference was found between both periodontal conditions, the abutment teeth presenting a greater depth of gingival crevice, an increase of calculus and dental mobility. It is believed that the increase in plaque accumulation is related to negligence of the patient and not necessarily brought about by the prosthesis. That periodontal alterations may be solely due to the patient's poor oral hygiene with no prosthesis involvement in this result32. Older patients maintain hygiene of natural teeth better than denture hygiene, and their results underscore the need for better instruction on maintaining denture hygiene20. A study comparing patients with removable partial dentures, patients with no prosthesis, or patients with fixed partial dentures showed the greatest plaque and calculus deposition, periodontal probing depth, and alveolar bone loss on the abutment teeth in removable partial denture wearers33. Some studies examined effects of forces transmitted to abutment teeth, jiggling, and eventual orthodontic tooth movement, and the results showed that such forces did not induce periodontal disease or progressive destruction of the periodontium if good hygiene was maintained 19,32. The prevalence of denture wearers with periodontal disease in the present survey was significant. The factors related to the development of periodontal disease could be involved both in sites with and without dentures, and probably one of the most evident factors was poor oral hygiene as observed by the authors during the clinical examinations. Thus, evaluation of the wearing of partial dentures and periodontal condition must be carried out based on several evidences related to the importance of controlling bacterial plaque in order to preserve the integrity of the periodontium. However, the in situ effect of dental prosthesis must not be overlooked in relation to its multiple functionality aspects, such as definition of margins and prosthetic adaptation which, if not correct, may effectively contribute to the development of periodontal disease. Agreement exists among several authors about the need for oral home care and a regular recall system, which influences the success of prostheses26,34-35. Clinical studies showed that when providing a regular recall system with control, re-instruction and re-motivation, partial dentures might not cause any damage of the periodontium. In a retrospective study, the changes in the periodontal conditions of patients wearing different designs of removable partial dentures over long-term were evaluate, and found a higher deterioration in the abutment teeth than in the non-abutment teeth35. According to these authors, the substantial dental and periodontal destruction in patients with partial dentures is found more frequently in patients who had a poor oral hygiene and seldom visited their dentist. Every patient should be included in a preventive oral health service, with control of bacterial plaque by the dentist and the patient. To maximize cost-effectiveness, prevention and control of periodontal diseases should be based on predicted risk of developing these diseases. In populations with low level of oral hygiene and limited oral health care resources, a "whole population" strategy for general oral health promotion should be applied36. Besides this, based on the risk profile, the basic strategy should be individualized treatment to eliminate infection by periopathogens and to control or/and reduce modifying risk indicators, risk factors and prognostic risk factors, as the wearing of dental prostheses. For rural populations, the strategies must emphasize the importance of adapting the services to the necessities and difficulties of those populations. The access to health services must be facilitated so all can be assisted, not only in relation to curative treatment, but also, and mainly, to preventive and educative activities. Finally, the results highlight the need for further epidemiologic studies to clarify the relationship between dental prosthesis and periodontal disease, types of dentures and period of development of disease. In conclusions, the wearing of partial dental prosthesis was associated with periodontal disease in this study population, and a significant percentage of cases might have been prevented if plaque control interventions had been implemented. The results suggest a need for populations-based plaque control programs in an attempt to reduce the incidence of development of periodontal disease in population. Acknowledgements This work was supported by general institutional funds from the Research Foundation of State of São Paulo, Brazil (FAPESP). References
© Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os06041f1.jpg] [os06041t2.jpg] [os06041t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}