 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 5, No. 19, October-December 2006, pp. 1239-1243 Comparison between two methods to record occlusal contacts in habitual maximal intercuspation Cláudio Wilson Lima Ferro Cabral1* , Frederico Andrade e Silva2 * , Willkens Aurélio Buarque e Silva2* , Alexandre Brait Landulpho3 * , Ligia Buarque e Silva4* 1Specialist in Prothesis , MS, PhD in
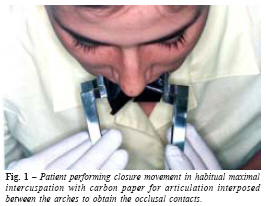
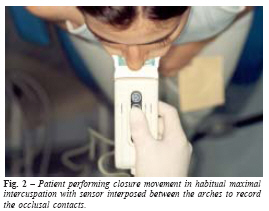
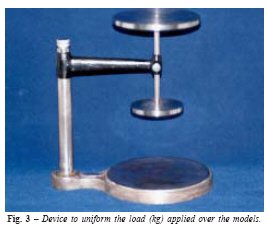
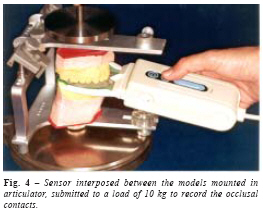
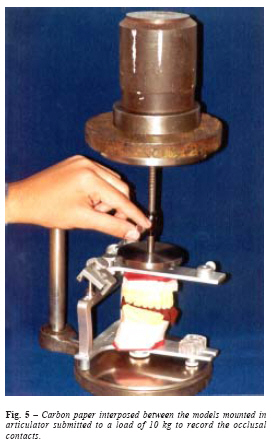
Dental Clinic Received for publication: October 02, 2006 Code Number: os06043 Abstract This research evaluated two techniques to record the occlusal contacts in habitual maximal intercuspation obtained in models mounted in semi adjustable articulator and in the mouth using an eight-micrometer carbon paper and sensors (T-Scan II). It was selected a sample of twenty five people, male and female, ages between twenty and twenty five years old with natural dentition. The collected data were visually and statistically evaluated by means of the Spearman coefficient. The results showed that the carbon paper as material used for the occlusal contact records enabled to determine exactly the quantity and its locations in the occlusal surface. However, it did not provide the information on the sequence, time and intensity on how these occur. The T-Scan system enabled to determine the quantity, the sequence and the exact time that they occur, however the system did not determine the exact location of the contacts over the teeth occlusal surface. It was observed that in both methods, the quantity of the occlusal contacts recorded in the mouth was higher than the ones obtained in the articulator and that the sensor thickness did not interfere in the reproduction of the quantity of dental contacts in comparison to the carbon paper. Key Words: dental occlusion, bite registration, diagnostic techniques Introduction In the last decades, a considerable quantity of patients report symptoms such as: noises in the TMJ´s, limitation on the mouth opening, pain in the preauricular region and headache. Those symptoms increasingly have been related with functional disharmonies of the stomatognathic system. Among the factors that can cause the temporomandibular dysfunction the occlusal contacts are highlighted. Several studies showed that premature contacts and/or occlusal interference caused changes in the functional activity of the masticatory muscles1-9, and that these changes in the way how the teeth are in occlusal contact could intensify the forces that come to the temporomandibular articulation during the mandible functional movements and as a consequence a remodeling in the soft and hard tissues of the TMJ´s could occur10-11. Furthermore, if the correct occlusal is ignored in a rehabilitation with prostheses or with silver amalgam filling both of them will have a doubtful prognostic12. Throughout the years several researchers, aiming to identify the exact location of the occlusal contacts, developed and evaluated different techniques and materials, such as: light crossing; bite record strips; wax; occlusal sonography; soot over models; black carbon or with oily dye; printing materials; photo occlusion; T-Scan computerized system, and more recently the Dental Prescale System13-21. It was also suggested the occlusal pathology diagnostic was carried out with the patient's models mounted in articulator22-23. The defenders of each technique reported that they provided the identification of the occlusal contacts satisfactorily. However, in practical terms, many of them are confusing and inexact. Considering this fact, several researchers carried out investigations to evaluate the performance of the techniques and materials used to record the occlusal contacts13,20,24-32 . However, there is still controversy referring to the dependability of each one. This research searched to compare the reproduction of the occlusal contacts obtained through two techniques: the one that uses the sensor coupled to the T-Scan II computerized system and the conventional technique that uses the articulator and carbon paper for the articulation. Material and Methods Twenty five students, male and female, ages between twenty and twenty five years old of the Undergraduate Dentistry School of Piracicaba Unicamp, Piracicaba, Brazil, with complete natural dentition except the third molars with no extensive coronary destruction and with no prosthetic restoration. Two techniques were compared in order to evaluate the record of the occlusal contacts on the posterior teeth with the mandible in habitual maximal intercuspation: the traditional one that uses models mounted in articulator and carbon paper for the articulation interposed between plaster models to confirm the reproduction of the contacts obtained in the mouth; and the one that uses a sensor coupled to the T-Scan II computerized diagnostic system obtaining the occlusal contacts directly in the mouth and in real time. The traditional method is based on the Lauritzen33 studies that suggested that the occlusal contact analysis could be carried out in plaster models previously mounted in an articulator that reproduced the mandibular movements satisfactorily. For the use of this method several previous steps should be carried out: molding of the dental arch, getting the models, mounting of the upper model in the articulator with the help of the face-bow, determining the maxillomandibular relationship, mounting of the lower model in the articulator, individualization in the articulator of the Bennett angles and the condylar guidances, setting the anterior guidance, reproduction in the occlusal contact models using the carbon paper for visual analyses of the contacts. The articulator used in this research was a semi adjustable (GNATUS 9600 Gnatus Equip. Med. Odont. Ltd, Brazil) Arcon type according to the American Dental Association classification. In order to obtain the record with the T-Scan II system the individual was oriented to sit down on a dental chair in a way that the Camper's plane and the bipupillary line would be parallel to the floor and then the contacts were registered and recorded for a later evaluation. The selected individuals were molded with silicone condensation through the mass/rebasing technique in accordance with the manufacturer recommendation. The molds were leaked with plaster IV type by using a vibrator. The plaster was provided and manipulated manually in accordance with the manufacturer recommendation. The upper models were mounted in a semi adjustable articulator with the help of the face-bow and hard plaster, type IV, added in two steps in order to minimize the effects of the setting expansion over the model position. The mounting of the lower model in the articulator was carried out using the record of the maxillomandibular relationship in habitual maximal intercuspation (HMI) obtained by means of the direct interdigitation between the models as stated by Walls et al.9. After determining the maxillomandibular relation the lower model was stabilized in the upper model by using the rubber bands. At the end of this procedure the relationships between the models were compared to the one observed in the individual mouth in order to assure an adequate mounting. The occlusal contacts were obtained and recorded in the mouth and in the models of each patient with paper for articulation of eight-micrometer AccuFilm II (PARKELL, Farmingdale, NY, USA) and also using the T-Scan II system whose sensor has sixty micrometers of thickness. The records of the occlusal contacts in the mouth not only with paper for the articulation but also with the sensor were also obtained with the patient sat down on the dental chair with the Camper's plane and bipupillary line parallel to the floor andmouth closure up to get habitual maximal intercuspation. The occlusal contacts with carbon paper were obtained after drying the occlusal surface. Each patient was instructed to close the mouth in HMI and to repeat the movements three times putting maximum strength in the final closure (Figure 1). From each patient it was obtained three records in different days always in the beginning of the afternoon. The T-Scan computerized system records were obtained after the set alignment (handling device, fork gadget and sensor) with the individual midline. After this step, it was started the record by the operator that asked for the patient to execute the closure three times and that at the end of the closure by using maximum strength (Figure 2). To record the occlusal contacts in the models it was developed a device that enabled to make uniform the static load applied to the articulator (Figure 3). This device avoided any variation applied over the models. The sequence for getting the occlusal contacts in the models was the same in both techniques and consisted of readapting the models in the articulator mounting plates, removing the incisal pin, positioning the articulator in the load device in order to produce the desired strength (Figure 4 and 5). This procedure was repeated twice for each element of the sample. The contacts obtained with carbon paper for the articulator were recorded and filed by means of a camera and those obtained with the T-Scan II system sensor were filed in compact disk (CD). The analysis of the data collected in the mouth and in the articulation consisted of evaluating visually and statiscally the quantity and the location of the occlusal contacts. To carry out the statistical analysis the data were entered in the Bio-Estat 2.0 program in a paired way and the selected statistical testing was the Spearman correlation. Results The results showed the quantity of occlusal contacts obtained in the mouth was the same not only with carbon paper but also with the sensor. The quantity of occlusal contacts in the articulator was also the same with the carbon paper and with the sensor. When compared the quantity of obtained occlusal contacts in the articulator and the mouth with the carbon paper and sensor, the contacts in the articulator were in a lower quantity. In relation to the location not only in the mouth but also in the articulator when it was used the carbon paper, the contacts repeated, that is, its location was the same in the two situations. However, when the sensor was used it was not possible to determine the location of the occlusal contacts. In the mouth, the quantity of contacts on the left and right sides with carbon paper when compared to the one obtained by the sensor, it showed a positive correlation, i.e., Spearman coefficient = 0.8728 (p=0.0000) and Spearman coefficient = 0.9970 (p=0.000) respectively. The record of the occlusal contact quantity obtained in the articulator with carbon paper and with sensor on the left and right sides also presented a positive correlation, Spearman coefficient = 1.000 and Spearman coefficient = 1.000 (p=0.0000) respectively. Comparing the quantity of the contacts obtained with carbon paper in the mouth to the ones observed in the articulator, it was verified a positive correlation in the two situations, Spearman coefficient = 0.2029 (p=0.3306) for the left side and Spearman coefficient = 0.4296 (p=0.0320) for the right side. In the comparative analysis of the quantity of contacts obtained in the mouth and in the articulator with sensor, positive correlations were observed not only on the left side but also on right side, Spearman coefficient = 0.2654 (p=0.1996) and Spearman coefficient = 0.4237 (p=0.0347) respectively. Discussion In the pilot surveying of this research was observed that a variation in the strength intensity in the mandible closure in habitual maximal intercuspation interfered in the quantity of occlusal contacts obtained. This remark had already been subject o research being demonstrated that the occlusal contacts increase significantly with the increase of the strength during the occlusion among the teeth34. Some researches showed that the skull position also interferes in the mandible position and that the ideal position to obtain the occlusal contacts would be a neutral position35. In this research, the neutral position was determined by maintaining the Camper plane parallel to the floor during the procedures to get the occlusal contacts. A comparative study about the reproducibility of the occlusal contacts using the T-Scan system and using carbon papers showed that the papers were more accurate than the T-Scan system32. This result differs from the one obtained in the present research that did not detect difference between the records done with carbon paper and those gotten through the sensor. Probably, the explanation for this fact is that the methodology did not standardize the intensity of the closure in habitual maximal interscupation since the authors did not state this. Another research states that carbon papers used to evidence occlusal contacts recorded false-positive contacts over the plaster models mounted in articulator in comparison with the T-Scan computerized system that showed more trustful results28. The results obtained by us did not show any numerical difference in the record of the contacts obtained with carbon paper and sensor in the articulator. It is possible that this divergence is related to the different characteristics presented by the articulators used in the researches. Furthermore, it should be considered the differences related to the load application. In some cases, the applied load was generated in the posterior region of the models and in this work; the load was applied almost directly over the models. Studies with the T-Scan system concluded that the records done with the system showed a lower contact quantity than the ones obtained when aluminum foil was used26. The difference in the results presented by the two studies may be related to the fact that in this research some variables were controlled such as: closure intensity and head position while in the other work this variables are not mentioned by the author. The evaluation about the size of the areas of the occlusal contacts obtained in plaster models mounted in articulator using carbon papers between eight and forty micrometers of thickness and the operator experience in the variation of the contact area showed that these two factors influenced in the variation of the size of the areas36. These results differ from the ones obtained in the present research in which two materials with different thickness were used to record the occlusal contacts in the mouth and over plaster models and differences have not been found between both of them during visual evaluation. Our results also showed that the dental contact quantity in the articulator was lower than those ones found in the mouth. This fact can be explained partially due to the plasticity of the maxilla and mainly the mandible, as well as by the capacity of the intrusion of the teeth in their alveolus during the contacts in habitual maximal intercuspation. Research using the photo occlusion technique also showed that depending on the increase of the strength of the mandibular closure the quantity of dental contacts also increased20. This can also be observed when we use the T-Scan II computerized system to record the occlusal contacts in the mouth and in the articulator. This shows that the occlusal profile is dynamic presenting numerical changes and most probably in the size of the contact area, depending on the variation in the intensity of the closure strength. In this study it was established that the T-Scan system enabled to record exactly the quantity, sequence, distribution in the arches, the intensity and time of duration of the occlusal contacts, but it could not identify precisely the location of the contacts in the teeth occlusal surface nor their area size. The record with eight-micrometer carbon paper provided the exact location of the occlusal contacts and the dimension of their areas, however it was not able to define their sequence, intensity and time of duration. Based on these remarks an association of the sensor with carbon paper is suggested during the records of the occlusal contacts. References
© Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os06043f5.jpg] [os06043f4.jpg] [os06043f3.jpg] [os06043f1.jpg] [os06043f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}