 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
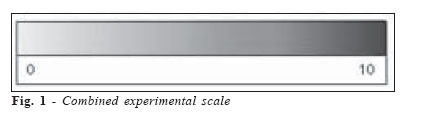
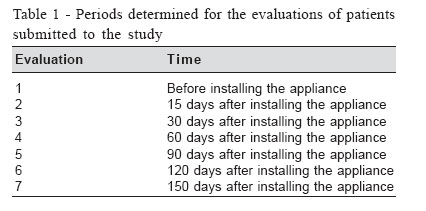
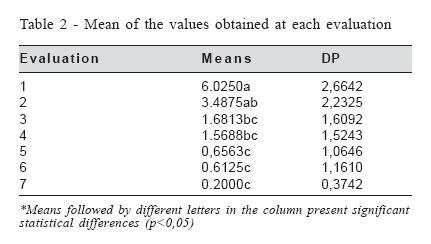
Brazilian Journal of Oral Sciences, Vol. 5, No. 19, October-December 2006, pp. 1244 -1248 Assessment of painful symptomology in patients with temporomandibular disorders by means of a combined experimental scale Giuliana Zanatta1* ,Wilkens Aurélio Buarque e Silva2* , Frederico Andrade e Silva2* , Guilherme da Gama Ramos1* , Henrique Casselli3* 1Master in Dental Prothesis Received for publication: March 13, 2006 Code Number: os06044 Abstract Quantification and assessment of the evolution of painful symptomology in patients with temporomandibular disorders, during the pre-, trans- and post-therapeutic stages is one of the greatest difficulties found by dental surgeons. Various authors have studied and discussed the use of verbal and non-verbal scales for this purpose. Therefore, this study aimed, by means of a combined experimental scale, to assess the evolution of painful symptomology in patients with completely edentulous maxilla and partly edentulous mandible, with Class I or Class II Kennedy prosthetic spaces, treated with flat occlusal appliances, before, during and after 150 of starting treatment. A selection was made of 16 patients with a mean age of fifty-two years, with signs and symptoms of temporomandibular disorders and diminished vertical occlusion dimension. The patients were submitted to treatment with flat occlusal appliances and fortnightly consultations for a period of 150 days. During these consultations, patients recorded their painful symptomology on a combined experimental pain scale. The results obtained were grouped into tables and submitted to the Friedman Test at a level of 5% probability. These revealed statistically significant differences between the values obtained at each assessment made. According to the methodology used and the results obtained, it was concluded that the therapy used was effective and that the experimental scale was efficient for registering the evolution of the symptoms initially detected. Key Words: temporomandibular disorders, occlusal appliances, pain, Class I or Class II Kennedy prosthetic, combined experimental scale Introduction When teeth are lost, a change occurs in the mandibular posture, the speech pattern, esthetics, and deglutition as well as in the individual's social, emotional and psychological behavior. The absence of posterior teeth has been described as an etiological factor of high prevalence in the functional alterations of the stomatognathic system1-,3. Therefore, treatment of patients with temporomandibular disorders (TMDs) is a challenge to the dental surgeon, more so when there is a need for prosthetic rehabilitation as a result of losing the posterior teeth. According to Weinberg4, Pameijer5, the first logical step towards rehabilitating patients that present with clinical signs that may suggest articular, muscular and occlusal changes, should be the optimization of the mandibular position, the muscular tonus and the occlusal pattern. The use of flat occlusal appliances enabled the elimination of occlusal interferences, a voluntary mandibular repositioning, synergic muscle contraction levels and decompression of the articular structures3,6-7. Feine et al.8, affirmed that it is common for the professional to question patients with regard to remembering his/her pain past and compare it to the trans- and post-therapy period. Many authors use patients' reports about pain relief as evidence of the efficiency of the therapeutic modality instituted. However, such relief or exacerbation reports do not necessarily reflect the efficacy of the therapy implemented, and are imprecise indicators of the true alterations in the state of pain, since they suffer from the distortions of the memory of it. In order for such problems to be avoided, such assessments should be founded on and recorded at the moment of the consultation, or as from the initial consultation. Many studies use verbal and non-verbal scales for this purpose9-11. Such researches very frequently use the visual analogical scale (VAS), and Numerical (NS), verbal (VS) and the Behavioral Scale (BRS). This study aimed to assess the evolution of the painful symptomatology by means of a combined experimental scale, in patients with temporomandibular disorders, treated with flat occlusal appliances for a period of 150 days, and whether the combined experimental scale used was capable of providing an efficient clinical assessment of the evolution of painful symptomology in patients, for the purpose of making a significant contribution to the clinical follow up of its evolution. Material and Methods Sample Selection A selection was made of sixteen patients (thirteen women and three men; aged 33-67 years, mean 52 years) from the Study and Treatment Center of Functional Alterations to the Stomatognathic System (CETASE) of the Piracicaba Dentistry Faculty UNICAMP. All of them presented with signs and symptoms of functional alterations to the stomatognathic system, had completely edentulous maxilla and partly edentulous mandibles, with the presence of Class I or II Kennedy prosthetic spaces; chronic, voluntary painful symptomatology and diminished vertical occlusion dimension. The volunteers signed terms of consent for the treatment and research, according to the Helsinki Declaration II, with the Dentistry Ethics Code (C.F.O. 179/93) and the National Health Council of the Ministry of Health Resolution No. 196, of 10/10/1996, approved by the FOP UNICAMP Ethics Committee on Research. Initially the volunteers were asked to reply to the questions on the clinical card of CETASE, FOP-UNICAMP, which includes personal data, spontaneous patient report with regard to the chief complaint, time of its duration and patient's expectations with regard to treatment. It also includes questions relative to sensitivity of TMAs, musculature and adjacent anatomical structures. Afterwards, patients were submitted to clinical and physical exams and asked to have radiographic exams done of the TMAs12 before and after treatment, with the object of assessing the positions of the condyles in relation to the mandibular fossas and articular tubercles and the anterior, posterior and superior intra-articular space in the maximum intercuspidation, opening and mandibular rest positions. Making of occlusal appliances The patients were submitted to therapy with flat occlusal cover appliances up to the period of 150 days of treatment. To make the appliances, molds were made of the top and bottom arches with alginate (JELTRATE- Dentsply Ind. E Com. Ltda) and the respective models poured with type IV plaster (HEROSTONE - Vigodent S. A. Ind. e Com.). Afterwards, these were mounted in a semi-adjustable articulator (BIO-ART Ind. Com. Ltda) with the help of a facial arch for mounting the top model and the record of the maximum intercuspidation position for mounting the bottom model. The models were mounted with the incisal pin of the articulator position on the zero marking. Afterwards, this pin was adjusted according to the patient's free functional space, previously measured with the help of a Willis Compass (GNATUS - Ind. Com. Ltda) to determine the height of the appliances to be waxed. The appliances were waxed on the top or bottom arch, taking into consideration for the choice, the stability of the appliances on the arches and the re-establishment of the occlusal plane, thus obtaining the largest possible number of occlusal contacts, without altering the flat configuration. Their inclusion was done in metal muffles (DCL, Ltda, Campinas SP - Brazil) and pressing was done with heat polymerizing acrylic resin (Artigos Odontológicos Clássico Ltda) by the conventional technique. After they were deflasked, they were finished and polished. Installing the appliances The appliances were installed firstly observing their seating and stability on the dental arch and next, by monitoring the distribution of the contacts between the occlusal surface of the appliance and the antagonist teeth. During the treatment period, patients were recommended only to remove the appliances for the three main meals. The patients were submitted to fortnightly consultations as from the installation of the appliances up to 150 days of treatment. At these consultations, adjustments were made to the appliances, so that stability was obtained on the dental arch and adequate bilateral distribution of the occlusal contacts without altering the flat configuration of the appliance. Experimental Scale The patients were asked to record their opinion about the painful symptomatology felt, on an experimental pain scale, before, during and at the end of treatment. The experimental scale consisted of the association of the visual analogical scale and numerical scale. (Figure 1). By means of this scale, patients could freely express their perceptions about the reproducibility of the painful symptomatology and consequently, their impression about the effectiveness of the therapy instituted. The patients were instructed to record their impressions with reference to occurrence and intensity of the pain, in the top and bottom square of the scale, with a vertical line. After being recorded, the distance between the left extremity (0) and the vertical line was measured with a millimetric ruler. Thus, the values obtained in each evaluation period were grouped in a table for later statistical analysis. Furthermore, at each evaluation made, information was obtained about the evolution of the signs and symptoms initially presented, by means of a clinical report from the patient based on the questions contained in the CETASE clinical record card, manifested positively in the previous sessions. The evaluation periods determined for this research are described in Table 1. Results The results obtained were grouped into tables and submitted to the Friedman Test at a level of 5% probability. The means for each evaluation period are set out in Table 2. The results obtained showed a reduction in the values recorded during the treatment period. The mean of the values from the first evaluation revealed statistically significant differences (p<0.05) in relation to subsequent evaluations, except for the second. The mean of the values for the second evaluation presented significant differences in relation to the values obtained in the last three. Discussion Innumerable authors defend the indication of occlusal appliances as the first step to help in diagnosis and control of painful symptomatology3,13. The assessment of the effectiveness of this type of device has commonly been clinically founded on the subjective quantification of the intensity and frequency of the signs and symptoms related and diagnosed before, during and after the treatment period. The results of this study show that at ninety days of treatment 56.25% of patients related remission of the initial symptomology. At one hundred and twenty and one hundred and fifty days of treatment, the absence of these symptoms attained 68.75% and 75% of the patients, respectively. These results confirm the studies of Zarb &Thompson14, Greene & Laskin15, Silva16 and Landulpho et al.17 With regard to time of treatment, the results showed that the period between one hundred and twenty and one hundred and fifty days was more effective than the one of ninety and one hundred and twenty days, longer than the period recommended by Silva7,16 and Landulpho et al.17.Probably, the profile of the selected patients contributed to this fact, all of them having edentulous top arches and Kennedy Class I or II prosthetic spaces in the bottom arch. Many of them related never having used prosthesis in the bottom arch and when they did have them, they had been used for over 10 years, favoring the appearance of signs and symptoms of temporomandibular dysfunction3,18, with patients relating it for a period of over seven years. Many authors have used patient records in pain quantification scales, as evidence of the efficacy of the therapy instituted19. Although many of them have been shown to be reliable and sensitive, there is no standard with regard to the subjective quantification of pain. However, there is general consensus that these scales should not generate additional expenses to the patient, they should be clearly understood, allow gradings and demonstrate reliability. Conti et al.10, in patients with chronic TMDs, studied the precision and sensitivity of the four scales most mentioned in literature for measuring pain: the visual analogical scale (VAS), numerical scale (NS), behavioral scale (BRS) and the verbal scale (VS). Their results allowed them to conclude that the numerical scale was shown to be the most precise of this analyzed. According to Kuttila et al.11, the scales were made up of the instruments most used for measuring the intensity of pain and among them, VAS provided satisfactory results in a simple, efficient and hardly invasive manner as far as the patients' personal problems were concerned. In the present study an experimental scale that associated VAS and NS was used. The association used in this study is characterized by adding only the initial "0" and final "10" values to the VAS scale. This procedure aimed to avoid growing numerical values, like the ones used in the NS. The value "0" corresponded to the reference of yellow coloring and the value "10" to red coloring. Growing numerical values may induce a memorization of the color reference and interfere in the recording of pain quantification, contributing to the increase in variability of records10. This association was also made by Price et al.20, who concluded that the numerical and analogical visual scales were consistent for measuring the clinical and experimental pain, but only VAS provided measurements of pain sensation intensity. During instructions to the patient, it was also opted to consider the value "0" as the absence of pain and the value "10" as the worst pain imaginable. Seymour et al.21, affirmed that the use of expressions that simplify the extremities of VAS provided an important referential for understanding it. The length of the scale used (10 cm) was also based on the opinions of this author, with the object of facilitating recording of the value obtained at each evaluation. In isolation, the two scales have positive aspects proved by various authors9,20-23. During the evaluations made in this study, patients had no difficulty in recording their impressions about the evolution of their painful symptomatology, allowing one to agree with Price et al.20 and Kuttila11, when they affirmed that the advantages of the combination between the numerical and visual analogical scales lay in the ease of their application and the possibility of using a simple instrument for gauging pain in clinical researches. It is considered that the use of scales for assessing the efficiency of the treatment of patients with temporomandibular disorders provides an extremely useful instrument, but they should not be used in isolation, as they may create questionable indicators for measuring chronic pain. The use of the experimental scale associated with the clinical and physical assessments seems to provide an important procedure for evaluating the efficiency of the therapy used. According to the methodology used and according to the results obtained, it may be concluded that: the experimental scale recorded a significant reduction of the signs and symptoms initially recorded; the experimental scale used allowed an efficient clinical assessment of the evolution of the painful symptomatology: the therapy used was shown to be effective. References
© Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil
The following images related to this document are available:Photo images[os06044t2.jpg] [os06044t1.jpg] [os06044f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}