 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 6, No. 20, January - March 2007, pp. 1260 - 1264 Correlation between marginal accuracy and fracture resistance of indirect composite restorations varying cavity preparation design Rodrigo Borges Fonseca1*,Hugo Lemes Carlo1* ,Alfredo Júlio Fernandes Neto2* ,Carlos José Soares1* 1Department of Operative Dentistry and
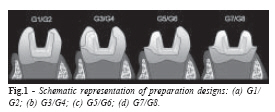
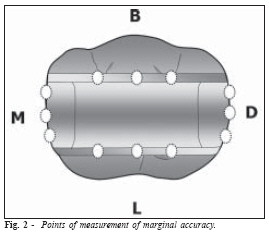
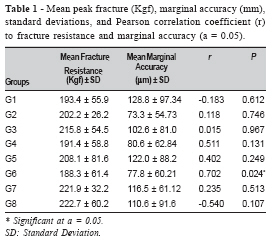
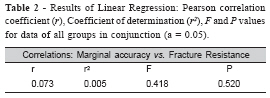
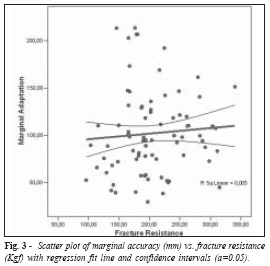
Dental Materials, Dental School Received for publication: November 14, 2006 Code Number: os07003 Abstract This study evaluated the correlation between marginal accuracy and fracture resistance of laboratory-processed resin composite (LPRC) restorations with different cavity preparation designs. Eighty human third mandibular molars were selected and divided into 8 groups (n=10): G1 conservative (-c) inlay; G2 extensive (-e) inlay; G3 onlay-c with mesio-buccal cusp coverage (CC); G4 onlay-e with mesio-buccal CC; G5 onlay-c with buccal CC; G6 onlay-e with buccal CC; G7 onlay-c with total CC; G8 onlay-e with total CC. Indirect composite restorations (SR Adoro, Ivoclar-Vivadent) were manufactured and positioned over each respective preparation. Marginal accuracy was assessed using a stereomicroscope at 3 points on buccal, lingual, mesial and distal regions (40x magnification). After adhesive cementation (Adper Single Bond 2 and Rely-X ARC, 3M ESPE) a load compressive test (0.5mm/minute) was performed. Data were recorded in mm (marginal accuracy) and Kgf (fracture resistance). In general, Pearson correlation coefficient (a=0.05) did not show significance between factors in study (r=0.073; p=0.520) but it showed significance only on G6 (r=0.702; p=0.024). Irrespective of the preparation design it seems difficult to state the clear correlation between marginal accuracy and fracture resistance of LPRC restored teeth. In this study the effect of one variable on another was negligible. Key Words: fracture resistance, marginal accuracy, correlation, composite inlays/onlays Introduction The last developments on adhesive dentistry have brought some great advantages on the treatment of weakened tooth structures. Materials and techniques are improved aiming to create a restoration that can mimic tooth substance, or better still regenerate tooth structure. Among currently available indirect restorative systems the second generation of laboratory-processed resin composites (LPRC) has been available since the early 1990s1. Several aspects of any restorative system require investigation but marginal accuracy seems to be of great importance due to its influence on the clinical longevity of restorations2-7. Plaque accumulation, gingival sucular fluid flow and bone loss, microleakage, recurrent caries, periodontal disease3,6-8, pulpal irritation and consequent sensivity9, marginal fracture and disintegration of the luting cement3,10-12 are some clinical disadvantages of poor adapted restorations. Leinfelder et al.6 have suggested as a general rule that the interfacial gap should not exceed 100µm, but some studies have shown gaps ranging from 0 to 200µm3,13. Furukawa et al.14 stated that within this gap range the effect of cement thickness on fracture resistance of LPRC restorations can be considered to be of little clinical importance, but their conclusion was based on a comparison between their results and the results from other studies. Cho et al.3 proved that as the occlusal convergence angles (6, 10 and 15 degrees) increases, the marginal accuracy and the fracture resistance of LPRC crows are negatively influenced. In addition, different finishing lines had an influence on marginal accuracy and fracture resistance of LPRC full crow restorations15. Irrespective of the cavity preparation design, it is a common finding to state that preparations weakens the tooth16-17 but the possibility of establishing good adhesion between teeth tissues and adhesive materials suggests the minor necessity to extend cavity preparations in order to prevent future tooth fracture18-20. It is hypothesized that indirect composite restorations for teeth with different cavity preparations could have a different influence on the correlation between marginal accuracy and fracture resistance. Then, if poor marginal accuracy could be correlated to low fracture resistance a careful attention should be spent before luting a new restoration. The purpose of this study was to evaluate the correlation between marginal accuracy and fracture resistance of LPRC restorations with different cavity preparation designs. The null hypothesis to be tested was that different cavity preparation designs have no effect on the correlation between marginal accuracy and fracture resistance of LPRC restored teeth. Material and Methods Eighty freshly extracted human third molars of similar size were selected for this study and divided into eight groups (n=10). Teeth were collected after patients had signed an informed consent, in accordance with the ethics committee of Federal University of Uberlândia, Brazil (protocol #029/2003). Calculus deposits and soft tissue were removed with a hand scaler and the teeth were stored in 0.2% thymol solution. The teeth roots were covered with a 0.3mm layer of a polyether impression material (Impregum F, 3M-ESPE, St Paul, MN, USA), to simulate the function of the periodontium, and embedded in a polystyrene resin up to 1mm below the enamel-cementum-junction to simulate the alveolar bone21. Teeth were divided into 8 groups (N=10): G1 - conservative (c-) inlay preparation; G2 - extensive (-e) inlay preparation; G3 c-onlay preparation with mesio-buccal cusp coverage; G4 e-onlay preparation with mesio-buccal cusp coverage; G5 c-onlay preparation with buccal cusps coverage; G6 e-onlay preparation with buccal cusps coverage; G7 c-onlay preparation with total cusps coverage; and G8 e-onlay- preparation with total cusps coverage. All teeth received standardized preparations with #3131 diamond burs (KG Soresen, São Paulo, Brazil) on a cavity preparation device so that all the cavities of a single group would have uniform dimensions. The cavity preparations were first named conservative or extensive, being that the occlusal isthmus width was the only difference between them (2.5 mm for conservative, and 5.0 mm for extensive ones). The teeth were prepared with the following standardized preparation criteria: a 6-degree axial wall taper, a 2.5-mm-deep occlusal isthmus and a 1.5-mmwide chamfer placed 1.5 mm cervical to the prepared occlusal pulpal wall, at proximal boxes. A 2.5-mm-occlusal reduction was defined from the top of each cusp and, on these groups, a 1.5-mmwide chamfer was placed 1.5 mm cervical to occlusal reduction. The proximal boxes were 1.5-mm-deep and their buccal-lingual interfacial distances (occlusal isthmus width) were prepared according to the experimental group: extensive (5.0mm) or conservative (2.5mm). Cavo-surface angles were approximately 90o and the internal angles were all rounded. Figure 1 shows the general types of cavity preparations for the different groups. One technician made all the restorations. A one stage impression was taken of each prepared tooth in a condensation silicon (Silon 2APS, Dentsply, Mildford, DE, USA) by use of a stock plastic tray, and poured with type IV stone (Durone IV, Dentsply, Mildford, DE, USA). Stone dies were isolated with SR Adoro Model Separator (Ivoclar-Vivadent, Schaan, Liechtenstein, Germany) before laboratory resin insertion. A die spacer was not used because it was suspected it could mask preparation irregularities. SR Adoro Liner 200 (Ivoclar-Vivadent, Schaan, Liechtenstein, Germany) was applied on a thin layer and then SR Adoro A3 were incrementally built up. Each layer were first pre-polymerized with an halogen light source (Targis Quick, Ivoclar 180 mW/cm2 at 10 mm distance) for 10 s and then, the final restoration was post-polymerized in a multi-focal halogen light source oven (Lumamat 100, Ivoclar-Vivadent, Schaan, Liechtenstein, Germany) with program 1 at 95oC and high light intensity for 25 min. After removing the restorations from stone dies it was necessary to perform internal adjustment for accurate seating4. The internal adjustment was accomplished by one operator with a low speed hand piece (Kavo, Joinville, Santa Catarina, Brazil) and #2131 diamond burs (KG Soresen, Barueri, Brazil). The internal surface of the restorations was 50 µm aluminum oxide sandblasted for 5 seconds, at a pressure of 4 bars and 2 cm of source-to-sample distance (Microjato Plus, Bio-Art, São Paulo, Brazil). After sandblasting, the interfacial distance of the restoration was assessed with a digital stereomicroscope (Model STN, Olympus, Tokyo, Japan) at 3 points on buccal, lingual, mesial and distal regions (Figure 2) with 40x magnification and 0.0005-mm accuracy resulting in 12 measurement points per tooth. The mean marginal accuracy for each tooth was obtained considering all measurement points together and then the mean for each group was calculated. A linear measurement was taken between the restoration and the cavo-surface-angle, after the restoration was set in place and stabilized with hueless glue (Tenaz, São Paulo, Brazil), at two points on occlusal margins7. The marginal accuracy, observed in linear measurement, was recorded at selected points with values expressed in microns (µm). After marginal accuracy assessment, the restorations were silaneted before cementation22. The preparations (enamel and dentin) were acid etched with 37% phosphoric acid for 15s, rinsed and blotted dried with a moist cotton pellet. The adhesive system Adper Single Bond 2 (3M-ESPE, St Paul, MN, USA) was applied to the preparation and left untouched for 20s, being light polymerized for 20s with an halogen light source, XL-3000, at an intensity of 800 mW/cm2 (3M-ESPE, St Paul, MN, USA). A dual-resinous cement, Rely-X ARC (3M-ESPE, St Paul, MN, USA), was mixed and applied to the internal surfaces of the restorations. The restoration was set in place under an occlusal load of 500grams for 5min, the excess cement removed with a brush, and light polymerized with XL-3000 from the mesio-buccal, mesio-lingual, disto-buccal, disto-lingual, and occlusal facial directions for 40 seconds in each direction. After bonding the teeth were stored in distilled water at 37oC in a dark container for 24h prior to testing. Teeth were then submitted to a compressive load on a testing machine (Emic DL-2000, EMIC, São José dos Pinhais, PR, Brazil) with a 6.0mm sphere contacting the center of the occlusal surface, at a crosshead speed of 0.5 mm/min. The compressive load at fracture (Kgf) was recorded for each specimen. Statistical analysis of the correlation between fracture resistance and marginal accuracy was performed using Minitab 14 statistical software (Minitab Corporation, State College, PA, USA) and SPSS 12.0 for Windows (SPSS Inc., Chicago, USA). The Pearson correlation coefficient (r) (p<0.05) was calculated for each experimental group and for the data of all groups in conjunction. The Coefficient of Determination (r2), which is the ratio of the explained variation to the total variation, was calculated for the data of all groups in conjunction. Linear Regression was computed, in order to clarify the correlation between factors in study, by means of a scatter plot with a regression fit line and confidence intervals (a=0.05). Results Table 1 shows the mean fracture resistance (Kgf), marginal accuracy (mm), standard deviations, Pearson correlation coefficient (r) of the groups and P associated values. All recorded data were checked for test distribution with the Anderson-Darling test (p<0.05) which revealed normal test distribution for all groups. Pearson correlation coefficient showed significance only on G6 (r=0.702; p=0.024). Then, the null hypothesis had to be rejected to all groups but not to G6. This fact means that, in general, the marginal accuracy of LPRC restorations seems to be poorly correlated to their fracture resistance. Table 2 shows the results of Linear Regression: Pearson correlation coefficient (r), Coefficient of determination (r2), F and P values for data of all groups in conjunction. It can be noted that the "r" value (r=0.073) is too close to 0, what means that the correlation of marginal accuracy and fracture resistance is weak enough to be significant (p=0.520). Figure 3 depicts a scatter plot with a regression fit line and confidence intervals (a=0.05). Few data points are close to the regression fit line and inside the lines representing the confidence intervals. The fit line represents the trend of the data and the space between the confidence intervals lines shows the data points which more adhere to this trend; it could be seen a small number of collected data points demonstrating a relationship (r=0.073) between marginal accuracy and fracture resistance. Discussion Several factors are believed to affect the marginal accuracy and fracture resistance of laboratory-processed resin composite restorations. For the former, scientific reports list the influence of luting agent type23-24, modulus of elasticity of the supporting structure, surface roughness, residual stress, restoration thickness3, properties of the restorative material24, manufacturing conditions of the restoration18, the employment of an adhesive technique7,14,16,18-19,23-25 and the preparation design3,7,15-16. Affecting marginal accuracy are the location of cavity margins, use of incremental placement techniques, restorative material type and methods of activation, the usage of liners and finishing methods26. In spite of the fact that some studies have investigated the influence of these factors both on marginal accuracy and fracture resistance of LPRC restorations3,13,15,19 none of them have established the relationship of these variables. Then, this study evaluated the correlation between marginal accuracy and fracture resistance of LPRC restorations with different cavity preparation designs. Cho et al.3 have demonstrated that as the occlusal convergence angles (6, 10 and 15 degrees) increases, the marginal accuracy and the fracture resistance of LPRC crows is negatively influenced. Thus, it means that when a cavity preparation results on poor marginal accuracy it is expected a negative influence on fracture resistance as well. Although this conclusion seems reasonable, Furukawa et al.14 showed that when an adhesive technique is successfully employed on the cementation of indirect composite restorations clinical gaps that normally range from 0 to 200µm do not significantly affect fracture resistance. In agreement with Furukawa et al.14 this study showed that there is no significant correlation (r=0.073 and p=0.520; Figure 3) between marginal accuracy and fracture resistance in gaps that ranged from 73.3µm to 128.8µm (mean values). The square of the r coefficient is called coefficient of determination (r2) and it is known to be the ratio of the explained variation to the total variation. Thus, considering that in this study r2=0.005, from a statistical point of view it means that just 0.5% of the variation of marginal accuracy can be explained by the relationship between marginal accuracy and fracture resistance27. The remaining 99.5% of the variation is unexplained and is due to chance or other factors. When it is considered the several types of preparation designs used on this study, G6 was the only one where a significant and positive correlation could be found (r=0.702; p=0.024). In fact, this occurrence seems not usual since one would expect that poor marginal accuracy is associated to good fracture resistance. If the coefficient of determination of this group was calculated it would return r2=0.499, and this mean that half (49.9%) of the variation on marginal accuracy can be explained by the relationship between this factor and fracture resistance, but for sure several other factors (50.1%) can have an influence. A mean gap of 77.8µm was observed on this group, and according to Furukawa et al.14 it is not probable that on a clinical situation it would have any influence on fracture resistance of indirect composite restorations. Several other factors may affect both variables and this makes difficult to establish a clear relationship. Mehl et al.28 studied different wall thicknesses for inlay preparations restored with ceramic or composites, showing that ceramic inlays provide significantly greater stabilization and better marginal quality than do composite inlays, but in the case of very thin remaining walls (about 1.3 mm), however, the marginal quality and the cusp-stabilizing effect are reduced. Then, similar to this study, it can be seen that preparation design can influence both marginal discrepancy and fracture resistance but it seems difficult to predict the exact influence of these parameters on each other. Studying the effect of finish line variants on marginal accuracy and fracture resistance of Targis/Vectris crowns, Cho et al.15 showed that crowns with a shoulder finish line showed a smaller marginal discrepancy than those with a chamfer finish line, but the fracture resistance of the crowns with a chamfer finish line was higher than that of the crowns with a shoulder finish line. Thus, marginal accuracy and fracture resistance had an opposite behavior. Again, this fact stresses the difficulties in establishing a clear relationship between these variables. On the present study it was only employed a chamfer finish line but the variation in preparation design between groups did not significantly influenced the correlation of these variables, except for G6. The results of this study are only indicative that at least from the perspective of an in vitro simulated clinical situation there is no correlation between marginal accuracy and fracture resistance for laboratory-processed resin composite restorations. For sure, several other factors must be studied in order to address a stronger conclusion and definite reasonable clinical guidelines. Further studies, especially clinical observations, are necessary to address stronger conclusions. In accordance with the methodology developed in this study it is possible to conclude that marginal accuracy and fracture resistance do not have a significant correlation to each other. Only for one group where teeth received an extensive onlay preparation with buccal cusps coverage (G6) it was observed a positive significant correlation. Acknowledgements Authors are grateful to Dentsply and KG Sorensen for full donation of the materials used in this study, and to Ivoclar-Vivadent and 3M-ESPE for partial donation. References
© Copyright 2007 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os07003f1.jpg] [os07003f3.jpg] [os07003f2.jpg] [os07003t1.jpg] [os07003t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}