 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
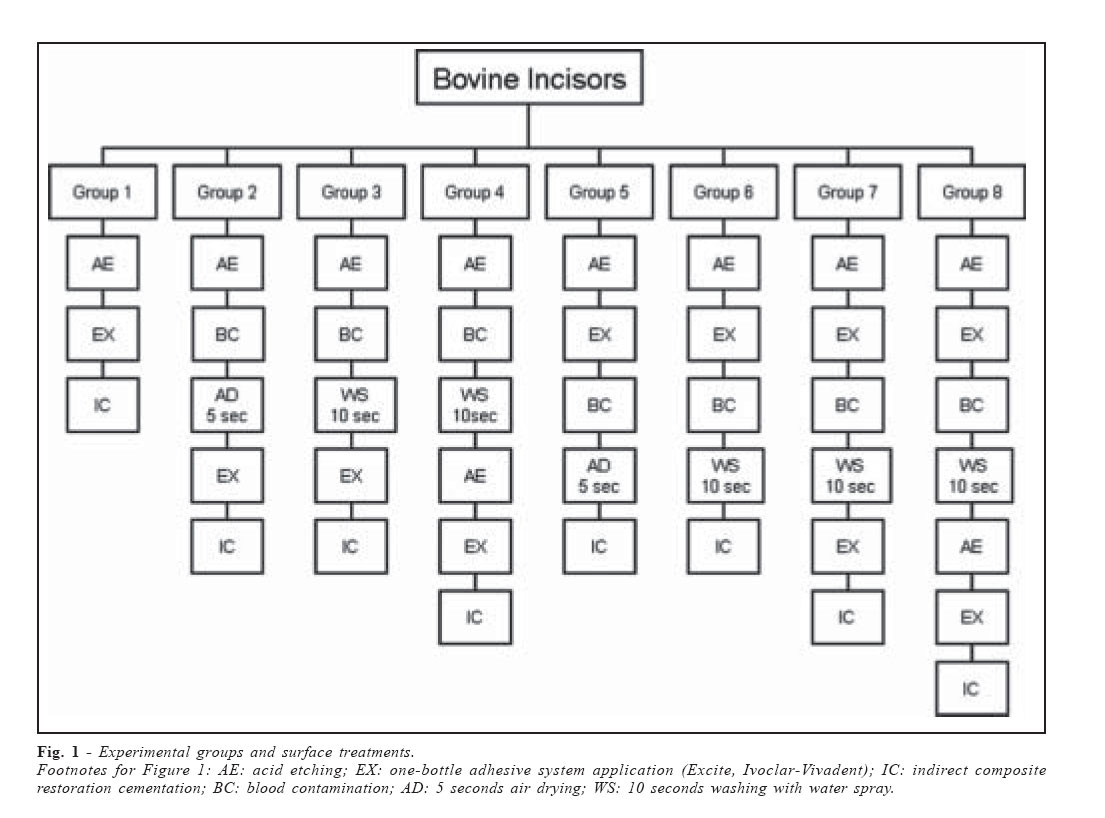
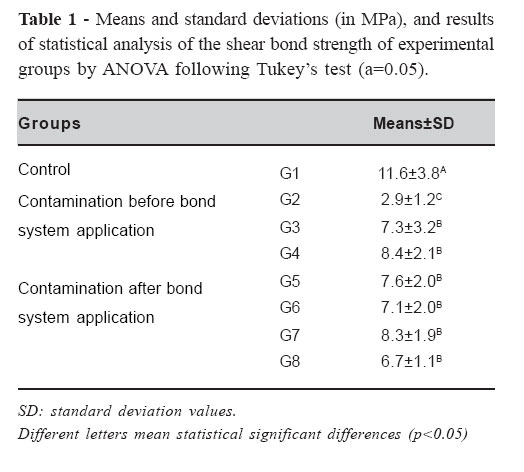
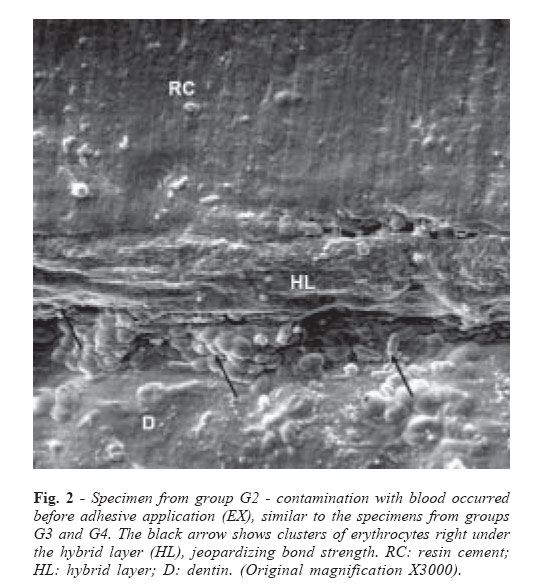
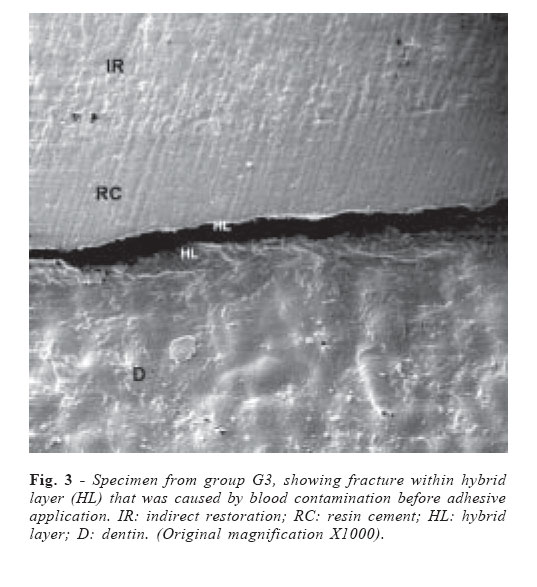
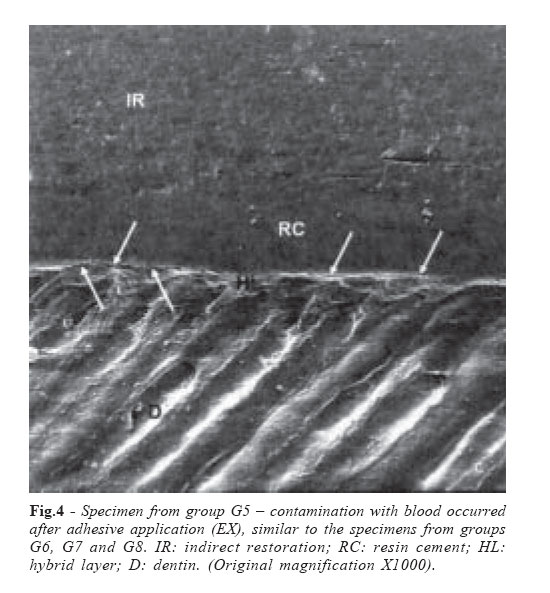
Brazilian Journal of Oral Sciences, Vol. 6, No. 21, April - June 2007, pp. 1320 - 1325 Effect of blood contamination during adhesive restorative procedures on dentin-resin cement shear bond strength Carlos José Soares1, Carolina Assaf Branco2, Priscilla Barbosa Ferreira Soares1, Rodrigo Borges Fonseca1, Hugo Lemes Carlo1, Alfredo Júlio Fernandes Neto2 1Department of Operative Dentistry and Dental Materials, Dental School - Federal University of Uberlândia. Correspondence to: Carlos José Soares Universidade Federal de Uberlândia – Faculdade de Odontologia Departamento de Dentística e Materiais Odontológicos Av. Pará, nº 1720, Bloco 2B, Sala 2B-24, CEP 38405-902 Uberlândia – Minas Gerais – Brazil Phone: +55-34-32182255 Fax: +55-34-32182279 E-mail: carlosjsoares@umuarama.ufu.br Received for publication: November 14, 2006 Code Number: os07014 Abstract The aim of this study was to evaluate the effect of dentin blood contamination during different steps of the restorative procedure on resin cement shear bond strength to dentin. Crows of 120 bovine incisors were prepared to obtain flat superficial dentin surfaces. Dentin was etched with phosphoric acid and contaminated with fresh blood for 10 seconds, before or after adhesive system application. Different treatments were tested in contaminated dentin, resulting on eight groups (N=15). Composite resin restorations (TPH Spectrum, Dentsply) were adhesively fixed (Excite, Ivoclar-Vivadent) with resin cement (Variolink 2, Ivoclar-Vivadent) and shear bond strength test (0.5 mm/min) was performed. Morphologic observations were carried out with scanning electron microscopy (SEM). Data (MPa) were submitted to one-way ANOVA following Tukey’s test (p<0.05), showing that blood contamination during adhesive procedure negatively affects bond strength, and decontamination methods do not recover original bond strength. The negative effects of blood contamination on shear bond strength to dentin and resin cement were significant in all contaminated groups; none of the tested dentin treatment procedures resulted in higher bond strength irrespective of the moment on which blood contamination took place. Key Words: blood contamination, adhesive system, dentin bonding, indirect restoration, shear bond strength IntroductionStable adhesion between resin composite and tooth structure is essential for the clinical success of restorations1. The creation of stable resin-dentin bonds relies on the formation of a hybrid layer that consists of partially or completely demineralized dentin and well-infiltrated, well-polymerized resins2. Achieving a good moisture control is essential to avoid any contamination during the adhesive procedure, but this is a common problem in restorative dentistry, especially when rubber dam isolation is not feasible3. Many carious lesions, which require the use of dentin bonding agents, are located on areas that are difficult to isolate and, therefore, dentin contamination with blood may occur. Blood contamination of the adhesive surfaces may affect the bond strengths of adhesive resins3-7. Recent studies have evaluated the effect of blood contamination of adhesives to dentin using different testing methods6-9, showing a significant reduction in bond strength values. Shear and microtensile tests are the most common methods used for determining the bond strengths of adhesive systems, revealing valuable clinical information10. The negative effect of blood on adhesion can be attributed to its high protein content (6-7%)8. The high protein content together with macromolecules as fibrinogen and platelets, can form a thin film on the dentin surface and prevent adhesive infiltration8. On the other hand, if contamination occurs on previous infiltrated dentin, the interaction between adhesive system and resin cement will be affected6. Regardless the time of blood contamination (before or after the adhesive application), different decontamination procedures have been used on contaminated dentin to recovery the original bond strength values6,8, but literature is still contradictory. Some studies show that decontamination procedures can recover bond strength6,9, but others show the contrary7. Then, it seems possible that contaminant-removing treatments after blood contamination could increase the bond strength. A re-etching, water rinsing or adhesive reapplication are some of these techniques3,6,8. The purpose of this study was to evaluate the effect of blood contamination at different steps during the restorative procedure on the shear bond strength between dentin and resin cement, and to determine the best decontamination method to re-establish the original resin-dentin bond strength. The null hypothesis tested was that different treatments of the blood contaminated dentin do not affect the bond strength. Material and MethodsOne hundred and twenty freshly bovine mandibular incisors extracted from two-to-three year old cattle were stored in thymol 0.2% at 4oC for up to two weeks and randomly assigned to eight groups (N=15). The roots of the teeth were cut-off with a double faced diamond disk (KG Sorensen, Barueri, Brazil) and any tissue remnant and debris were removed. The crowns were then mounted in a cylinder with self-curing polystyrene resin (Cromex, Piracicaba, Brazil) and their labial surface was ground with wet 180-, 320- and 600-grit SiC abrasive paper (Norton Abrasivos, Campinas, Brazil) in order to obtain flat superficial dentin surfaces and to produce a standardized smear layer. An adhesive tape with a 3mm central perforation was positioned on the flat dentin surface to demarcate the bonding area. This methodology ensured a standardized measurement of the bonding area, facilitating the obtainment of accurate bond strength values. A condensation silicone (Zeta Plus and Oral Wash, Zhermack, Italy) was used to take an impression of a metallic cylinder (3x3mm), and after polymerization the cylinder was removed and the impression used to build indirect composite restorations. The composite resin (TPH Spectrum, Dentsply, Milford, USA) was inserted in three increments and light-polymerized for 40 seconds with a conventional halogen light curing unit XL 2500 - 600mW/cm2 (3M-ESPE, St. Paul, USA); then, samples were post-polymerized in a autoclave at 110ºC for 15 minutes. Dentin was etched with phosphoric acid (35%; Ivoclar-Vivadent, Schaan, Liechtenstein) for 15 seconds, copiously washed for 30 seconds and excess of water removed with an tissue paper (Snack, Melhoramentos Papéis Ltda, Caieiras, Brazil). In accordance with the ethics committee of Federal University of Uberlândia, Brazil, human blood was collected from one volunteer and immediately used. Blood was dropped to contaminate the dentin surface for 10 seconds, before or after adhesive system application. Different protocols were tested due to blood contamination before or after adhesive application, resulting in eight groups (Figure 1): G1 (control): after acid etching (AE), an one-bottle adhesive system (Excite, Ivoclar-Vivadent) (EX) was applied with a disposable brush, left untouched for 20s, re-applied and light-cured for 20s, and the indirect composite restoration (IC) was fixed with a resinous cement (Variolink 2, Ivoclar-Vivadent); in G2, G3 and G4 contamination occurred before adhesive application: G2: after AE, blood contamination (BC) was carried out by drooping blood from a capillary tube on all exposed dentin surface, followed by air drying for 5 seconds (AD), EX, and IC; G3: AE, BC, water spray washing for 10 seconds (WS), EX and IC; G4: AE, BC, WS, AE, EX and IC; in groups G5, G6, G7 and G8 contamination occurred after adhesive application: G5: AE, EX, BC, AD and IC; G6: AE, EX, BC, WS and IC; G7: AE, EX, BC, WS, EX and IC; G8: AE, EX, BC, WS, AE, EX and IC. Restorations were fixed with a dual-cure resinous cement (Variolink 2, Ivoclar-Vivadent) under 500g of load and lightcured in two opposite directions for 40s. Samples were stored in distilled water at 37ºC immediately after bonding, for 24hs, and then a shear bond test was conducted in a Testing Machine (EMIC DL 2000, São José dos Pinhais, Brazil) at a crosshead speed of 0.5mm/minute. The knife-edge chisel was applied parallel to the dentin surface with a source-to-sample distance of approximately 0.2mm, and perpendicular to the composite restoration. Shear bond strength was calculated by dividing the ultimate load (N) by the bonded surface area (mm²). Two samples of each group were prepared for SEM evaluation. Specimens were soaked in 6 mol/L HCl for 5s, followed by immersion in 5% sodium hypochlorite for 5 min, dehydrated in ascending concentrations of ethanol (50% for 10 min; 70% for 10 min; 95% for 10 min; and 100% for 30 min) and fixed in 2.5% glutaraldehyde. Thereafter, the specimens were gold sputter-coated and observed at the SEM (Zeiss DSM 940 A, Germany). Data was analyzed by one-way ANOVA, followed by Tukey’s multiple comparisons test with a 5% level of significance. ResultsMean shear bond strength values were expressed in MPa. Data presented a normal and homogeneous distribution, which enabled parametric analysis. One-way ANOVA revealed that there was a significant difference on the bond strength of the different groups (Table 1). There was a significant decrease in bond strength due to blood contamination, regardless the cementation protocol used for each group. There was no statistical difference between contaminated groups, except when the blood contamination was followed by air spray and adhesive application (G2), resulting in the lowest bond strength mean. SEM evaluation showed the presence of erythrocytes within partially infiltrated dentin (Figure 2) and adhesive failures between dentin and adhesive system (Figure 3) or between adhesive system and resin cement (Figure 4). Discussion Blood contamination is a major clinical problem during restorative dental treatment8. Kaneshima et al.6 stated that the effects of blood contamination on bond strength of adhesive resin to dentin may vary greatly depending on the adherent surface conditions. According to basic concepts of adhesion, the closer the contact between the adhesive and the adherent, the stronger is their junction11. Therefore, the contaminated layer may become a strong mechanical inhibitor of adhesion, preventing both adhesive system infiltration and polymerization, thus adversely affecting its bonding with the resin cement6. Dental surface contamination can occur at two critical times during the bonding procedure: after the tooth surface had been etched (Figures 2 and 3) and/or after the adhesive system had been applied (Figure 4). As a result, bonding can be compromised at both times. In this study, the negative effects of blood contamination on shear bond strength to dentin and resin cement were significant in all contaminated groups. Previous studies showed a decrease on shear bond strength when blood contamination occurred before the adhesive system application6,8. Blood residues or reactants obstructing the dentin tubules can inhibit primer infiltration into dentin6,8, thus interfering with hybrid layer formation. Figure 2 shows the presence of erythrocytes right below the hybrid layer, which seems to be responsible for failures within the hybrid layer, as seen in Figure 3. In this study, blood air drying after contamination (G2) caused a catastrophic decrease in bond strength between the adhesive and dentin, which is in agreement with previous published results6,8. Similarly to Kaneshima et al.6 when the blood was applied and just dried on the surface, a great number of blood residues were observed on dentin surface (Figure 2). This situation might have left more blood contaminants on dentin surface and also caused collagen fibrils to collapse, preventing adhesive monomers to infiltrate12. The blood protein components trapped on the dentin surface interferes with the bonding agent ability to form a uniform surface coating3,8. According to Abdalla et al.8 resin tags formed on air-dried dentin surfaces were found to be fewer and much shorter than that in control conditions and blood contamination prevents adhesive infiltration into dentin tubules. In spite of the fact that most of dentin bond strength is due to resin infiltration in intertubular dentin12, the absence of tag formation can be interpreted as a direct result of the presence of contaminants which would also jeopardize infiltration into collagen fibrils reducing bond strength, as seen in this study. Then, the use of air drying on contaminated dentin, before adhesive application, should be avoided. Water spray (WS) after dentin contamination increased bond strength (G3) to the same level that when WS was followed by re-etching (G4). In a study by Xie et al.9 plasma contamination lowered bond strengths by 33 – 70% for both enamel and dentin, but re-etching restored bond strength. In this study the use of blood instead of just plasma contamination showed that dentin re-etching did not improve bond strength. Then, in this situation re-etching should be avoided because a severe dentin decalcification can denature collagen fibrils1, and there is not a significant increase in bond strength. The use of an organic solvent on the contaminated surface to re-establish the capacity of formation of the hybrid layer seems to be a good alternative in cases of blood contamination. Kaneshima et al.6 found reduced bond strength unless the most superficial layer (exposed collagen fibrils) was removed from the surface, before or after blood contamination, with hypochlorite solution6,13. They concluded that large blood corpuscle elements could have been completely rinsed away; then the adverse interaction between the exposed collagen meshwork and the blood protein components that could inhibit primer infiltration into dentin was eliminated. The removal of surface collagen fibrils eliminates the creation of a hybrid layer and can produce high bond strength by the closer contact between adhesives and dentin14 but collagen impregnation and the formation of high quality hybrid layers are still regarded as the main mechanism of dentin adhesion15. When blood contamination occurs after adhesive application the interaction between adhesive system and resin can be jeopardized6. Eiriksson et al.3 evaluated the effects of blood contamination on resin-resin interfaces showing that blood protein components were not able to be completely rinsed away by water spray, lowering the surface energy of the cured composite. They concluded that the application of a more fluid adhesive layer significantly increased the resin-resin bond strength. In the present study, irrespective of the cementation procedure, when blood contamination occurred after adhesive system application, a new adhesive layer (G7 and G8) did not result on higher bond strength, probably because blood protein components still impaired an effective adhesive interaction. Figure 4 shows failure right above the hybrid layer as a signal of blood contamination after adhesive application. In spite of the fact that no significant differences were found between G8 and the other contaminated groups, except G2, the mean shear bond strength of G8 was relatively lower when compared to the other treatments. In this group, blood contamination occurred after adhesive system application, and it was followed by water spray, re-etching and application of a new adhesive layer. Re-etching either seemed not able to clean the surface or it could also have made this surface more acidic causing an adverse surface interaction16. The new etching over previous polymerized adhesive layer was rinsed off by water spray for 10s, but if any remnant of the phosphoric acid was still present it could react with the adhesive system tertiary amine initiator thus interfering with the polymerization of the new adhesive layer16. This occurrence may be the cause for G8 having lower, but not significant, bond strength than G7, where a new adhesive layer was applied but it was not preceded by re-etching. Further studies are necessary to confirm this hypothesis. The bond strength reported in this study when blood contamination occurred after adhesive system application was substantially lower than those reported in previous investigations3,6,8,13. However, published researches that deal with the effects of blood contamination on adhesive restorations are limited and comparisons are difficult. These differences in results between studies may especially be due to variations in interpretation of what constitutes a contaminated dentin surface8, and the bond strength test used17-18. In addition, several variables have been identified to influence the results of bond strength measurements, including bonding systems, type of substrate, type of blood fresh or anticoagulated19, the origin and condition of the dentin substrate, the etching, priming and bonding procedures and storage of the specimens. Few researchers had used freshly drawn blood3,6,8,20, as in this study. Dietrich et al.19 found significantly higher percentages of marginal openings after contamination with fresh capillary blood compared to anticoagulated blood. Another important point is the bond strength test used on each research. Each test keeps its advantages and limitations in determining the significance of the results obtained. Hence, comparisons among studies are difficult because a variety of tests, and are not always feasible. If different tests are used, it seems difficult to compare and draw conclusions with data gathered from different studies10. The shear bond strength test used in this study is an extensively used test4-5,8,21-22 and it has been one of the most common laboratory techniques for evaluating adhesives on resin-bonded restorations17. For sure, testing adhesion with shear bond strength may not be the most specific method17 but shear represents a destructive force which occurs in almost all restorations in clinical function, due to a complex stress distribution of bite forces23. In spite of the limitations imposed by this method, its direct association with what happens in real situations may be the reason for many researchers still use it. The results from the present study clearly indicated that, when the dentin surface was contaminated either before or after application of the adhesive system, any of the cementation protocols recovered the bond strength to the level of the control group. It is likely that contaminants may have remained on the dentin surface, thus interfering with the formation of a hybrid layer or inhibiting the bonding of adhesive system to resin cement. Therefore, the most important factor for ensuring optimal bonding is to avoid blood contamination. However, furthers studies varying the conditions, specially the laboratory technique and the adhesive system, are necessary for definitive conclusions. AcknowledgementsAuthors are grateful to Ivoclar-Vivadent and Dentsply for partial donation of the materials used in this study. The authors have no financial interest in any of the products mentioned in this article. References
© Copyright 2007 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os07014f3.jpg] [os07014f1.jpg] [os07014f2.jpg] [os07014t1.jpg] [os07014f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}