 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 6, No. 21, April - June 2007, pp. 1357 - 1363 Aesthetic resources in rehabilitation with implant-supported restoration inthe anterior region: a clinical case Paulo Roberto R. Ventura1, Adalberto Bastos de Vasconcelos2 1Specialist in Dental Prosthesis, ABO-RJ -Major in
charge of the Service of Implantology of the 1st
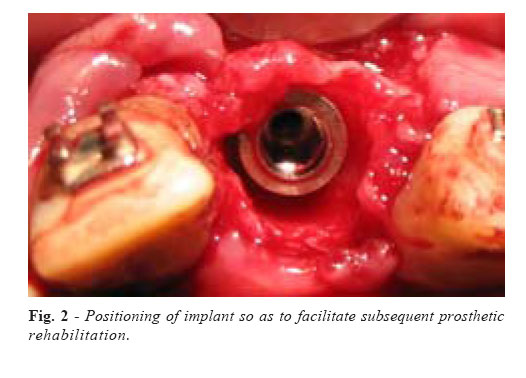
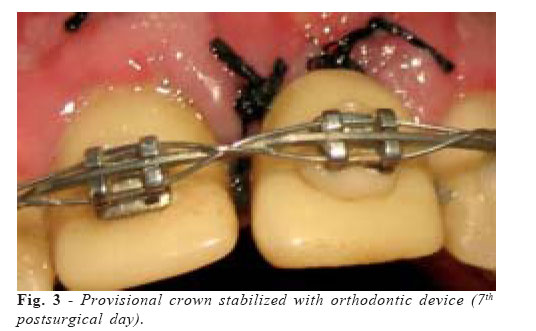
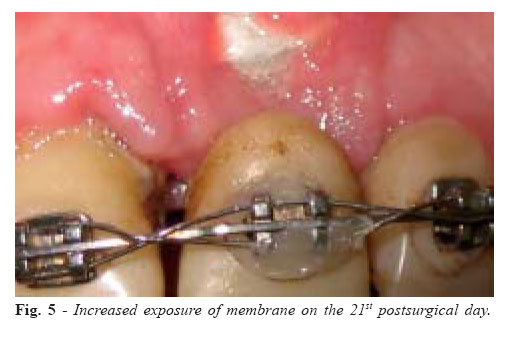
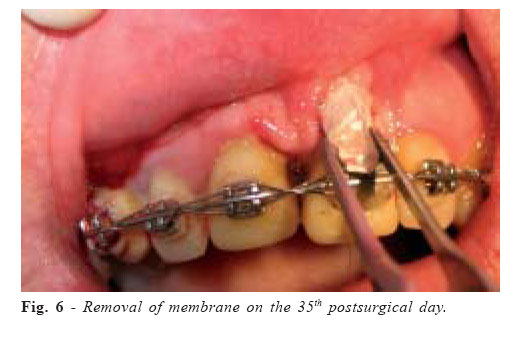
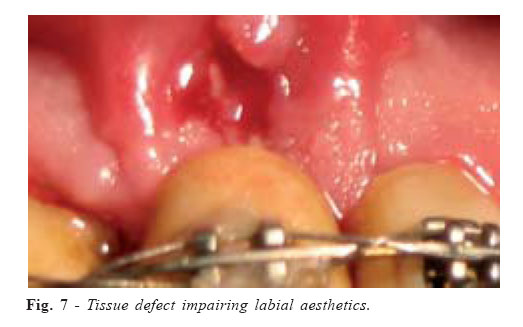
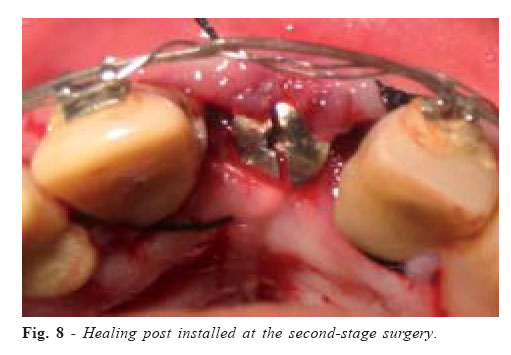
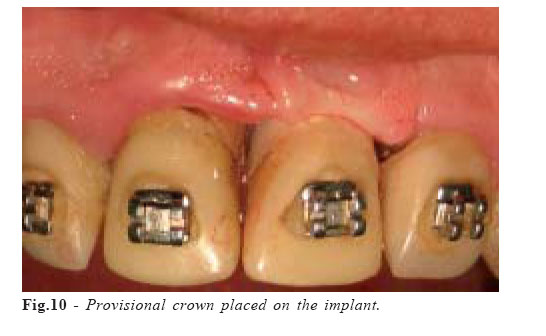
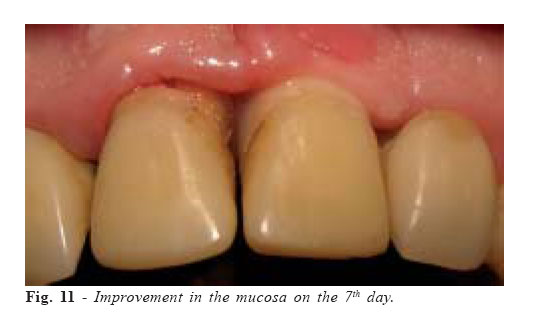
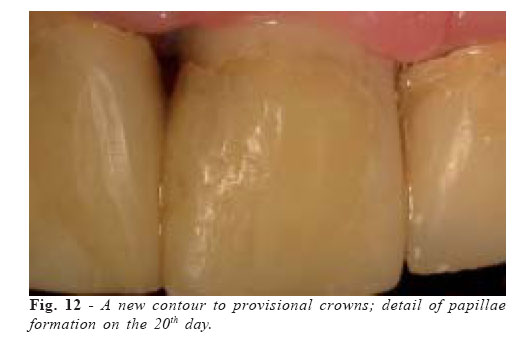
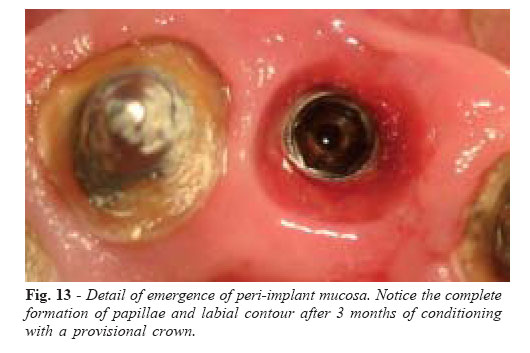
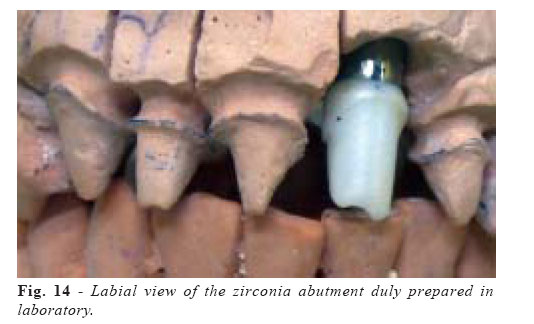
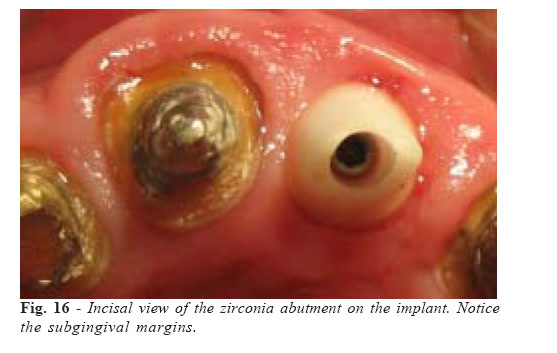
Dental Office of CBMERJ- Rio de Janeiro Correspondence to: Paulo Roberto R. Ventura Presidente Domiciano Street, 164 Ingá, Niterói – RJ/Brazil E-mail: pauloventura@uol.com.br Received for publication: March 04, 2007 Code Number: os07021 Abstract Achieving aesthetic satisfaction in anterior teeth rehabilitation is a constant challenge to clinicians. Modern implantology is an invaluable tool to replace missing teeth; however, it requires carefully determined steps in each rehabilitation stage, from implant placement of the implant-supported crown. This article aims at reporting the several resources employed in a clinical case that should always be used in rehabilitation with single implant-supported crowns in the maxillary anterior area. Key Words: implants, aesthetic, implant-supported crown, ceramics, zirconia Introduction With the advent of osseointegrated implantology, oral rehabilitation has acquired a new tool to replace missing teeth. However, the search for optimal aesthetics has been another great challenge in this field, mainly when there are losses in the maxillary anterior region. Today, we know that not only the prosthetic crown, but also the way it relates with the implant and the adjacent tissue are key factors to achieve excellent copies of natural teeth. For this purpose, it is necessary to devise interdependent prosthetic and surgical plans, in which the final aesthetics begins with the observance of implant position at the moment of installation and goes to the correct choice of the prosthetic restoration type. We have to consider that, when a tooth is lost, there is a collapse of the hard and soft tissues in the region. A change in the bone architecture will determine, in the remaining soft tissue, a complete loss or considerable decrease in the height of proximal papillae, as well as the disappearance of the cervical contour associated to labial concavity. Preventing such losses or giving back to those structures their appropriate framework, by means of surgical and prosthetic techniques, is characterized today as a protocol to be followed. The labiolingual relation with the bone wall and the mesiodistal relation with the neighboring teeth or other implant will favor the formation of new papillae. Implant inclination, following the long axis of the future crown, will make possible the correct emergence profile of this coronal restoration, acting as a support for the cervical and labial contour of the mucosa. The manipulation of peri-implant soft tissue, from the placement of a provisional crown to the installation of the permanent one, offering adequate proximal contacts, also determines the reformation of papillae. The advance of fully metal-free restorations and intermediate ceramic abutments has provided enough resistance, improved the translucency of the crown, and prevented the metal from showing through the soft tissue in the cervical area. This article aims at reporting several scientifically proved criteria adopted in a clinical case that should be met to achieve a satisfactory aesthetic solution in rehabilitation with single implant-supported crowns in the anterior region. Clinical CaseMale patient, 38 years old, with deficient single anterosuperior crowns, whose tooth 21 showed a fistula and had an unfavorable prognosis due to root fracture. After the necessary clinical, radiographic, and laboratory procedures, we extracted the tooth and installed immediately an osseointegrable implant of 4.3 X 13 mm (“Conect Cônico” by Conexão Sistemas de Prótese, São Paulo, SP/Brazil) to restore both damaged function and aesthetics (Figures 1 and 2). On exploring the socket, we found a labial fenestration related to the region of the fractured root, and used a deproteinized cortical bovine bone graft (“GenOx Inorg” by Baumer, Mogi Mirim, SP/Brazil), supported by a non-resorbable membrane, to fill both the labial defect and the gap between socket and implant. Then, we opted for placing a provisional crown with no immediate load, retained by an orthodontic device (Figure 3). The gradual exposure of the membrane produced an aesthetic defect in the labial mucosa (Figures 4, 5, 6, and 7). After the osseointegration period, we carried out the secondstage implant surgery and placed a healing to restore the mucosa in this first healing stage (Figure 8). Only 28 days later we installed the abutment and placed the provisional crown on the implant (Figures 9 and 10). New and gradual contours, associated to the reestablishment of proximal contact points, were implemented to provisional crowns to provide adequate support to the soft tissue and to induce the formation of interdental papillae (Figures 11 and 12). After waiting for three months for the physical aspect of the mucosa to stabilize (Figure 13), we made a custom molding to start the final prosthetic stage. Taking the thickness of the peri-implant soft tissue into account, we decided to use a zirconia prosthetic abutment (Conexão Sistemas de Prótese, São Paulo/Brazil – Figures 14, 15 and 16) to receive a fully metal-free restoration. Thus, we avoided a possible darkening in the cervical region, which could impair aesthetics as a whole. DiscussionReplacement of missing teeth by osseointegrated implants has increasingly become a safe treatment choice. However, in the case of aesthetic regions, mainly in the maxillary anterior area, several criteria must be met. Planning in implantology does not allow for a complete independence between the surgical and the prosthetic stages. Both the surgeon and the prosthetist share responsibilities, and should take jointly planned steps to achieve a satisfactory aesthetic result. The aesthetics of an implant-supported restoration depends not only on the quality of the coronal prosthesis, but also on its relation with the adjacent hard and soft tissues. Errors meeting these criteria are the most common barriers to achieve gingival symmetry around the implant-supported restoration. Cardapoli, Lekholm and Wennström1 evaluated clinically dimensional alterations in peri-implant tissues of single restorations during one year after loading, and observed a bone and soft tissue remodeling that may affect the aesthetics of the restorative therapy. Bone crest, soft tissue thickness, cervical contour, interproximal papillae, and their relations with the crown are factors to be considered to achieve an anatomically natural look. Such is the importance given to these factors that Meijer et al.1 proposed an index for rating aesthetics of single implantsupported crowns, based on anatomic form, color, and surface characteristics of restorations and of peri-implant soft tissue. The collapse of the bone tissue after tooth extraction can be an inconvenience in the surgical installation of implants and also in the peri-implant inter-relations. Several authors agree that it is important to preserve bone architecture. Berglundh and Lindhe2 showed in studies with dogs that filling bone defects with mineralized bovine bone led to a neoformation in the region around the implant after 3 to 7 months of observation. Many authors also agree that an implant placed immediately after tooth extraction preserves better the original characteristics of neighboring tissues, although the bone remolding process around an implant installed in a socket is different from the one that occurs in the cicatrized bone crest (Botticelli et al.)3-4. However, in a more recent study in humans, with clinical and radiographic evaluation at 1-year longitudinal follow-up, Juodzbalys and Wang5 described 100% of success and aesthetic result in the installation of immediate implants with deproteinized mineral bovine bone graft, in which the thickness of mucosa and the height of bone crest remained statistically stable. Positioning during implant installation is not only a question of directing occlusal forces on its long axis, but mainly a matter of aesthetic expectation concerning the future prosthetic crown. The vertical distance between the implant platform and the cervical margin of the crown of neighboring teeth should never surpass 3 mm or be shorter than 2 mm. In the labiolingual direction, the implant must not be distant from the labial limit of the bone wall, which would result in the construction of a prosthetic crown with enlarged labial volume, detrimental to hygiene and aesthetics. As for the mesiodistal direction, the implant must be well-centered to avoid proximity to adjacent roots and favor the formation of interproximal papillae. Therefore, a space of 2 mm between the implant and the neighboring roots is necessary, and it must be of 3 mm minimum in the case of distance between two implants, since an inadequate space will cause loss in the bone crest and, consequently, a predictable reduction in the height of interdental papillae (Tarnow et al.)6. Aiming at valuing and guiding the positioning of implants during surgical installation, some authors report the importance of using radiographic and surgical guides. This procedure generates a three-dimensional map of implant position that help reaching a higher number of implants placed in optimal positions (Higginbottom and Wilson)7. The second-stage surgery of implants installed in the anterior region must be seen as an additional opportunity of aesthetic resource, when we can manipulate soft tissues with a more favorable healing in mind. This concern was reported by Reikie8, when this author proposed a simplified surgical technique to establish a better relation of the soft tissue around an implant at the moment of performing the second-stage implant surgery and installing the healing abutment, in which the surgical flap provides an overcontour of mucosa on the healing. The construction of a good crown on the implant should always be preceded by the making of an adequate provisional restoration that guides the adjacent mucosa to achieve an ideal contour and the formation of papillae. The establishment of the interproximal contact point is directly related to the presence or absence of interproximal papillae. In an assessment of 288 sites, Tarnow et al.9 showed that, when the distance from the bone crest to the proximal contact point was 5 mm or less, papillae reformed in about 100% of cases; as this distance increases, the percentage of papilla formation decreases considerably. . Other studies have shown the osseous-gingival relationship as a means to achieve predictable aesthetic results concerning the formation of interproximal pappilae between adjacent implants and between implants and natural teeth, Salama et al.10 and Tarnow et al.11. To achieve an emergence profile by means of a provisional crown, it is necessary that adjustments in the contour, increasing or decreasing its volume, press the mucosa to cause a slight transient ischemia that stops at 5 to 10 minutes (Macintosh and Sutherland)12. Such adjustments must be gradual until we achieve the ideal contour, with reestablished interproximal pappillae and a definitive emergence profile. The development of reinforced ceramics has provided a new alternative for the achievement of satisfactory results when we work with implant-supported restorations in aesthetically demanding areas. Metal showing through periimplant mucosa produces an undesirable grayish hue, mainly when the soft tissue is thin. Choosing an all-ceramic intermediate abutment is today the best option for single crowns in the maxillary anterior region. It is true that, even being aesthetically more appropriate, all-ceramic abutments are more sensitive to manipulation when compared to titanium abutments (Andersson et al.)13, which can induce to a decrease in mechanical resistance. This statement concerning technical sensitivity was later observed by Tan and Dunne14 as well, although, in a clinical case report about restorative alternatives, they showed the aesthetic superiority of all-ceramic abutments and crowns. However, in a clinical study, including analysis and a 4-year followup, Glauser et al.15 observed 54 implant-supported restorations, made of zirconia abutments under all-ceramic crowns (Empress I), and concluded that those abutments offered enough stability to support a single implantsupported restoration for anterior region and premolars. These authors also concluded that soft and hard tissues reacted favorably. Confirming these data, an experiment simulating the exposure of 48 crowns to continual occlusal loads and thermal variations demonstrated that even metal abutments having significantly higher values, alumina and zirconia abutments are able to resist physiologically to occlusal forces in the anterior region (Att at al.)16. Exactly as the ceramic intermediate abutments, fully metalfree crowns represent the best choice for a better aesthetic result in rehabilitation on implants. The margin of the subgingival emergence of an implant-supported crown must be respected so that the deepening is not excessive, which could make difficult the removal of excess cement inside the peri-implant groove. Sutherland et al.17 have already reported their concern with the quality of this margin when measuring the marginal gap of all-ceramic crowns cemented on CeraOne abutments with three different materials, in an experiment that concluded that large marginal discrepancies could cause problems in the peri-implant region. Unhealthy peri-implant tissues may represent a significant aesthetic problem, since they could potentially alter the stability of soft and hard tissues. In a laboratory investigation, Kohal et al.18 concluded that an all-ceramic crown seems to fulfill all biomechanical requirements for the anterior area; however, further studies still have to be conducted. The laboratory stage is also highly important to guarantee a favorable aesthetic solution for metal-free crowns, given that a thin ceramic layer applied on its infra-structure could interfere in the final color (Nakamura et al.)19. Based in this case report and the literature review, it can be concluded that: the development and commercialization of new reinforced ceramics allow the oral surgeon to work with a higher level of predictability concerning aesthetic solutions in anterior restorations on single implants.Achieving aesthetic results when one intends to rehabilitate an anterior area by means of implant-supported crowns requires a rigorous protocol, in which the oral surgeon must know the criteria to be adopted for a correct prosthetic intervention, and the prosthetist, on their turn, must know all surgical steps, so that both can carry out the best planning for each case. References
© Copyright 2007 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os07021f15.jpg] [os07021f7.jpg] [os07021f13.jpg] [os07021f10.jpg] [os07021f8.jpg] [os07021f4.jpg] [os07021f16.jpg] [os07021f5.jpg] [os07021f20.jpg] [os07021f12.jpg] [os07021f6.jpg] [os07021f2.jpg] [os07021f17.jpg] [os07021f11.jpg] [os07021f9.jpg] [os07021f3.jpg] [os07021f18.jpg] [os07021f14.jpg] [os07021f1.jpg] [os07021f19.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}