 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
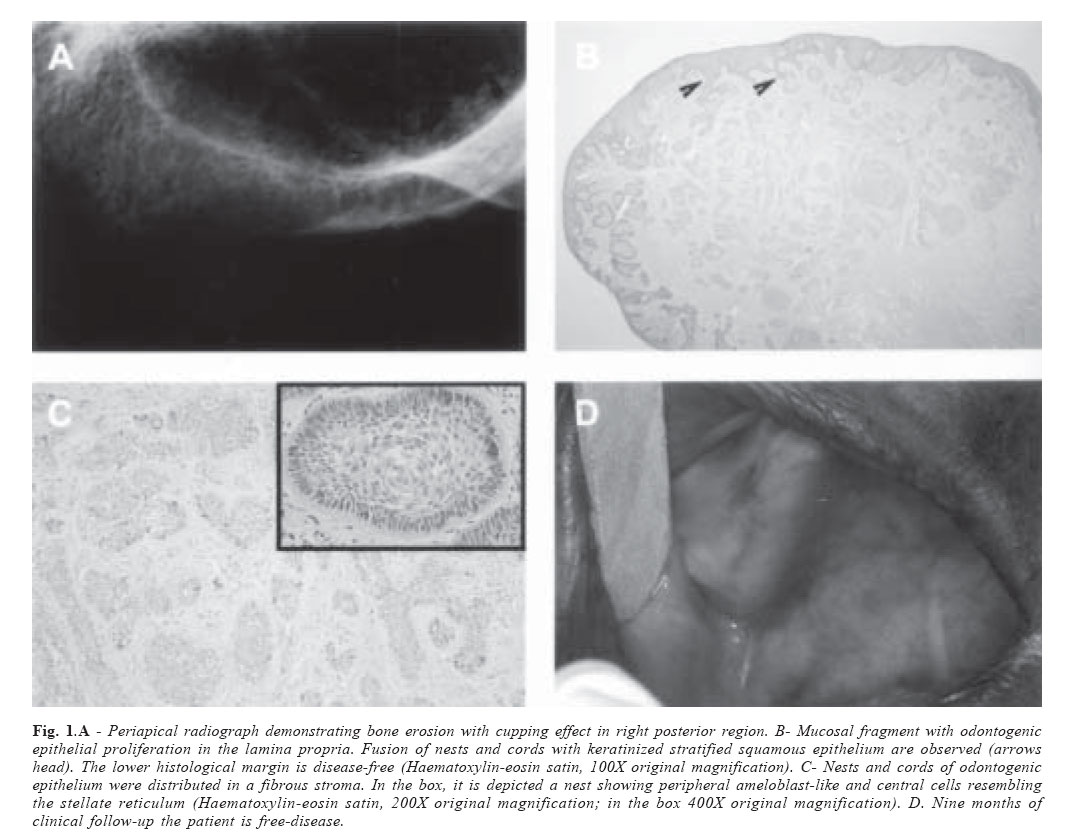
Brazilian Journal of Oral Sciences, Vol. 6, No. 21, April - June 2007, pp. 1364 - 1366 A clinical case of peripheral ameloblastoma Carolina Cavaliéri Gomes1*, Bruna Gonçalves Garcia1*, Ricardo Santiago Gomez2*, João Batista de Freitas3*, Ricardo Alves Mesquita2* 1DDS. Undergraduate student Correspondence to: Ricardo Alves Mesquita Universidade Federal de Minas Gerais -Faculdade de Odontologia Av. Antônio Carlos, 6627, Pampulha Belo Horizonte, Minas Gerais, Brazil CEP: 31270-901 Fax: +55 31 3499-2472 E-mail: ramesquita@ufmg.br Received for publication: March 28, 2007 Code Number: os07022 Abstract The peripheral ameloblastoma (PA) is a rare, benign, extraosseous odontogenic soft tissue tumour that is confined to the gingiva or alveolar mucosa. The PA presents the same histological characteristics of intraosseous ameloblastoma, although it is less aggressive than this classical subtype. We report a clinical case of PA of the alveolar mucosa in the right posterior maxilla, highlighting the importance of histological examination to the diagnosis. Key Words: peripheral ameloblastoma, odontogenic tumour, gingival lesions Introduction The peripheral ameloblastoma (PA) is a rare, benign, extraosseous odontogenic soft tissue tumour that was first truly reported in the literature by Stanley and Krogh in 19591. The clinical appearance of the PA may vary, but most of time it presents clinically as a slow-growing, firm, painless mass with a sessile or pedunculated base with a smooth surface and a normal mucosa color. Although it is usually confined to the gingiva or alveolar mucosa it may cause a depression of the underlying bone or exhibit a “cupping” effect due to the pressure resorption2-6. We presented an additional clinical case of PA that occurred in the right posterior alveolar mucosa of the maxilla. Clinical CaseA 79-year-old woman presented to the Stomatology Clinic of the School of Dentistry, Federal University of Minas Gerais (Belo Horizonte, Brazil) reporting a painless swelling on the gingiva. The patient could not tell when she noted the lesion. She was edentulous and did not wear dental prosthesis. Intraoral exam revealed a nodule covered by normal mucosa with a smooth surface and firm consistency located in the right posterior alveolar mucosa of the maxilla measuring approximately 6x4x4mm. Periapical radiograph examination displayed bone erosion with cupping effect (Figure 1A). With the hypothesis of soft tissue tumours or peripheral odontogenic tumors, an excisional biopsy was performed. The specimen was fixed in 10% formalin buffer and was sent to the Oral Pathology Service. The microscopical findings were nests and cords of odontogenic epithelial cells showing ameloblast-like peripheral cells with polarized nuclei and central cells reticulum estrellate features. These nests and cords were distributed in a fibrous stroma and they seemed to fuse with the keratinized stratified squamous epithelium that covered the lesion. The histological surgical margin of the excised lesion was disease-free (Figures 1B and C). The diagnosis was peripheral ameloblastoma. The patient is in follow-up for nine months without signs of recurrence (Figure 1D). Discussion Ameloblastoma is an epithelial odontogenic tumour of the jaw bones which is thought to arise from rests of the dental lamina or from basal cells of the surface epithelium7-9. A recent investigation demonstrated that alterations of the ameloblastin gene forms the genetic basis for ameloblastoma10. Currently, ameloblastoma was divided in four clinicopathological types: solid, desmoplastic, unicistic and peripheral7. The PA is also known as the extraosseous ameloblastoma, soft tissue ameloblastoma, ameloblastoma of mucosal origin, or ameloblastoma of the gingiva. It comprises 1.3-10% of all ameloblastomas3. While some lesions are localized entirely within the connective tissue of the gingiva, others seem to fuse with or originate from the mucosal epithelium, the former present in the current case report7. Phillipsen et al.3 in 2001 reviewed 160 cases of PA and observed that this tumor usually exhibit as a painless, sessile, firm growth with a smooth surface. In the majority of the cases there is no radiological evidence of the bone involvement3. The PA is more common in men (65%) and the mean age at the time of diagnosis is 52.1 years old. Although our case occurred in the posterior maxilla of a woman, the mandible is the most common site for PA accounting for 70.9% of the cases3. The differential diagnosis should include soft tissue tumors such as peripheral giant cell granuloma, peripheral odontogenic fibroma, peripheral ossifying fibroma, papilloma and pyogenic granuloma3-4. Authors believe that PA totally lacks the persistent growth of intraosseous ameloblastoma. It is less aggressive than the intraosseous ameloblastoma and the term PA can be potentially dangerous because the diagnosis may lead to unnecessary aggressive treatment11. Although the recurrence rate of the PA is much lower (16%, 19%)12-13 than the intraosseous ameloblastoma, long-term follow up is required. In addition, recurrent lesion has been reported as an ameloblastic carcinoma14. Our case has nine months of followup and the patient is free of disease. Although the current case had clinical appearance of reactive hyperplastic lesions, the microscopic examination revealed the diagnosis of PA. Therefore, it is important to include peripheral ameloblastoma as a differential diagnosis of nodular lesions of gingiva and alveolar mucosa. Acknowledgements The authors would like to thank FAPEMIG (CDS 895/05) and CNPq (301736/2004-9; 502978/2004-0) for financial support. RS Gomez and RA Mesquita are research fellows of CNPq. References
© Copyright 2007 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os07022f1.jpg] |
| |||||||||

{kind=link}