 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 6, No. 23, October-December, 2007, pp. 1432-1437 Effect of platelet-rich plasma on gingival and periodontal ligament fibroblasts: new in-vitro growth assay Fatih Arikan1 Sema Becerik1 Sule Sonmez1 Ismet Gurhan2
1Ege University, School of Dentistry, Department of Periodontology 2Ege University Faculty of Engineering, Department of Bio-Engineering
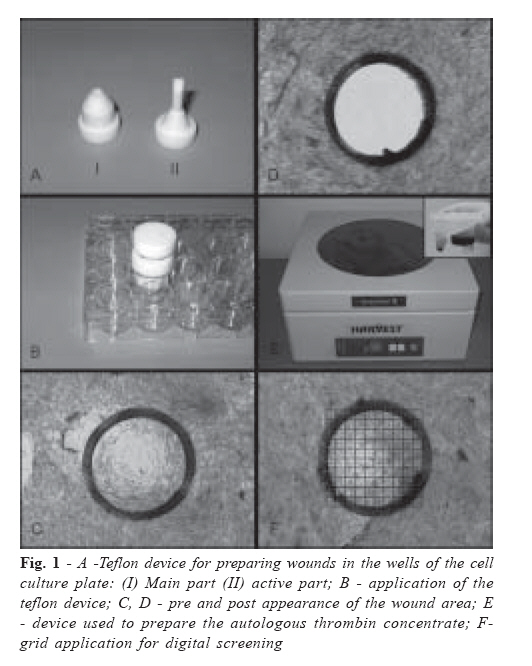
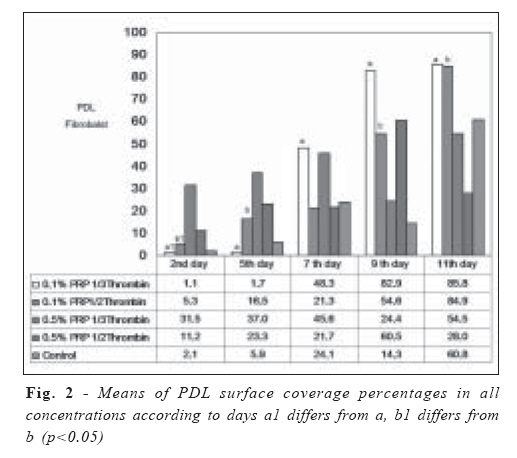
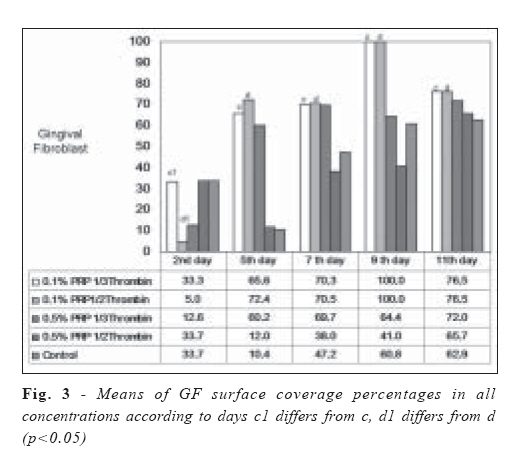
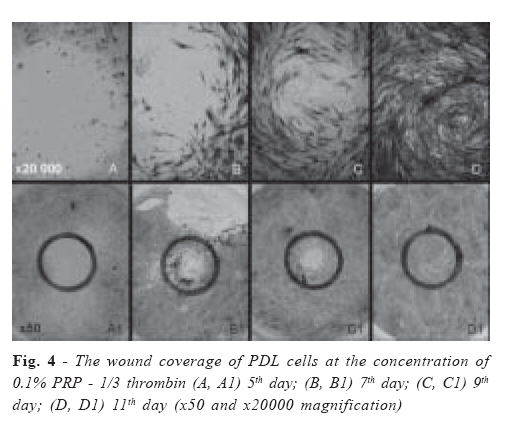
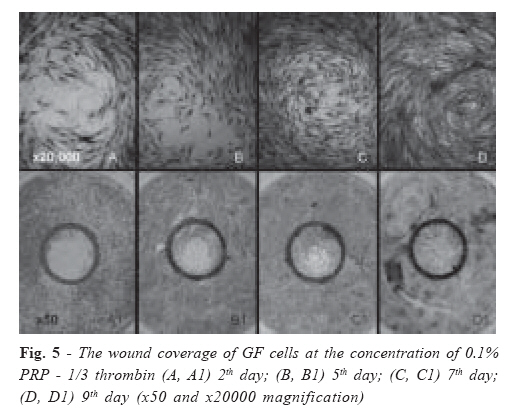
Received for publication: September 9, 2007 Accepted: November 29, 2007 Code Number: os07035 Abstract The use of platelet-rich plasma (PRP) as a source of growth factors is reported to be beneficial for periodontal regeneration. The aim of this study was to evaluate its effect on gingival and periodontal ligament fibroblast healing on a special growth assay designed by the working group. A wound with a 5 mm of diameter has been performed on periodontal ligament (PDL) and gingival fibroblast (GF) cell cultures. The cell wells were divided into five groups. The control group received only Dulbecco’s modified Eagle’s medium/ Ham’s (DMEM) and the test groups received 0.5% PRP with 1/3 or 1/2 thrombin; 0.1% PRP with 1/3 or 1/2 thrombin. All of the groups were stained with haemotoxylene-eosine on days 2, 5, 7, 9 and 11. Digital screenings were performed on each time stop and the results were interpreted by means of % surface area covered by the cells. The results showed that 0.1% PRP with 1/3 thrombin group have closed up the wound circle in GF group at day 9 and in PDL group at days 9 and 11 with a significant difference when compared with other groups. GF response was significantly better than PDL cell response starting from day 5. Concluding, PRP favored wound closure in PDL and GF cell cultures and the developed growth assay may be utilized in future investigations of the biological basis of periodontal wound healing. Key words: periodontal regeneration; wound healing model; PRP Introduction Periodontitis is a chronic inflammatory disease leading to the destruction of tooth-supporting structures. A therapeutic method producing predictable regeneration of the periodontium remains to be the major goal of periodontal therapy. Current methods for enhancing periodontal regeneration are: application of root conditioning agents1 , application of tissue guiding membranes2, and implantation of inert osteoconductive/osteoinductive materials3 . Recently, autologous PRP has gained popularity as a clinical treatment in periodontal regeneration4-6 . The wound healing process is a complex mechanism characterized by four distinct, but overlapping, phases: hemostasis, inflammation, proliferation and remodeling7 . The proliferative phase includes blood vessel formation by endothelial cells and bone synthesis by osteoblasts. All these events are coordinated by cell-cell interactions and by soluble growth factors released by various cell types5 . Medical literature provides evidence that platelets contain many growth factors including platelet derived growth factor (PDGF), insulin-like growth factor (IGF) and transforming growth factor- â (TGF-β ) that enhance wound healing and help to induce regeneration of the tissues8 . This autologous plasma is a rich source of growth factors and its application has been reported as an effective way to induce tissue repair and regeneration9 . Although its therapeutic effectiveness is still under investigation by many research groups, data have been reported recently by several investigators. High levels of both PDGF and TGF- β are contained in human PRP preparations and that modulates proliferation of cultured human periodontal ligament (PDL) fibroblasts or oral epithelial cells in a cell type-specific manner10 . Kawase et al.4 stated that PRP provides platelet aggregates as nuclei to initiate mineralization with stimulating PDL cell proliferation, differentiation and collagen production. The combination of these effects may effectively mediate PRPs ability to promote regeneration of periodontal tissue, including skeletal tissue at the site of injury. For economical and biological reasons, PRP preparations has been fractionated from plasma of patients and used as an autologous source of these growth factors to regenerate periodontal tissue defects. This is based on the evidence that human platelets are enriched with PDGF and TGF-β 4,10 . However, limited information is currently available concerning the quantitative effect of PRP on PDL and gingival fibroblast (GF) regeneration. A new in vitro growth assay has been developed in the present study and it has been aimed to quantify the effect of PRP on PDL and GF wound healing in vitro. Materials and Methods Cell Culture Human PDL fibroblasts were obtained from healthy premolar teeth extracted for orthodontic reasons from systemically and periodontally healthy three patients (age between 12-16 years) according to the method of Somerman et al.11 with slight modification. The patients were duly informed of the nature and extent of the study, and informed consents were obtained according to the Helsinki Declaration. Following the extraction, the teeth were immediately placed in Dulbecco’s modified Eagle’s medium/Ham’s F-12 (DMEM/ F-12) (Biochrom, Germany) with 0.1% NaHCO3 , 400 U/ml penicillin / 400 μg/ml streptomycin and 0.5% amphotericin B. Under sterile conditions, the PDL tissue was collected from the mid-third portion of the teeth roots with a scalpel and transferred into 35-mm diameter culture dishes and then cultured with DMEM/F-12 supplemented with 20% ml fetal bovine serum (FBS) (Biochrom, Germany) 0.1% NaHCO3 , 400 U/ml penicillin / 400 μg/ml streptomycin and 0.5% amphotericin B at 37°C in the presence of 5% CO2 in air. Human GFs were obtained from the papillae of the same healthy premolar teeth extracted for orthodontic reasons from the systemically and periodontally healthy patients. Following the extraction of the tooth the papillae was excised with a scalpel and immediately placed in DMEM/F-12 with 0.1% NaHCO3, 400 U/ml penicillin / 400 μg/ml streptomycin and 0.5% amphotericin B. Under sterile conditions, the gingival tissues were transferred into 35 mm culture dishes, cut into small portions with a scalpel and cultured with DMEM/F-12 supplemented with 20% FBS (Biochrom, Germany), 1% NaHCO3, 400 U/ml penicillin /400 μg/ml streptomycin and 0.5% amphotericin B at 37°C in the presence of 5% CO2 in air. Within 30 days, all the PDL and GF outgrowth became confluent. These confluent cells detached by trypsin/ EDTA treatment and transferred to 25 cm2 culture flasks. The sixth passages were used in this study. In Vitro Growth Assay Protocol For preparing standard wound, 2 ml of medium containing 105 PDL cells/ml or 105 gingival cells/ml was put into 10 wells of standard 24 well culture plates. After 24 hours incubation in DMEM/F-12 supplemented with 10% FBS, 0.1% NaHCO3 , 400 U/ml penicillin / 400 μg/ml streptomycin and 0.5% amphotericin B at 37°C in the presence of 5% CO2 in air, confluent monolayer of PDL and gingival fibroblasts were obtained. Standard wounds were created in the cultured cells by using a teflon device which has been developed by the working group of the present study. To prepare the wound, first, the main part (Figure 1-A-I) of the device was placed into one of the wells of the 24 well plate, then the active part (Figure 1-A-II) of the device was placed through the main part and turned clockwise several times (Figure 1-B), dragging the surface of the culture plate in order to disrupt and remove the cellular and extra-cellular material. The wounded well then was washed 3 times with PBS to remove the peeled cells (Figure 1-C, D). The wounds which had a diameter of 5 mm and located centrally in the 10 wells of 24 well culture plates were checked under inverted light microscope (Olympus CK, Japan). Preparation of PRP PRP was prepared following a simple protocol. Venous blood samples were withdrawn from one healthy volunteer. Autologous platelet concentrate was prepared with SmartPReP®2 (APC-20i) (Harvest Technologies Corporation, MA, USA) with the related device (Figure 1-E) and thrombin supply was prepared with autologous thrombin kit (Hat Kit) (Harvest Technologies Corporation, MA, USA). The mentioned procedures were done as described in the manufacturer’s instructions. The harvested PRP was added to complete medium at a ratio of 0.5% & 0.1% and incubated at 37oC for 30 minutes. The presence of FBS allowed platelet aggregation and degranulation. Human thrombin obtained by autologous thrombin kit (Hat Kit) (Harvest Technologies Corporation, MA, USA) was added to medium for platelet activation at 50% (1/2) and 33% (1/3) ratio of PRP and the prepared solutions were applied on PDL and GF cells. As a result of incubation, a gel was formed which is rich of plateletderived growth factor and this gel survived for 11 days by adding the medium two times a day to the wells. The cell wells were divided into five groups. The control group received only DMEM, where the test groups received 0.5% PRP with 1/ 3 thrombin; 0.1% PRP with 1/3 thrombin; 0.5% PRP with 1/2 thrombin and 0.1% PRP with 1/2 thrombin respectively. All of the groups were stained with haemotoxylene-eosine on days 2, 5, 7, 9 and 11. All examinations were done twice for GF and PDL cells on each group for each day (2, 5, 7, 9 and 11) and the whole assay was repeated for 3 times. Evaluation of the Repopulation of the cells Digital screenings were performed on each time stop and a grid with 304 equal squares has been placed on each wound circle (Figure 1-F). The squares occupied by the cells have been scored from 1 to 4, meaning that if the recorded score is 1.25% of the square is covered by the cells. When the wound area is covered completely, the score was marked as 1216. All the sample pictures were represented with a code and blind evaluations were performed by three independent observers of the working group. The results were interpreted by means of % surface area covered by cells. Statistical Analysis Data were analyzed by descriptive statistics (means and standard deviation). Pearson’s correlation analysis was applied to evaluate the harmony between the three observers and the statistical analysis was based on the number of repetitions. The counted cell numbers were analyzed after log 10 transformation. A double factored repeated measure of ANOVA was performed to evaluate the effect of various concentrations to cell numbers on different time stops. A significant interaction was found between concentration and time stops; therefore the statistical analysis preceded with the evaluation of every concentration at all the time stops with single factored repeated measures of ANOVA. Dunnet-C test was used to compare the concentrations where a significant difference was found on specific time stops. Difference was considered significant at a p-value < 0.05. Results Pearson’s correlation analysis was performed on the results of every time stop and it was assessed that the observers are in harmony in counting the cells. A comparison between the days and the PRP concentrations used was performed with repeated measures of ANOVA on the mean of the values declared by the three observers. Mean percentages of wound coverage for PDL and GF in all concentrations according to days are presented in Figure 2 and 3. PDL cells group: There was a significant difference on the coverage of the wound between the 2nd day and the 5th, 7th, 9th, 11th days of the PDL /0.1% PRP - 1/3 thrombin group respectively especially better results on day 9-11 as shown in Figure 2. According to Dunnet-C test results, there was a significant difference between the PRP concentrations of PDL cells on 2nd day (p<0.05), meaning that 0.5% PRP concentrations are more effective on cells in coverage when compared to 0.1% PRP Figure 2. Figure 4 shows the wound coverage of PDL cells on days 5, 7, 9 and 11 at the concentration of 0.1% PRP - 1/3 thrombin, where 2nd day image is not included because there were very few cells. GF group: Figure 3 and 5 shows the wound coverage of GF cells on days 2, 5, 7 and 9 at the concentration of 0.1% PRP -1/3 thrombin, where 11th day image is not included because the wound area was fully covered by the cells at 9th day (p<0.05) (Figures 3, 4 and 5). A significant difference was also found between the 2nd day and 7th, 9th, 11th days of the GF 0.1% PRP -1/2 thrombin and 0.1% PRP-1/3 thrombin group respectively (p<0.05) Figure 3. There was a significant difference between the PRP concentrations of GF cells when the results are analyzed with Dunnet-C test. On the wound coverage, this finding has been switched on the 5th day; such as, the 0.1% PRP concentration has a more positive effect on the cells when compared to 0.5% PRP (p<0.05). However, when focused on the time intervals 5, 7, 9, 11 0.1% PRP - 1/3 thrombin and 0.1% PRP - 1/2 thrombin concentrations were found to be effective for GF in wound coverage. The interaction between the days and the concentrations was significant (p<0.05); therefore, the inter group variation of every concentration according to days was analyzed. The difference between the percentage of wound coverage at the same time stops between the concentrations 0.5% PRP 1/3 thrombin and 0.5% PRP - 1/2 thrombin was not statistically significant both in PDL and GF. Also the control group did not reveal statistically significant difference at the percentage of wound coverage between the time intervals. GF cells seem to respond better when compared to PDL cells at the mentioned time intervals. It has been found out that 0.1% PRP with 1/3 thrombin group have closed up the wound circle with a significant difference when the GF and PLF group combined in this concentration (p<0.01). Day 9 GF group and in PDL group has significant difference when compared with other groups. GF response is significantly better than PDL cell response starting from day 5 to 11 (p<0.01). Discussion Periodontal wound healing is regulated through multiple cellular and molecular interactions. On a cellular level, there have been only a few studies that have compared proliferation rates between PDL and GF. Lacker et al.12 have documented the development of an in vitro model capable of investigating cellular events associated with wound healing. Using both human PDL cells and GF confluent cultures, they created in vitro wounds mechanically by removing a 3 mm wide band of the cell layer. Furthermore, they have shown that the response to wounding is inherently different in PDL and GF cultures, suggesting unique signaling mechanisms. The results suggested that GF possess the ability to fill the wound areas at a faster rate than PDL cells, consistent with current principles of GTR. The working group of the present study has improved the wound model of Lacker et al.12 and developed a circular wound area that can be fully controlled in quantitative surface coverage analysis. Presently, it has been shown that following in vitro wound development, when considering wound fill as a measure of overall effects of both migration and proliferation, GF repopulated the wound at a greater rate than PDL which is in parallel with the previous studies12-14. The proposed mechanism of PRP’S action on PDL and GF cells is that fibrinogen contained in PRP is cleaved by a serine protease thrombin which is produced by these cells and converted to insoluble fibrin. The formation of fibrin clot is positively promoted probably by a component(s) derived from platelets. The resulting fibrin clot stimulates type I collagen synthesis more potently than PDGF, TGF-β , or fibrinogen each alone and the growth factors contained in PRP (and probably fibrinogen/fibrin combination) stimulate the cell proliferation. Thus, it is suggested that PRP is capable of increasing cell numbers and simultaneously up regulating extra-cellular matrix production. These 2 actions in combination would effectively promote wound healing at the site of periodontal injury4,10,15. In an in vitro study, Kawase et al.4 suggested that fibrinogen, converted to fibrin, in combination with growth factors present in PRP effectively promote wound healing at sites of injury in periodontal tissues. Okuda et al.10 demonstrated that both PDGF-AB and TGF-β 1 are highly concentrated in the PRP preparations. They suggested that cell type-specific actions may be beneficial for periodontal regenerative therapy. Annunziata et al.15 investigated the effects between PRP and cell populations involved in periodontal regeneration, namely primary human PDL cells, GFs and keratinocytes. As a result, they found out that there was a strong stimulation of human periodontal ligament cells proliferation, a minor increase in the growth rate of human gingival fibroblasts and a marked decrease of human keratinocyte proliferation was evident. The results of the present study are in parallel with the aforementioned investigations. When compared with the control group, the PRP applied groups presented a better wound coverage at all concentration (p<0.05). Furthermore, the developed wound model let the investigators of the present study to evaluate the quantitative effect of four different PRP concentrations on the wound coverage. Platelet concentrates are potentially useful in wound-healing applications because they function as both tissue sealant and a drug delivery system that contains a host of powerful mutagenic and chemotactic growth factors5,16-18. However, the method of PRP preparation has a potentially significant impact on the different levels of platelet recovery and activation. Platelet activation during preparation of the platelet concentrate can result in early á-granule release and loss of the growth factors during the collection process5,19. It is therefore critical to recognize that each PRP preparation method may differ in regard to the platelet number, platelet activation rates and growth factor profiles. Weibrich et al.20, who analyzed the effect of platelet count in PRP on bone regeneration in vivo stated that the PRP concentration they used was less than 10%, and Frèchette et al.5 used a PRP concentration of 10% while investigated the growth factor content of PRP and its roles in wound healing. In the present study, a preliminary test was performed to determine the accurate PRP concentration. It was found out that at concentrations of 10% and 5%, the PDL cells and GFs could not survive. It can be due to the platelets in PRP shared the nutritional sources of the culture media with the PDL cells and GFs. According to the preliminary test, the highest PRP concentrations were 0.1% and 0.5%. The thrombin supply concentration suggested by the manufacturer of SmartPReP® (Harvest Technologies Corporation, MA, USA) was 33% (1/ 3). Just for a test, a concentration of 50% (1/2) was also used but it was found out that 1/3 thrombin acted better than 1/2. Also, 0.1% PRP presented a better wound coverage than 0.5% PRP. The reported in vitro effects of PRP on periodontally related cells are similar to those described for some platelet-released growth factors. In particular, platelet-derived growth factor and transforming growth factor-â act as strong mitogenic and anabolic factors and are reported to markedly stimulate the proliferation of fibroblasts and PDL cells, as well as extracellular matrix formation20. PRP contains high levels of these growth factors, together with other active molecules such as fibrin and fibrino-peptides during clot formation10,14,17. Thus, PRP could affect behavior of periodontally related cells by a platelet-derived growth factor- and/or transforming growth factor-â mediated action10,17. Differing from the results of the present study, recent clinical trials21-24 focusing on the usage of PRP combined with different types of bone substitutes in intra-bony defects revealed that the applications had no benefit in reduction of pocket depth, clinical attachment gain and defect fill. A possible explanation could be that PRP is delivered into the cultures several times, while clinically a single application could be performed. Another reason is that different concentrations of thrombin are added to platelets in the present study, where the clinical studies mentioned above added bioactive glass21, natural bone mineral22, β-TCP23, and inorganic bovine bone mineral24 to PRP instead. Platelets are activated in the presence of thrombin and release a myriad of proteins and growth factors, helping in the development of the fibrin clot which is the first step of the healing process25,26. The authors of the present study believe that organizing an in vitro study with osteoblasts and adding PRP with thrombin to the culture media will clarify this conflict. In conclusion, the cell-type growth modulation represents important biological effects of PRP on periodontally related cells and PRP plus thrombin concentrations may have varying affects on different cell type in the periodontal tissue regeneration. Acknowledgement The research has been supported by the Ege University Research Foundation and presented orally in Europerio 5, Madrid, Spain, 2006. References
© Copyright 2007 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os07035f4.jpg] [os07035f3.jpg] [os07035f2.jpg] [os07035f1.jpg] [os07035f5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}