 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 6, No. 23, October-December, 2007, pp. 1450-1456 A clinical evaluation of bioactive glass particulate in the treatment of mandibular class II furcation defects Manoj Humagain1 Dilip G Nayak2 Ashita S Uppoor3
1Specialist Resident , 2Professor and Head ,3 Professor
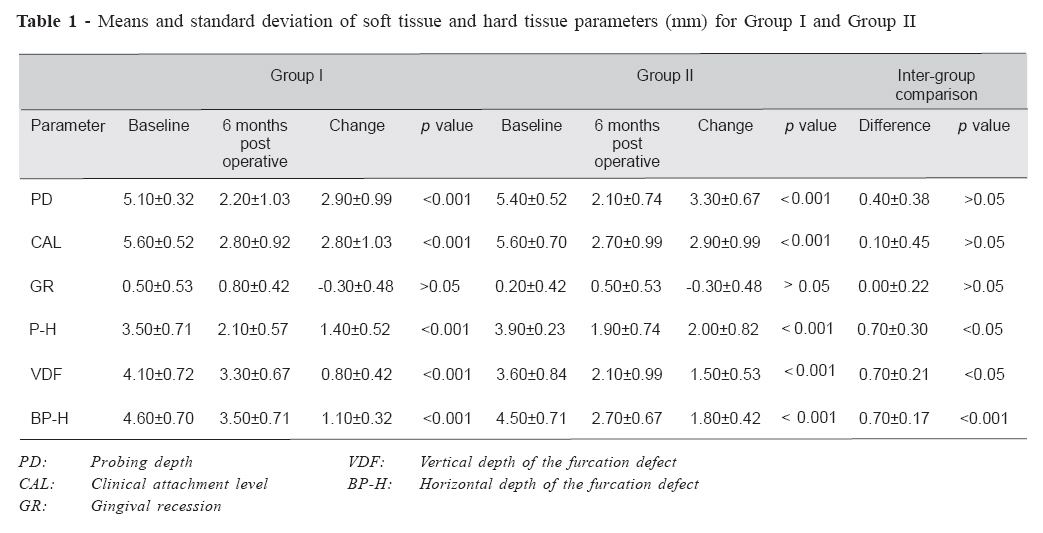
Received for publication: July 27, 2007 Accepted: November 08, 2007 Code Number: os07039 Abstract Bioactive glass particulate has been applied to dentistry in the treatment of bone defects, ridge preservation and periodontal bone defects including the furcation defects. The aim of this study was to compare the clinical attachment gain and vertical and horizontal bone fill obtained with open flap debridement (OFD) alone and OFD with bioactive glass particulate in the treatment of mandibular Class II furcation defects. Twenty mandibular class II furcation defects were selected in 16 systemically healthy patients out of which 10 defects were treated with OFD alone (Group I) and other 10 defects were treated with OFD and bioactive glass particulate (Group II). Each defect was randomly assigned to Group I and Group II. The soft tissue and hard tissue measurements including vertical probing depth, horizontal probing depth, clinical attachment level, gingival recession, vertical depth of the furcation defects, and horizontal depth of the furcation defects were recorded at baseline and six months post surgery. At 6 months evaluation, both treatment procedures resulted in significant improvement in soft tissue and hard tissue parameters when compared to the baseline. There was no significant difference between the two groups with respect to soft tissue changes (p>0.05) like probing depth reduction (3.30 mm versus 2.90 mm), clinical attachment level gain (2.90 mm Vs 2.80 mm) and gingival recession. Vertical defect fill were significantly greater in the bioactive glass sites (1.50 mm) compared to control sites (0.80 mm). There was highly significant reduction in horizontal probing depth of the defect (1.80 mm Vs 1.10 mm, p< 0.05) after 6 months post surgery. In conclusion, bioactive glass showed significant improvement in clinical parameters like vertical and horizontal defect fill in mandibular class II furcation defects when compared to OFD. Key words: furcation defects, bioactive glass, open flap debridement Introduction Management of molars with furcation involvement has been one of the most challenging problems in periodontal therapy. Teeth with furcation involvement undergo more extensive and rapid clinical attachment loss and are lost with greater frequency than are single-rooted teeth. One of the basic goals of periodontal therapy is the thorough removal of subgingival plaque and calculus as a prerequisite for reestablishment of a healthy periodontium, which can be maintained by patients on a long-term basis. In case of molars with furcation involvement, reduced efficacy of conventional periodontal therapy has been observed. Reasons for compromised results in furcation areas include the lack of proper access for instrumentation as well as for proper maintenance care due to the complex furcation anatomy, and consequently, a persistence of pathogenic microflora. The management of class II furcation involvement presents a unique clinical problem. Extensive research has been carried out over the past three decades in evaluating the efficacy of various treatment modalities employed for managing class II furcations1-5. The early work concentrated more on resective procedures intended to eliminate the pocket by furcationplasty and root resection1. The most favorable outcome of any furcation therapy would be the regeneration of the lost attachment apparatus, which would result in the closure of the furcation. A number of studies conducted in the past three decades have shown that class II furcation defects respond favorably to regenerative procedures in a predictable manner1-6. The various regenerative approaches utilized in the management of class II furcation involvements include root surface biomodification using root conditioning agents, coronally positioned flaps, the use of various bone replacement grafts, and guided tissue regeneration using non-resorbable or bioabsorbable barrier membranes2,6. Over the years, bone grafts have been widely used in the management of periodontal osseous defects and are still the most preferred regenerative technique. The various bone graft materials used in Periodontics include autogenous grafts, allogenous grafts, xenografts, and alloplasts. The use of autogenous grafts and decalcified freeze-dried allografts has shown significant clinical improvements, and histological studies have reported regeneration of the attachment apparatus. But the lack of adequate donor material and the fear of the remote chance of disease transmission have limited the use of autogenous grafts and allografts on a routine basis. This prompted the development of alloplasts or synthetic bone substitutes for periodontal applications. The bioactive glasses have been used extensively in medicine for middle ear surgery and have been applied to dentistry in the treatment of bone defects, ridge preservation and periodontal bone defects7. Recent reports in the literature have demonstrated that Bioactive Glass (PerioGlas®) may support regeneration in class II furcation defects by its osteostimulating mode of action, and there was a greater improvement in clinical indices for mandibular molar class II furcation treated with Bioactive Glass bone replacement graft than in those treated with open flap debridement surgery8-9. The aim of this study was to compare the clinical attachment gain and vertical and horizontal furcation bone fill obtained with Open flap debridement (OFD) alone and with bioactive glass particulate (PerioGlas® -Novo Bone Products, USA) in the treatment of mandibular molar class II furcation defects. Materials and Methods The present study was conducted in the Department of Periodontics, Manipal College of Dental Sciences, Mangalore, India. It was approved by Institutional Ethics Committee, Kasturba Medical College, Mangalore, India. Sixteen systemically healthy patients (10 males and 6 females, aged from 23 years to 62 years, with a mean age of 44 years) with 20 mandibular molar class II furcation defects (8 lingual and 12 buccal), according to the simplified classification of Hamp et al. (Carnevale et al.)10 in mandibular molars were selected for this study. Of the 16 patients enrolled, 4 patients demonstrated bilateral class II furcation defects. These patients served as split mouth candidates, receiving open flap debridement (OFD) alone in one defect (Group I) and OFD with PerioGlas in contralateral side (Group II).12 patients with unilateral class II furcation defects, served in either group I (6) or group II (6). The following criteria were adopted for patient selection:
Informed consent was procured from the patient in the form of a duly signed document prior to the surgical phase. Each patient was prepared for surgery with an initial phase of therapy including oral hygiene instructions, scaling and root planing, and occlusal adjustments was performed whenever necessary. Patients were re-evaluated to assess clinical parameters and monitored for plaque control four weeks after initial therapy. Clinical measurements Customized acrylic stents were fabricated on study casts and trimmed to the height of contour of the teeth, to serve as fixed reference point to take measurements [i.e. the lower border of the stent]. One vertical groove was prepared in the stent for the furcation that had to be measured. This groove is to provide reproducible alignment for a periodontal probe. All measurements in this study were performed with the help of a color coded UNC-15 periodontal probe and a 1 mm incrementally graduated Nabers’s probe. All measurements were rounded off to the nearest millimeter. All the clinical measurements were done by a single examiner to avoid interexaminer variation. Soft tissue measurement Soft tissue parameters were evaluated by ascertaining clinical attachment level, reduction in probing depth and gingival recession. The apical end of the vertical groove of the stent was used as a reference point (RP).
The following soft tissue measurements were taken along with the above-mentioned measurements after six months, i.e., clinical attachment gain, VPD reduction, and P-H reduction. Hard Tissue Measurements Hard tissue measurements were taken at baseline through bone sounding (probing bone level measurements) and via surgical entry (open bone level measurements). At six months post surgery, hard tissue measurements were taken through bone sounding only. Hard tissue changes were evaluated by using probing bone level measurements. At baseline probing bone level measurements and open bone level measurements were compared.
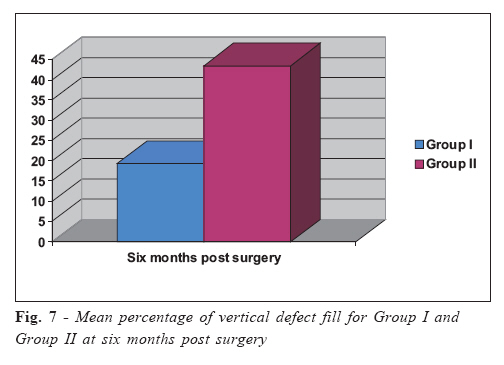
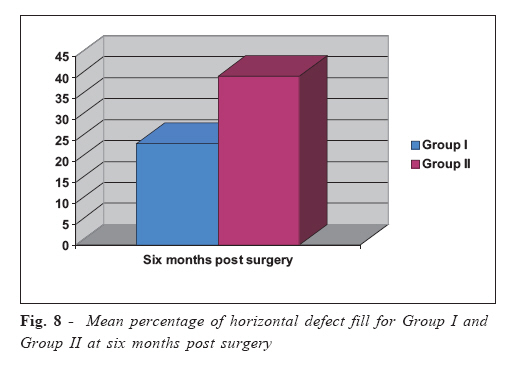
Both the vertical and horizontal open bone level measurements were taken during surgery before the placement of bioactive glass particulate into the defects. The following hard tissue parameters were taken after six months post surgery along with the above mentionedprobing bone measurements: vertical furcation bone fill in mm, horizontal furcation bone fill in mm, and percentage bone fill ( both vertical and horizontal). Surgical Protocol Following data collection, the decision to use PerioGlas bone replacement graft material or open flap debridement surgery only was determined randomly through coin toss. Under local anesthesia using Xylocaine 2 % with adrenaline 1:200000, and all aseptic precautions, continuous suction was applied to keep the surgical site clean. A sulcular incision was made and full thickness flaps was raised retaining sufficient tissue to attain primary closure (Fig 1). The furcation defects were thoroughly scaled and root planed with hand instruments and ultrasonic scalers. Following the removal of granulation tissue, enamel projections when noted was removed with high speed rotary instruments. Following surgical debridement, no root bio-modification or osseous resective procedures were attempted in this study. In patients selected for PerioGlas bone replacement grafts, the graft material was placed into the furcation defect with the help of a plastic instrument and was condensed in place to a level of the plane connecting the eminences of the root surfaces adjacent to the furcation defect (Fig 2). Care was taken so as not to overfill the defect beyond this reference plane. Primary soft tissue closure was done with interrupted sutures using non resorbable black silk sutures [4-0]. In patients selected for open flap debridement alone, flap was repositioned with interrupted sutures after the thorough cleaning and degranulation of the surgical site (Figure 3). Patients were prescribed 100 mg of doxycycline daily for ten days to prevent post surgical infection11, ibuprofen 800 mg every eight hours, as needed, for pain, and 0.2% chlorhexidine gluconate mouth rinse twice daily for four weeks post surgery to aid in plaque suppression. They were asked to refrain from mechanical plaque control for two weeks at the surgical site. Sutures were removed after seven days. Postoperative appointments were conducted at 7, 14, 21 days and one, three, and six months. At six month post surgery, both hard tissue and soft tissue measurement were taken. Statistical Analysis Both hard and soft tissue measurements were obtained at baseline and at the six months post surgery review appointment. Statistical analysis was employed to compare the study results. Microsoft Excel spreadsheet program was employed for tabulation and the statistical analysis was done with the Statistical Package for Social Sciences [SPSS-15] program. For each outcome measurement, 95% confidence interval (CI) was estimated for all observation times and for change from baseline to post surgery observation time. Unilateral and bilateral sites for the Alloplastic bone graft PerioGlas and open flap debridement groups, i.e. Group II and Group I respectively, were compared. Comparisons were made between Group I and Group II (inter-group) through unpaired Students “t” test and within the respective groups themselves through a paired Students “t” test (intra-group). Results All patients were compliant, and healing was uneventful for both groups. Baseline analysis did not display any significant differences between groups for any of the assessed variables, suggesting that final differences between treatment groups were not influenced by initial defect characteristics, thus allowing post treatment results to be compared. Changes in soft tissue and hard tissue parameters at six month post surgery for Group I and Group II, and the intergroup comparison are presented in Table 1. The mean percentage of vertical and horizontal defect fill was calculated for both groups (Figure 7 and 8). No site in either Group I or Group II displayed 100 % horizontal or Vertical defect resolution. Discussion A multitude of new materials has been used for promoting periodontal regeneration in furcation defects. Clinical application studies with bioactive glass particulate have been gaining momentum in recent years. Bioactive glass shows both osteoconductive and osteostimulatory effects. The pore size (90- 710) of bioactive glass allows an optimal space for vascularization. It is easy to manipulate and has a local haemostatic effect12-13. In the present study Group I showed statistically significant improvement from baseline to 6 months post surgery in soft tissue parameters such as probing depth reduction, gain in clinical attachment level (CAL) and horizontal probing depth reduction (Table 1). Similar results were observed by Andregg et al.14 and Ong et al.15 while using open flap debridement in the mandibular class II furcation defects. When soft tissue parameters were assessed from baseline to 6 months post surgery, Group II also showed significant mean probing depth reduction (3.30 mm), gain in CAL (2.90 mm) and horizontal probing depth reduction (2.00 mm) (Table 1). However, change in gingival recession (0.30 mm) was not CAL (0.87 mm), and increase in gingival recession (0.70 mm). significant. Mean recession observed in the past studies The hard tissue changes were evaluated using probing bone with the use of bone grafts in class II furcation defects ranges level measurements (bone sounding measurements). from 0.2 mm to 1.7 mm. Froum et al.8 and Zamet et al.16 Although surgical entry is the most accurate method to observed similar results using bioactive glass. The result of access hard tissue changes, trauma to the regenerated tissue, the present study was higher than the study by Ong et al.15 patient’s discomfort and ethical concern for the re-entry who found mean probing depth reduction (1.24 mm), gain in surgery were the limitations of the open bone measurements11-12. Bone sounding has been shown to be a reliable method in assessing hard tissue changes as surgical re-entry.17-18 Group I showed statistically significant improvement in hard tissue parameters from baseline to 6 months post surgery such as vertical and horizontal bone fill (Table 1). The mean vertical and horizontal bone fill in Group I was 0.80 mm and 1.10 mm respectively, which is in agreement with the findings of Froum et al.8. Renvert and Egelberg19 found defect fill of 0.9 mm 6 months post surgery which is similar to the findings of our study. Renvert et al.20 and Meffert et al.21 also found significant bone fill of 0.70 mm when treated with OFD alone. Similarly, Group II showed a significant improvement in hard tissue parameters after 6 months when compared to baseline (Table 6), which is in agreement with study inferences of Froum et al.8, Yukna et al.22, Park et al.12, Zamet et al.16. The mean vertical and horizontal bone fill in Group II were 1.50 mm and 1.80 mm respectively, which are highly significant. A literature review on treatment of periodontal defects by different surgical approach showed the mean defect fill in the sites treated with OFD and bone grafts was 1.2 to 3.6 mm23. The result of our study also falls within the same range. In intra-group comparison, there was no significant differences in the soft tissue parameters, except the mean reduction in horizontal probing depth (Table 1). Similar results were observed by Froum et al.8 and Ong et al.15. Hard tissue parameters demonstrated significant differences between groups, showing higher vertical and horizontal defect fill in Group II than Group I six months post surgery (Table 1). Kenney et al.24 showed significantly better defect fill in sites treated with OFD and bone grafts when compared with OFD alone. Similar results were achieved by Froum et al.8, Andregg et al.14, Zamet et al.16 with significant bone fill in the defects treated with bone grafts. The results of the present study are in general agreement with Garrett’s statement, i.e., “In controlled clinical trials treating furcation defects and intra-osseous defects with non- absorbable and absorbable synthetic bone graft materials have consistently demonstrated clinical advantages beyond that achieved by debridement alone”25. Moreover, the results are in line with the conclusion of Zamet et al.16 that bioactive glass treated sites showed a ‘greater trend to improvement’ when compared to OFD treated sites. In view of the present findings, it may be permissible to conclude that in this study, both an open flap debridement and open flap debridement with bioactive glass particulate (PerioGlas®) are effective in the treatment of mandibular class II furcation defects. The combination of open flap debridement with bioactive glass particulate leads to better results in hard tissue measurement as compared to open flap debridement alone. Future studies using bioactive glass particulate are needed to determine its efficacy in the treatment of furcation defects in large scale population. References
© Copyright 2007 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os07039f3.jpg] [os07039t1.jpg] [os07039f8.jpg] [os07039f7.jpg] [os07039f5.jpg] [os07039f4.jpg] [os07039f6.jpg] [os07039f2.jpg] [os07039f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}