 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 6, No. 23, October-December, 2007, pp. 1457-1461 Shear bond strength of metallic brackets bonded with four different composite resins Fábio Lourenço Romano1, Lourenço Correr-Sobrinho2* , Darcy Flávio Nouer3*, Américo Bortolazzo Correr4*, Mário Alexandre Coelho Sinhoreti2*, Maria Beatriz Borges de Araújo Magnani3*
1PhD Student in Orthodontics*, Assistant Professor, Dental School of Federal University of Alfenas, Orthodontics Area 2Professor, Department of Restorative Dentistry, Dental Materials Division 3Professor, Department of Pediatric Dentistry, Orthodontics Division 4PhD Student in Dental Materials *Piracicaba Dental School – State University of Campinas, Piracicaba, São Paulo Brazil
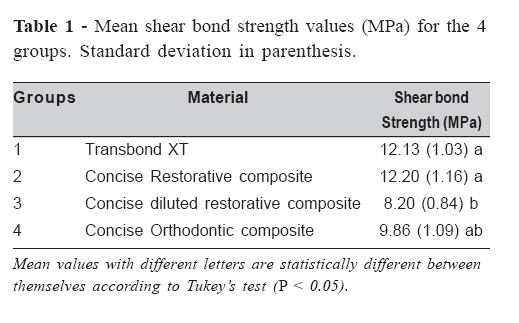
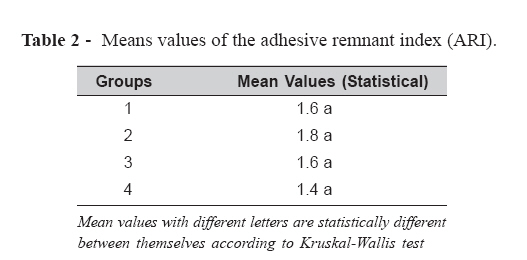
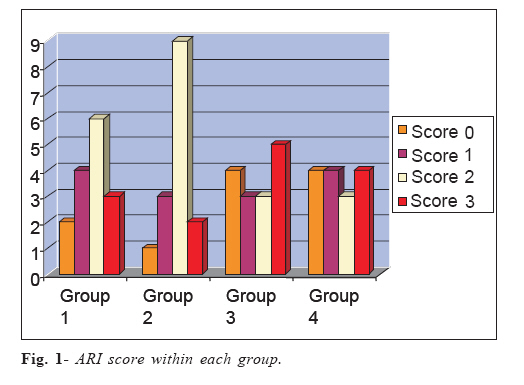
Received for publication: October 21, 2006 Accepted: October 26, 2007 Code Number: os07040 Abstract The objective of this study was to assess the shear bond strength of metallic brackets with different types of Concise composites and the Adhesive Remnant Index (ARI). Sixty bovine permanent lower incisors were inserted into PVC tubes and divided into four groups (n = 15): Group 1 – Transbond XT (control) composite; Group 2– Concise restorative composite; Group 3 – Concise diluted restorative composite (Artun and Zachrisson’s technique); and Group 4– Concise Orthodontic composite. After bonding the brackets, the samples were stored in distilled water at 37° C for 24 hours and then submitted to shear strength tests (Instron) at a crosshead speed of 0.5 mm/min. Analysis of variance and Tukey’s test (5%) were used for statistically analysing the data regarding the shear bond strength results, whereas Kruskal-Wallis test was used for analysing the ARI scores. The shear bond strength mean values (MPa) for Group 1 (12.13) and Group 2 (12.20) were found to be statistically higher (p < .05) than that for Group 3 (8.20). No statistically significant differences were observed (p > .05) between Groups 1, 2, and 4 (9.86) as well as between Groups 3 and 4. Regarding the ARI evaluation, the majority of the fractures involved the bracket/ composite interface. Key words: composite, orthodontic brackets, dental bonding Introduction The acid conditioning of dental surface proposed by Buonocore1 enabled increased adhesion between enamel surface and resin material due to mechanical imbrications caused by the resin and microporosities produced by acid etching. Orthodontics had taken advantage of this technique as orthodontic accessories can be directly bonded to enamel. Over the past few years one of the most commonly used materials for bonding orthodontic accessories to enamel has been the composite2-6, whose adhesiveness and clinical effectiveness have been corroborated by numberless studies in the literature7-11. Amongst these materials, we can cite the Concise composite (3M Dental Products, St. Paul, USA), which consists of two pastes – one working as an activator and the other as a catalyser, both chemically activated. Each paste has the same load concentration, the former containing tertiary amine and the latter containing benzoyl peroxide. The main component of the composite resin is the dimethacrylate, which results from the reaction between bisphenol-A and glycidyl methacrylate (BIS-GMA). The diluent resin is also dimethacrylate, with a solid fraction of 75%12. Although such a material was originally developed for restorative procedures, it has also been used in orthodontics for bracket bonding13. The Concise restorative composite usually employed for dental reconstruction is viscous and dry. Such characteristics are found to be ideal for bonding the brackets because the removal of excessive material around them is facilitated. On the other hand, the viscosity and dryness make the penetration of the material into the base of the bracket difficult, which impedes the complete filling of the bracket mesh structure and consequently decreases the mechanical retention between material and bracket (i.e. tooth)13. In order to improve the bonding of orthodontic accessories to tooth enamel, the Concise Orthodontic has developed a restorative composite with greater dilution and lesser viscosity13. This lesser viscosity makes the removal of material excess difficult and can dislocate the bracket already placed on the tooth enamel, thus interfering with its positioning. Despite the excessive dilution, the Concise restorative composite has presented good results for bracket bonding6-7,14-18 . In 1982, Artun and Zachrisson13 succeeded in obtaining adequate dilution of the Concise restorative composite for bracket bonding by increasing the fluid resin existing in each paste from 62% to 125%. According to the authors, such a dilution allows Concise restorative composite to become the ideal material for bonding orthodontic brackets to enamel without interfering with their positioning and also facilitating the removal of material excess. Another material specifically developed for bonding orthodontic accessories to enamel is the Transbond XT composite (3M Unitek, Monrovia, USA). This light-curing composite is composed of 14% BIS-GMA, 9% BIS-EMA, and 77% load particles. Transbond XT composite has been currently used in several controlled studies because of its adequate adhesive values for enamel6-7,16. Therefore, the objective of the present study is to assess the shear bond strength of brackets bonded with either Concise restorative composite, Concise Orthodontic composite or Concise diluted restorative composite by comparing them to Transbond XT. Material and Methods Sixty freshly, extracted bovine permanent lower incisors were collected, cleaned and stored in 10% formalin solution for 1 week in refrigerator at a temperature 6 °C. The selection criteria were intact buccal enamel with no cracks or decalcification. After being cleaned, the dental roots were centrally inserted into PVC tubes (Tigre, Joinville, Brazil) previously filled with chemically activated acrylic resin (Jet Clássico, São Paulo, Brazil) so that their buccal surfaces were perpendicularly positioned in relation to the cylinder base by using a 90-degree glass square. After inclusion, the samples were stored in distilled water and kept in refrigerator again until the day of bracket debonding. Next, the buccal surfaces were submitted to prophylaxis by using water, fluoride-free pumice paste (S.S. White, Petrópolis, Rio de Janeiro, Brazil), and a rubber cup (KG Sorensen, Barueri, São Paulo, Brazil) mounted on counterangle handpiece (Dabi-Atlante, Ribeirão Preto, São Paulo, Brazil) at low rotation during 10 seconds. The teeth were washed during 10 seconds and dried by applying air jet free of oil and humidity for 15 seconds. Following the prophylaxis, the samples were randomly divided into four groups (n = 15). The buccal surface of the teeth from all groups were etched with 37% phosphoric acid for 30 seconds, then washed and dried during 20 seconds. Next, the brackets were bonded to them according to the following groups: Group 1 (control) – Transbond XT was used according to the manufacturer’s recommendations: (1) application of XT primer on etched surface; (2) slight application of air-jet; (3) placement of composite on the bracket base; (4) the bracket was positioned on the centre of the buccal surface and pressured; (5) excess removal; (6) light-curing for 40 s (10 s for each face, i.e., mesial, distal, incisal and gingival) by using a XL 1500 light device (3M Dental Products, St. Paul, USA) with an intensity of 500 mW/cm2, regularly checked by means of a radiometer (Demetron, Danburry, CT, USA). Group 2 – Procedures: (1) Fluid resin “A” was mixed with fluid resin “B” and then applied on the etched surface; (2) slight application of air-jet; (3) Concise restorative composite (3M Dental Products, St. Paul, USA) was applied on the bracket base; (4) the bracket was positioned on the centre of the buccal surface and pressured; (5) excess was removed. Group 3 – Procedures: (1) Fluid resin “A” was mixed with fluid resin “B” and then applied on the etched surface; (2) slight application of air-jet; (3) Concise diluted restorative composite was applied on the base of the bracket; (4) the bracket was positioned on the centre of the buccal surface and pressured; (5) excess removal. The concise restorative composite was diluted by putting a single drop of fluid resin “A” on 1g of paste “A” and another single drop of fluid resin “B” on 1g of paste “B”. As the Concise restorative composite is commercially found in paste (6g recipients), six drops of fluid resin were dropped on each recipient of paste according to Artun and Zachrisson12. Group 4 – Procedures: (1) Fluid resin “A” was mixed with fluid resin “B” and then applied on the etched surface; (2) slight application of air-jet; (3) Concise Orthodontic composite (3M Dental Products, St. Paul, USA) was applied on the base of the bracket; (4) the bracket was positioned on the centre of the buccal surface and pressured; (5) excess was removed. Standard Edgewise upper central incisor metallic brackets (code 10.30.201, Morelli, Sorocaba, Brazil) were used for study and no angulations or torque were applied. The bracket base area was of 0.1402 cm2 with slot of 0.22 x 0.28. In the present study, pliers (Morelli, Sorocaba, SP, Brazil) were used in all bonding procedures and the material excess was removed by using an exploratory probe (Duflex, Juiz de Fora, MG, Brasil). Following the bracket bonding, the samples were stored in distilled water in stove at 37oC for 24 hours. Next, the samples were submitted to shear bond test by using a testing machine (Instron, Canton, USA) at a crosshead speed of 0.5 mm/min, with bracket debonding occurring through activated chisel point. Firstly, the shear bond strength values were recorded in kgf, and then in kgf/cm2 by the following formula: S = F/A, where S = shear bond strength, F = force necessary for breaking the bracket/tooth interface, and A = area of the bracket base (0.1402 cm2). The shear bond strength values in kgf/cm2 were transformed into MPa. After the debonding procedures, the buccal surface of each sample was evaluated by using an 8x stereoscopic magnifying glass (Carl Zeiss, Goettingen, Germany) in order to quantify the adhesive remnant index (ARI). The criteria used had been previously approved by Artun and Bergland19: 0 = no adhesive remaining; 1 = less than half of adhesive remaining; 2 = more than half of adhesive remaining; 3 = all adhesive remaining. The data on shear bond strength were submitted to both analysis of variance and Tukey’s test (5%), whereas the ARI scores were assessed by the Kruskal-Wallis test. Results Table 1 shows that the shear bond strength values for Groups 1 and 2 were higher than those from Group 3 (p< .05). No statistically significant difference was observed between Groups 1, 2, and 4 as well as between Groups 3 and 4 (p> .05). With regard to the adhesive remnant index, no statistically significant difference was observed among the four groups (p=0.089), as shown in Table 2. However, the ARI scores were found to be different within each group (Figure 1). In Groups 1 and 2, the ARI score of 2 was predominant. In Group 3, ARI score of 3 was predominantly seen, whereas in Group 4 a steady distribution of the ARI scores was observed. Discussion The Concise composite has been used by orthodontists as the material of choice for bonding orthodontic accessories to enamel. Such material is largely used in Orthodontics; it continues to be evaluated by numberless studies and serving as a reference for analysing other materials7,11. Several formulations involving the Concise composite were tested in the present study, namely, two proposed by the manufacturer (Concise restorative and Concise Orthodontic composites) and one suggested by Artun and Zachrisson13 (Concise Restorative Diluted Composite). Transbond XT composite was used as control. No statistically significant differences among Group 1 (Transbond XT), Group 2 (Concise RESTORATIVE) and Group 4 (Concise Orthodontic) regarding the shear bond strength (Table 1) were found. This similarity involving the Concise Restorative and Concise Orthodontic composites is not corroborated by the manufacturer’s information, since the latter penetrates into the bracket base more steadily due to its greater dilution, which increases the mechanical retention between bracket and tooth. Although the lack of such characteristic did not indicate the use of Concise Restorative composite for bracket bonding, this fact was not observed in our study. The lack of statistical difference found between Group 1 (Transbond XT) and Group 4 (Concise Orthodontic) is also corroborated elsewhere17-18. In Group 3, the Concise Restorative composite was diluted according to proposition by Artun and Zachrisson13, whose objective was to facilitate the mechanical imbrication of the material on the bracket base. Nevertheless, the results were found to be statistically inferior to both Transbond XT and Concise Restorative composites. This statistical similarity between Groups 1, 2, and 4, in addition to the differences regarding Group 3, reveals that, regardless of the viscosity of the material (diluted or not diluted), the pressure exerted on the bracket against the enamel during the bonding procedure enables the material to penetrate into the bracket mesh and enamel, thus yielding an adequate mechanical retention. With regard to the shear bond strength, we could observe that all the four groups showed higher mean values in comparison to those found by Reynolds20 for either laboratory (above 4.9 MPa) or clinical experiments (7.8 MPa), thus indicating the clinical usage of such materials. Therefore, the adhesion values found in the groups further showed that viscosity of the material did not interfere with bracket bonding. After the debonding procedures, the amount of composite adhered to the enamel was observed in accordance with the ARI scores (Artun and Bergland19). Such an evaluation is of crucial importance because the ideal ARI score following the bracket debonding is 3 (all adhesive remaining), thus meaning that the enamel would be protected against eventual fracture. Regarding the mean ARI values, no statistically significant differences were found among the four groups (Table 2). However, the ARI scores were found to be different within each group (Graphic 1). Most of the fractures seen in all groups involved the bracket/ composite interface and displayed remaining material adhered to the enamel following the debonding. In accordance with other studies3,6,11, both Groups 1 and 2 showed ARI score of 2 predominantly, thus meaning that half of the composite had been adhered to enamel following the bracket debonding (Figure 1). In Group 3, ARI score of 3 (all adhesive remaining) was not so predominantly seen, and four samples had showed ARI score of 0 (no adhesive remaining), as evidenced by fractures in the enamel/composite interface during the bracket debonding (Graphic 1). On the other hand, however, Group 4 showed a steady distribution of the ARI scores, which was not seen in other groups (Figure 1). Concluding, the Concise diluted restorative composite was found to have shear bond strength values inferior to those from Transbond XT and Concise restorative composites and all tested Concise composites had adequate adhesive values for clinical usage. Moreover, after the bracket debonding, no statistically significant difference was observed between the four groups regarding the ARI scores, and most of the samples showed remaining material adhered to the enamel. References
© Copyright 2007 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os07040t2.jpg] [os07040t1.jpg] [os07040f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}