 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 6, No. 23, October-December, 2007, pp. 1467-1469 Clear cell myoepithelioma of the hard palate A.K. Agarwal1 Ashwani Sethi2 Shamit Chopra3 Deepika Sareen3
1MS, Director, Professor 2MS, Senior resident 3MBBS, Junior Resident Department of ENT & Head and Neck Surgery, Maulana Azad Medical College and associated
L. N. Hospital
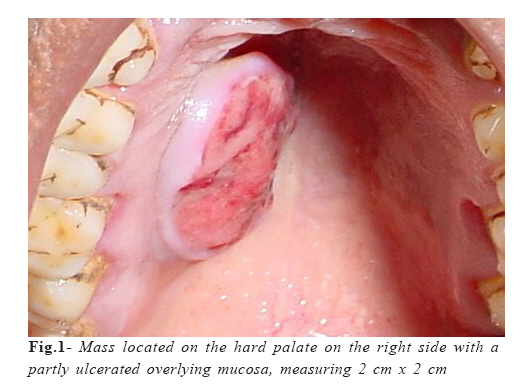
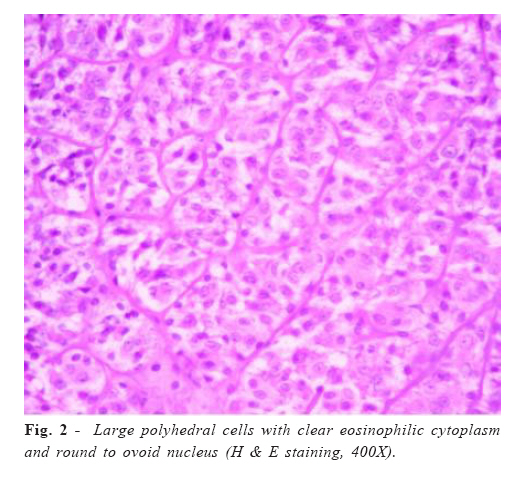
Received for publication: August 7, 2007 Accepted: November 11, 2007 Code Number: os07042 Abstract Salivary gland myoepitheliomas are rare tumours. We report the case of a 40-year-old female who presented to us with a hard palatal mass. The tumour was excised with a healthy rim of surrounding tissue. Histological and immunohistochemical analyses revealed the tumour to be a myoepithelioma of the clear cell variety. Key words: myoepithelioma; hard palate; salivary gland tumours; minor salivary gland Introduction Myoepithelial cells are contractile cells derived from ectoderm and are seen in major and minor salivary glands, lacrimal glands, breast, sweat glands and prostate1. These cells are thought to be responsible for expulsion and propagation of secretions from the acini and through the ductal network of these tissues. These cells may assume several distinct forms- as a spindled, plasmacytoid, clear, stellate or a basket-like cell2. The tumours arising exclusively from these cells are rare and account for less than 1% of all salivary gland tumours3. Most of these tumours have been reported in the parotid gland and minor salivary glands on the hard palate4. Although, clear cell myoepitheliomas have been reported at other sites5-8, most of the cases of palatal myoepitheliomas have been plasmacytoid or spindle cell type9. We did not find any report of a clear cell myoepithelioma of the hard palate in the review of medical literature. The extreme rarity of such an occurrence prompted us to report this case. Case report A 40-year-old female presented to us with a palatal mass of 6 months duration, which has been gradually increasing in size and was painless. The patient had no other significant complaints. The patient had history of chewing tobacco for the past 15 years. Examination of the oral cavity revealed a firm, non-tender, well-circumscribed mass located on the hard palate on the right side, measuring 2 cm x 2 cm with a partly ulcerated overlying mucosa (Figure 1). Nicotine stains could be seen on the teeth. The patient had no trismus or cervical lymhadenopathy. Routine hematological and urine analyses and chest X-ray were normal. ELISA for HIV was non-reactive. A fine needle aspiration cytology (FNAC) of the tumour revealed a cellular minor salivary gland tumour suggestive of a pleomorphic adenoma. An enbloc excision of the tumour with a rim of surrounding normal mucosa was performed and subjected to histopathological evaluation. The postoperative period was insignificant and the patient is totally asymptomatic for the disease without any signs of recurrence one year postoperatively. The specimen consisted of a firm, circumscribed tumour with a smooth external and a solid tan cut surface. On light microscopy, it was found to be surrounded by a thick fibrous capsule. The tumour was uniformly composed of large polyhedral cells with glassy, clear eosinophilic cytoplasm arranged in closely packed interlacing bundles (Figure 2). The nuclei were round to oval, eccentrically placed and were vesicular with small nucleoli. Immunohistochemically, the clear cells were immunoreactive for cytokeratin, S-100 and muscle specific actin (MSA) and non-reactive for epithelial membrane antigen (EMA), vimentin and carcinoembryonic antigen (CEA). A final diagnosis of clear cell myoepithelioma of the hard palate was made. Discussion Myoepitheliomas are rare, generally benign tumours with the parotid gland and palate accounting for three-fourths of all cases2. The age range is wide, and there is no significant gender predisposition of this tumour2,4. The plasmacytoid variant appears to have a predilection for the palate in slightly younger individuals, while the spindle cell type tends to occur in the parotid gland of older individuals5-6. On the other hand, clear cell tumours of the salivary glands are almost invariably malignant in nature, with rare exceptions in the form of myoepitheliomas and oncocytomas6. When benign, the tumour most often presents as an asymptomatic mass that slowly enlarges over a course of several months to years. Parotid lesions never produce facial dysfunction and those of the palate rarely ulcerate2. Our patient had a history of 6 months with a partly ulcerated, slowly growing mass. Pathologically, myoepitheliomas vary from 1 to 5 cm in greatest dimensions and are well demarcated with a smooth, sometimes bosselated external appearance and a uniform white, tan or gray cut surface. They are generally encapsulated except for palatal myoepitheliomas, which may or may not have a capsule2. In or patient, the tumour measured 2 cm x 2 cm and was encapsulated. Microscopically, primarily spindle-shaped cells, occasionally plasmacytoid cells, or a combination of these two cell types constitute these tumours, being the stellate and clear cell variants rare2. Immunohistochemically, a large number of markers have been used for establishing the diagnosis of myoepitheliomas. The myoepithelial cells are usually found to be immunoreactive to S-100, actin and prekeartin, and are non-reactive to desmin and EMA. Other markers that have been used in some reports are CEA, secretory piece, high molecular weight keratin, cytokeratin and factor VIII antigen9. The reactivity to MSA and vimentin has been reported variably in different reports2,4,10. In our patient, the tumour cells were found to be immunoreactive to MSA, S-100 and cytokeratin and negative for vimentin and EMA. There is a close correlation between histological appearance and prognosis. Tumours showing a more aggressive behaviour are mitotically active, more anaplastic and contain fewer myofilaments. Cellular pleomorphism, increased mitotic activity, necrosis and invasion indicate towards possibility of malignancy2. These features were absent in our case. Wide local excision with a rim of surrounding normal tissue is considered the treatment for myoepitheliomas. Our patient also underwent similar treatment without any evidence of recurrence one year following the surgery. Myoepitheliomas of the salivary glands are uncommon tumours with clear cell variants still rarer. In our review of medical literature, we did not come across any report of a palatal clear cell myoepithelioma. The diagnosis of these tumours is based on a combination of routine microscopy as well as immunocytochemistry. The treatment is surgical with wide local excision. In conclusion, myoepitheliomas are rare benign tumours arising from myoepithelial contractile cells present in minor and major salivary glands. These tumours are difficult to diagnose on routine histochemical staining and require immunohistochemical staining for diagnosis. The clear cell variants of myoepitheliomas are extremely rare on the palate with no case reported in the pertinent medical literature in the past. Wide local excision is usually curative. References
© Copyright 2007 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os07042f1.jpg] [os07042f2.jpg] |
| |||||||||

{kind=link}
{kind=link}