 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
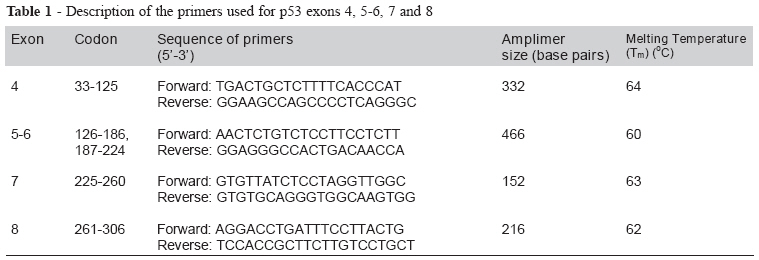
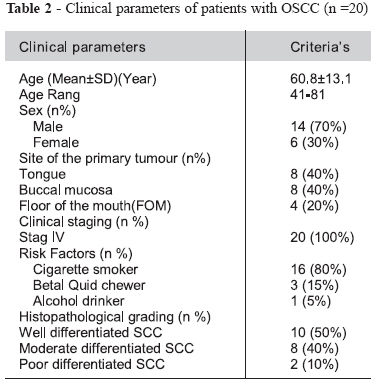
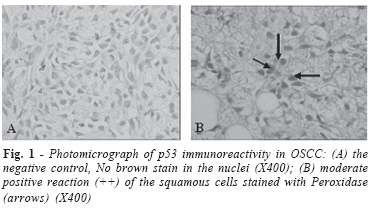
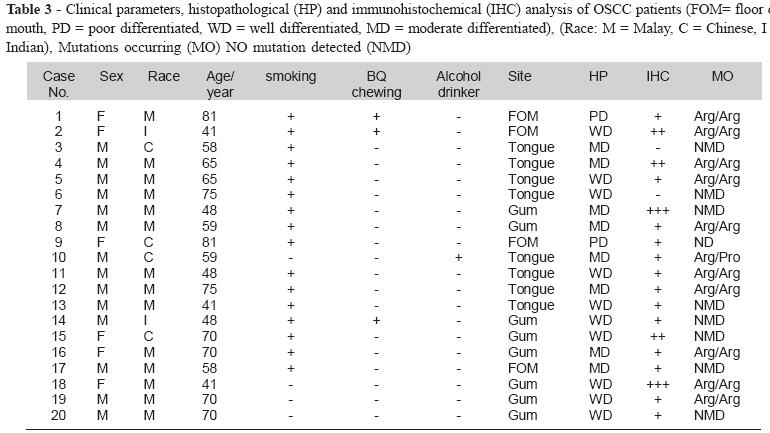
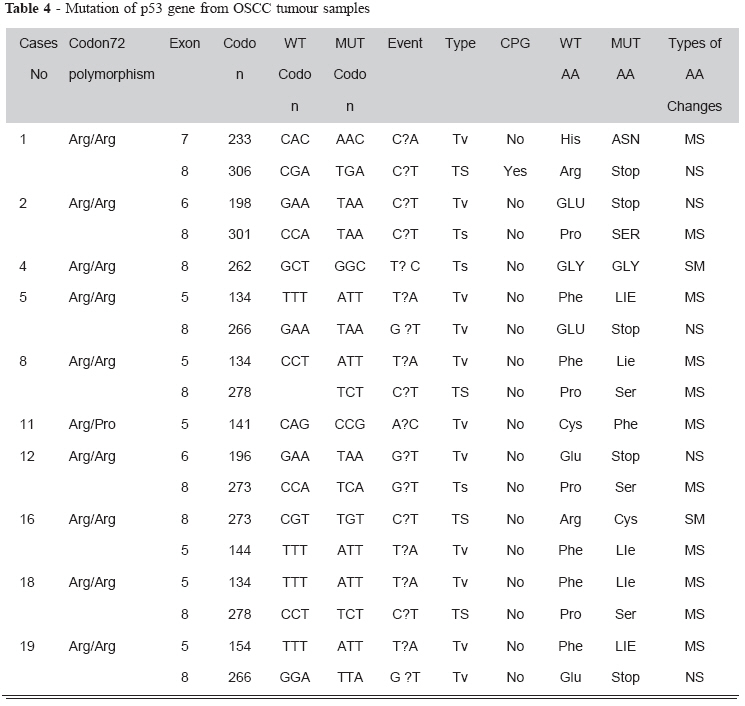
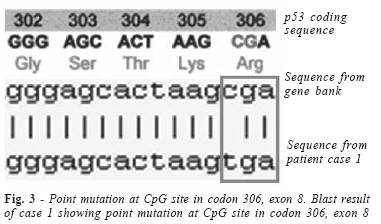
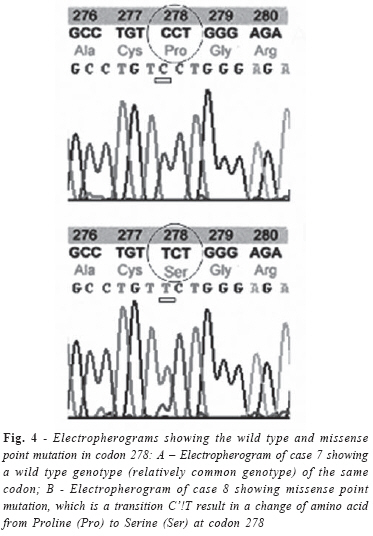
Brazilian Journal Oral Sciences, Vol. 7, No. 24, Jan/Mar 2008, pp. 1476-1483 Immunohistochemical and molecular genetic analysis of p 53 in oral squamous cell carcinoma (scc) in Hospital University Science Malaysia: a preliminary study Karima Akool Al-Salihi1, S. L. Ang1 , A. Azlina2 , M.S. Farini2 , H. Jaffar3 1School of Dental Sciences, Received for publication: August 19, 2007 Accepted: March 27, 2008 Code Number: os08002 Abstract The role of p53 mutation in oral cancer cases has not been studied in Malaysia. This study was designed to focus on over expression of p53 nuclear protein and gene mutation in oral squamous cell carcinoma (SCC) cases in Hospital University Science Malaysia (HUSM). Twenty randomly selected cases previously diagnosed as oral SCC lesions in HUSM since 2002 were included in this study. Patient’s folders were reviewed to study clinical history and tumor staging. Extracted DNA amplified using PCR. Gene sequencing had done to detect genetic mutation. Protein overexpression detected using the Streptavidin-biotin Peroxidase technique. P53 gene mutations, analyzed within exons 5- 8, were observed in 10 out of 20 cases (50%) of oral SCC. The positive nuclear staining by immunohistochemical was observed in 18 cases (18/20, 90%). These data indicate the highly incidence of p53 protein overexpression as well as specific mutations in oral SCC patients in Malaysia. However this preliminary study had been based on analysis of relatively few cases of oral squamous cell carcinoma, so further study require to including large number of cases from different states in Malaysia. Key words: p53, SCC, immunohistochemical, mutation, PCR Introduction Oral cancer is the 11th most common cancer in the world1,2 and more than 90% are oral squamous cell carcinoma3,4. Human cells become malignant through the activation of oncogenes, which stimulate cell proliferation, inactivation of tumour suppressor genes. DNA repair genes lead to progression genetic instability resulted in uncontrolled growth, and loss of differentiation, invasion and metastasis1- 5. p53 tumor suppressor gene (TSG), as the guardian of the genome6 plays two major important roles as a “gatekeeper” in control the pathways of cell proliferation and ‘caretaker’ in DNA repair and maintain genetic stability. TSG are typically inactivated by gene mutations in one allele, followed by loss of the intact allele during cell replication lead to loss of suppressor function1. Thus, p53 mutation appears to be the most frequent genetic event7,8. According to the p53 mutation database R10 (July, 2005), 21,587 somatic mutations and 283 germline mutations have been reported9. As far as we are aware, there are no documented publications available for p53 mutation in the oral carcinogenesis in Malaysia. The aim of this study is to detect the p53 genetic alteration in the conserved region of the P53 gene in OSCC patients by polymerase chain reaction (PCR) and direct sequencing as well as to evaluate the over expression of p53 in oral SCC using immunohistochemical test. Materials and Methods Patients and study design Twenty cases were randomly selected from the list of oral cancer patient in the DNA library /Human Genome Center/ University Science Malaysia (USM). For each case, a pair of tumor and normal adjacent non-tumor tissue samples were surgically dissected into small pieces, frozen immediately in liquid nitrogen and stored at -80 0C. Whole surgically removed samples were sent to the department of pathology for histopathological diagnosis. Histopathological changes were categorized as well differentiated squamous cell carcinoma, moderate differentiated squamous cell carcinoma and poor differentiated squamous cell carcinoma. The inclusive criteria were primary tumor diagnosed as Oral Squamous Cell Carcinoma under International Classification of Disease, ICD10 (C00-C04) or ICD-9 (140.0-141.9, 143.0-144.9). On the other hand, the exclusive criteria were past history of cancer at other site of the body. This study was approved by the Ethical and Research Committee of University Science Malaysia. Patients already signed inform consent form prepared previously by the Malaysian National Oral Cancer Group. Data collection was done from the patient folders at record unit, Hospital USM. Immunohistochemical staining Immunohistochemical staining was performed according to strept-avidin-biotin peroxidase complex (ABC) method10. Briefly, 4 ìm sections from paraffin embedded specimens were deparafffinized with xylene and rehydrated with graded ethanol. Epitope retrieval (antigen retrieval) was done by incubating the sections in 10mM sodium citrate buffer (pH 6.0) for 20 minutes in a conventional microwave-oven. The endogenous peroxidase activity was blocked by immersing the sections in methanol with 0.3% hydrogen peroxide. Mouse Anti-Human p53 Protein (DO-7) (Dakocytomation, Cat# M7001) diluted 1:300 in primary antibody dilution buffer. Sections were incubated with diluted primary antibody overnight at 4 0C, followed by incubation with a biotinylated anti-mouse secondary antibody and streptoavidin-biotinperoxidase complex (labeled Streptavidin Biotin Kit, Dako). The peroxidase reaction was developed using diaminobenzidine (DAB) as a chromogen. The sections were counter-stained with hematoxylin solution. For negative controls, primary antibody was replaced with 0.05M Tris -HCL buffer solution (PH 7.6). The slides were then viewed using a ZEISS microscope with an Image Analyzer. Immunostaining for p53 positive cases were graded as negative (-) no nuclear staining, mild positive (+) if fewer than 10% of nuclear were stained, or moderate positive (++) if more than 10% of nuclear were stained and strong positive (+++) if more than 50% of the nuclear were stained. DNA Extraction Single-strand conformation polymorphism analysis was used to analyze all tumor samples for mutations within exons 5-8 of the p53 gene. Cases, which were displaying an altered electrophoretic mobility, were re-amplified in another separate reaction. High molecular weight DNA was purified by digestion with proteinase K and extraction in phenolchloroform. The primers used for exon 5-8of p53 showed in Table 1. T m was calculated using the formula, Tm = [4(G+C)+2(A+T)] 0C. DNA samples (100 ng) were subjected to PCR in a mixture (10 ìl) using two appropriate oligonucleotides as primers as described previously. The PCR mixture heated to 95oC with an equal volume of formamide dye mixture (95% formamide, 0.05% bromophenol blue, 0.05% xylene cyanol, 20mM EDTA); 2ìl of the preparation was applied to a 6% polyacrylamide gel, both with and without 10% glycerol. Electrophoresis was performed at 70W for 1.5 hour. The gel was analysed under UV light using Chemilmager Analyzer 4400 (AlphaInnotech Corp., USA). DNA purification was done using Wizard® SV Gel and PCR Clean-up System (Promega, USA) according the protocol provided by the manufacturer. It involves three main steps, which are binding of DNA, Washing and Elution. The purified PCR product (DNA) in the collection tube was stored at -20°C. The concentration of purified PCR product measured at 260nm using spectrophotometer (Eppendorf BioPhotometer, USA). Direct DNA sequencing was done. The PCR was treated with 1 ì g of genomic DNA, 200 ng of each primer, 200 ìM dNTPs, 1 X PCR reaction buffer, 2.5 U Taq polymerase. Aliquots of PCR amplified mixtures diluted with 2ml of distilled water and spun in a centricon 30 microconcentrator to remove the excess primers and dNTPs. DNA was then resuspended in 50 ìl of 10 mM Tris pH 8.0 and 1 mM EDTA and direct sequencing were done followed the instructions of the Promega fmol TM DNA sequencing system technical manual. The sequencing results were analysed. Obtained results were BLAST by align each sequence with the p53 sequence (code 35213) at the gene bank at http:// www.ncbi.nlm.nih.gov/BLAST/Blast.cgi, Align two sequences. The results were further analyzed using DNA software Chromas Version 1.62 (32-bit). The codon and amino acid was check by referred to the p53 CODING SEQUENCE from IARC TP53 DATABASE - TP53 coding sequence, www.iarc.fr/p53. The presented mutation was confirmed by comparing with the International Agency for Research on Cancer (IARC) TP53 Database which is a database consisting of the p53 mutation reported in the world. The reference to other cancer was done when no cases was found to be compatible with the result in head and neck cancer. Results Population characteristic and clinical parameters Archival representative blocks from the primary tumours were available for 20 patients included in this study. The demographic data and review of all patients’ folders are shown in Table 2. The study included 14 male and 6 female. The patient races were 14 Malay, 4 Chinese and 2 Indian. The mean age (rang 41- 81 years) is 60.8±13.1 years. 90% of the patients had exposed to at least 1 of the risk factors for oral cancer. 80% (16/20) of the patients smoked, 15% (3/20) chewed betel quid and 5 % (1/20) were alcohol user. The patients included in this study showed considerable variation in histopathological appearances of oral SCC, according to their histopathological features as follow: ten patients showed typical features of well differentiated squamous cell carcinoma, eight patients showed histopathological features of Moderate differentiated squamous cell carcinoma and only two patients showed histopathological features of poor differentiated squamous cell carcinoma. Immunohistochemical analysis p53 positive immunoreactivity reaction was indicated by brown nuclear staining. Eighteen cases were revealed positive over expression reaction for p53 (Fig. 1 A, B). Thirteen patients of these cases revealed mild positive reaction for p53 and only two cases showed strong positive reaction, which appeared as dark, brownish nuclear stained. While three cases showed moderate reaction. Two cases were negative for p53. All negative control sections revealed no brown colour stain and the nucleus were stained with the haematoxylin counter stain. Clinico-pathological parameters in relation to the over expression of p53 are summarized in table 3. Molecular genetic analysis Eighteen p53 mutations were occurring in 10 OSCC patient’s tumour tissue samples (50%) in exons 5-8. A total of 18 point mutations occurred in 10 out of 20 cases (50%). All the mutations were point mutation which presented as 11 missense mutation (61.11%), 5 nonsense mutation (27.77%) and 2 silent mutation (11.11%). Table 4 showed the mutations occur in exon 5-8. Figure.2 shows an electropherogram for confirmation of the amplified PCR product (Amplier). BLAST result of case 1 represented in Figure.3 revealed point mutation at CPG site in codon 306, exon 8. Figure.4 represented the electropherogram of selected cases (7 and 8) showing a wild type genotype (relatively common genotype) of the same codon in case 7 and missense point mutation,in case 8 which showed a transition of C to T resulted in a change of amino acid from Proline (Pro) to Serine (Ser) at codon 278. Discussion Oncogenes alone are not sufficient to cause oral cancer and appear to be initiators of the process. The crucial event in the transformation of a premalignant cell to a malignant cell is inactivation of cellular negative regulators—tumor suppressor genes—and is regarded to be a major event leading to the development of malignancy. Tumor suppressor genes are most often inactivated by point mutations, deletions, and rearrangements in both gene copies11,12. The importance of the p53 tumor suppressor gene in the process of carcinogenesis is well established. The p53 protein blocks cell division at the G1 to S boundary, stimulates DNA repair after DNA damage, and also induces apoptosis. These functions are achieved by the ability of p53 to modulate the expression of several genes13,14. The p53 protein transcriptionally activates the production of the p21 protein, encoded by the WAF1/CIP gene, p21 being an inhibitor of cyclin and cyclin dependant kinase complexes15. p21 transcription is activated by wild-type p53 but not mutant p5316. However, WAF1/CIP expression is also induced by p53 independent pathways such as growth factors, including platelet derived growth factor, fibroblast growth factor, and transforming growth factor ß17. Wild-type p53 has a very short half life (four to five minutes)18, whereas mutant forms of protein are more stable, with a six hour half life19. In the developed world, about 30% of all oral cancer affects the lip and has a more clearly defined aetiology (mainly exposure to sunlight) and a better prognosis than intra-oral cancers. In this study, the entire patient’s lesion is from intra oral, which include tongue, buccal mucosa and floor of the mouth. All patients presented with advance clinical staging (Stage IV). This clinical presentation for the patient in this study is compatible with previous observation described by other researchers. They found that most mouth cancers are asymptomatic or presented with minimal pain at early stages20, which lead to delay in seeking professional care4. In this study 18/20 patients were presented with nodal metastasis, which revealed higher frequency than previous studies reported in literature20.The results of this study showed that patients had exposed to at least 1 of the risk factors for oral cancer. 80% (16/20) of the patients smoked, 15% (3/20) chewed betal quid and 5% (1/20) were user of alcohol. These suggest that smoking and betal quid chewed play an important role in the development of oral cancer. The results of this study are compatible with others. Other studies explained that specific risk factors, i.e. tobacco, betel quid and alcohol may contain or are metabolized to several known carcinogens, which are extremely important in oral mutagenesis3. Other study found that the primary cause of high incidence in Asians is the widespread habit of chewing betel quid, deficiency of antioxidant micronutrients such as P carotene and vitamin C and some viruses, such as HPV (types 16 & 18)20-48. Most population of this study showed low prevalence of drinking habit due to religion reason. There are totally eighteen p53 mutations occurred in 10 OSCC patient’s tumour tissue, (50%) (10/20patients) with point mutation, occur in exon5-8, with predominance in exon 8. This percentage (50%) of mutation is relatively compatible with the results found previously by other researcher21, they found p53 mutations in 42% of the patients (54 of 129). All the mutations have been reported by other studies. Eight out of 18 mutations have been observed in previous studies in head and neck cancer22-34. The other 4 was observing in studies of gliomas, keratosis, ulcerative colitis and acitinic keratoses35. This result suggests that the mutation occur is site specific. The most prevalent mutation found in this study was C to T transition, which occurred in 6 of 18 mutations (33.33%). The mutation in codon 306 was at the CpG site, where cytosines that were located next to a guanine (5’-CpG-3’)36. C>T mutations occur frequently at CpG sites by endogenous mechanisms, which were hydrolytic deamination and enzymatic deamination. Other studies showed that many of the genes associated with methylated CpG islands could be reactivated in cell lines by experimental demethylation using 50-aza-20 deoxycytidine36. Codon 278 is one of the residual conserved areas for p53 mutation. There are no direct structural explanations for many of these, one can assume that they are conserved throughout evolution for a good reason and, in the case of surface residues; this is likely to be that the amino acid is critical for interactions with other proteins37. Regarding codon 72 polymorphism, the Arg/Arg, Arg/Pro and Pro/Pro genotype frequencies were 70%, 20 and 10% respectively. The Arg/Arg genotype frequency is high compare to previous studies reported as 52 % in SCC head and neck (SCCHN) patient and 52.6 % for the control group as reported previously38 and 52% in SCCHN and 50% in control group. This might suggest that Arg/Arg have role in oral carcinogenesis in advance stage. This is contradicting with others39 . This suggests that arginine allele appears to protect against head and neck cancer. However, several studies show that p53 Arg/Arg variant individuals were seven times more susceptible to develop human papilloma virus (HPV) associated cervical cancer but both confirm and contradicted by several groups39. Studies in OSCC or SCCHN suggested that there was no difference in the distributions of p53 codon 72 genotypes between cases and controls but Pro allele was associated with an early onset of cancer38, which is contradict with the pro allele patient in this study who have late onset of cancer. p53 protein expression as detected by immunohistochemical does not always reflect the presence of mutant p53 protein, and neither does the absence of p53 staining preclude it . In this study 18 cases showed positive p53 immunoreactivity and only 2 cases were negative reaction. All cases with gene mutation showed p53 protein overexpression. This showed there is some good relationship between immunohistochemical detection of p53 protein and the presence of mutations within the p53 gene. On the other hand, 8 cases revealed positive reaction for p53 protein immunoperoxidase overexpression with no gene mutation detection. There is also controversy about the relation between p53 mutation and detection of the p53 protein by immunocytochemical. Some authors have suggested a high correlation between p53 expression and point missense mutation40, whereas others have reported some discrepancy in oral cancer, with lack of expression demonstrated by immunocytochemical having been attributed to insensitive methods of detecting p53 mutation, or the existence of truncating mutations that result in the absence of protein41 43. However, stabilisation of p53 and detection by immunocytochemical might not necessarily be the result of mutation. In Li-Fraumeni syndrome, p53 is mutant but the protein is unstable, like the wild-type p53 protein, which suggests that some other event may be necessary for stabilization , and that stability of p53 is not intrinsic to the mutant p53 structure, but might vary in different cell backgrounds43,44. In this study 2 cases were negative for p53 immunoreactivity. It is used base on the principle that normal p53 protein only has half life of 15 to 20 min and the mutated p53 have a longer half life45. The short half life is control by feedback loop. The p53 protein bind to MDM2 gene to stimulate the MDM2 protein synthesis, and the MDM2 protein will bind to p53 protein and stimulates the addition of ubiquitin groups to the protein and cause it degradation46. This is the reason for p53 protein to undergo stabilization without any mutation after exposure to DNA damage agent or functional inactivation by the binding of the p53 protein to other viral or cellular proteins. Where the feedback loop is diminish and cause accumulation of p53 protein. In addition immunohistochemical has a number of disadvantages, including the fact that any mutations that abolish p53 expression (splicing signal mutations, nonsense mutations, insertions or deletions) do not produce the protein and therefore give a negative result. In conclusion this study revealed high prevalence of p53 mutation in the OSCC patient with advance clinical stage with good relationship to the immunohistochemical result, which revealed high prevalence of p53 protein overexpression. Acknowledgments We thank Puan Bizzura BT Abdoulgani for helping us with preparation of all histological sections. This work was supported by project number CDC M3/001 from Academy of Sciences Malaysia. There was no any conflict of interest in connection with this study. References
© Copyright 2008 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os08002t3.jpg] [os08002f3.jpg] [os08002f4.jpg] [os08002f2.jpg] [os08002f1.jpg] [os08002t1.jpg] [os08002t4.jpg] [os08002t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}