 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
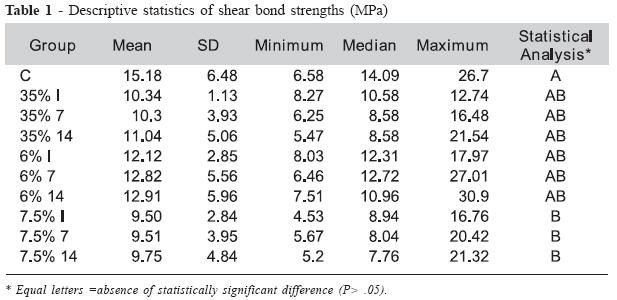
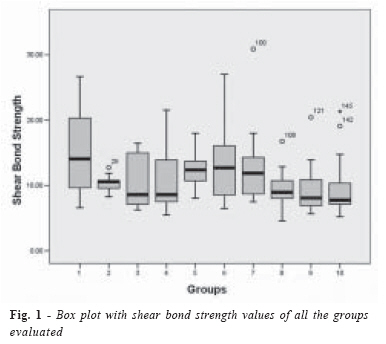
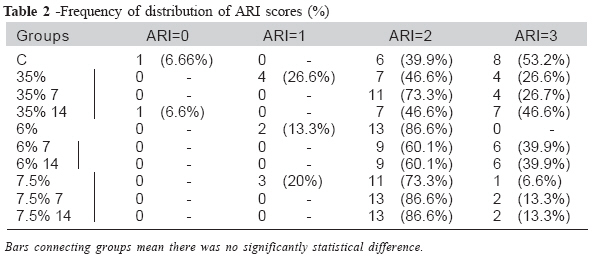
Brazilian Journal Oral Sciences, Vol. 7, No. 24, Jan/Mar 2008, pp. 1483-1488 Effect of bleaching with hydrogen peroxide into different concentrations on shear strength of brackets bonded with a resin-modified glass ionomer Matheus Melo Pithon1 Antônio Carlos de Oliveira Ruellas2 Eduardo Franzotti Sant’anna2 1DDS, Undergraduate Student 2DDS, MS, PhD, Professor Department of Orthodontics and Pediatric Dentistry, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil Received for publication: August 29, 2007 Accepted: March 28, 2008 Code Number: os08003 Abstract The evolution in glass ionomer cements has contributed to the reduction in dental caries in orthodontic patients because of the biological and chemical characteristics of this material; however no studies in the literature have evaluated the effect of bleaching treatment on the bond strength values of resin-modified glass ionomer cements (RMGICs). This study assessed the effect of a 6, 7.5 and 35% hydrogen peroxide bleaching gel on shear bond strength and bond failure site of brackets bonded with a resin-modified glass ionomer (Fuji Ortho LC, GC Europe, Leuven, Belgium). One hundred-fifty bovine mandibular permanent incisors were randomly divided into 10 groups; each group contained 15 teeth. Bleaching treatment was performed immediately at 2 different times before the bonding procedure. One hundred-fifty stainless steel brackets were bonded with the resin-modified glass ionomer. Following, all samples were stored in distilled water for 24 hours and then tested in shear mode on a Instron machine. ANOVA and Tukey’s test showed statistical differences between the groups whose teeth were treated with 7.5% hydrogen peroxide and the control group. However, no statistical differences were found for the other groups (P > 0.05). With respect to adhesive remnant index (ARI), the majority of fractures occurred at the bracket/composite interface. Despite the decreased shear bond strength, the bonding of teeth whitened with different concentrations of hydrogen peroxide was found to be strong enough to resist mechanical and masticatory forces. Key words: Tooth Bleaching; Orthodontic Brackets; Glass Ionomer Cements; Hydrogen Peroxide Introduction In Orthodontics, the white spot lesions and marginal gingivitis worry most practitioners; as a result, they are well aware of the new materials for minimizing and preventing such lesions. Among these materials, the glass ionomer cement stands out from all the others. The evolution in glass ionomer cements has contributed to the reduction in dental caries in orthodontic patients because of the biological and chemical characteristics of this material1. The recent popularity of tooth whitening or bleaching has a significant impact on the practice of dentistry2. Several whitening systems are currently being used to bleach enamel3. Amongst the whitening systems commonly used today at low and high concentrations, we can cite the hydrogen peroxide-based ones used at home and in office, respectively. The increased use of hydrogen peroxide system is due to the smaller size of its molecules compared to those of carbamide peroxide. As a result, hydrogen peroxide molecules are more likely to move easily and quickly within the gel matrix, which provides greater osmotic pressure on the tooth/ gel interface and accelerates the diffusion of peroxide into the dental structure. Because peroxide penetration into the dental structure is one of the phases determining the speed of whitening process, one can conclude that the faster the peroxide penetration, the faster is the whitening process3. Hydrogen peroxide can move through the tooth structure for effective stain removal4. This is possible because of its low molecular weight and its capacity to denature proteins; this increases tissue permeability and allows ions to move through the teeth5. Hydrogen peroxide releases free oxygen radicals, which can cause cellular change6. The use of hydrogen peroxide-based tooth-whitening materials has increased substantially in the past few years, despite many unanswered questions about their use7. There have been controversial reports regarding the interaction between bleaching agents and bond strengths of composite materials to enamel. Some authors reported significant decreases in the average bond strength of composite to bleached enamel compared with unbleached enamel8-9. However, others found no significant differences in composite bond strengths between bleached and unbleached enamel4,10. So far, to our knowledge, no studies in the literature have evaluated the effect of bleaching treatment with different concentrations of hydrogen peroxide on the bond strength values of resin-modified glass ionomer cements (RMGIC). Therefore the purpose of this study was to assess the effect of bleaching at 3 different concentrations of hydrogen peroxide (6, 7.5 and 35%) on shear bond strength and bond failure pattern of orthodontic brackets bonded with an RMGIC (Fuji Ortho LC, GC Europe, Leuven, Belgium). Material and Methods One hundred-fifty freshly extracted bovine mandibular permanent incisors were collected from a local slaughterhouse and stored in a solution of 0.1% (weight/ volume) thymol for a week. The criteria for tooth selection included intact buccal enamel with no cracks caused by the extraction forceps and no caries. After extraction, all enamel surfaces were examined under a light stereomicroscope (Olympus SZ2-ILST, Beijing, China) at 10 times magnification. The teeth were cleansed of soft tissue and inserted into polyvinyl chloride tubes PVC (Tigre, Joinville, Brazil) reducing bushes (Tigre, Joinville, Brazil) filled with acrylic resin (Clássico, São Paulo, Brazil) with only their crowns kept exposed. The buccal surfaces of the crowns were perpendicularly positioned to the shearing die’s base using a Glass square to enable proper mechanical test. After polymerizing of the resin, all samples were stored in distilled water and kept again in the refrigerator (80C). The teeth were randomly assigned into 10 groups containing 15 specimens each, by using random number tables. Each group contained 15 specimens: Group C (Control): no whitening treatment was performed. Hydrogen peroxide at concentrations of 6% and 7.5% (White Class 6%, and 7.5% FGM, Santa Catarina, Brasil), mostly used in at-home tooth whitening, was applied using individual moulds made of acetate and a vacuum plasticizer (Bioart, São Paulo, Brazil) in order to spread the material uniformly on the dental surface. After preparing the acetate mould, the teeth were whitened over a 14-day period with the material being used 8 hours a day. The bleaching agent was changed every day after the bleaching cycle was completed. In the groups using 35% hydrogen peroxide (Whiteness Hp Maxx 35%, FGM, Santa Catarina, Brasil) the whitening gel was spread on the buccal face of the teeth according to the manufacturer’s recommendations. One minute later, the whitening agent was exposed to a light-emitting diode (LED) Radii (SDI Limited, Victoria, Australia) device during two 20second cycles with 1-minute interval. Following the LED exposure, the whitening material was maintained on the dental surface for more than 5 minutes, as suggested by the manufacturer. The time interval between the treatment sessions was 7 days, thus totaling three whitening sessions for each group. After the whitening procedure, one hundred-five stainless steel maxillary central incisor brackets (Abzil Lancer, São José do Rio Preto, Brazil) were bonded by one operator. The average area of bracket base surface was determined to be 13.8 mm2. All teeth were cleaned with a mixture of water and pumice by using a rubber polishing cup, rinsed with water to remove the pumice, and dried with oil-free air. After prophylaxis, phosphoric acid at concentration of 37% was used for etching the teeth during 20 seconds and then the teeth were washed and dried for the same period of time. Next, the bonding procedure was performed. For all groups, the brackets were bonded with RMGIC (Fuji Ortho LC, GC Europe, Leuven, Belgium) following the manufacturer’s guidelines. The adhesive-filled Fuji Ortho LC capsule was activated by manual squeezing and triturated for 10 seconds at 4000 rpm. The capsule was then loaded into an application gun, and the adhesive was squeezed onto the bracket base. The brackets were positioned on the teeth near the center of the facial buccal surfaces with sufficient pressure to express excess adhesive, which was removed from the margins of the bracket base with a scaler before polymerization. The RMGIC were lightcured for 40 seconds with a halogen light (Ortholux XT, Unitek/3M, Monrovia, Calif; light intensity was 470 mW/cm2), 10 seconds each at the mesial, distal, gingival, and occlusal margins. Light intensity was measured and checked throughout the study with a radiometer (Demetron, SDS Kerr, Danbury, Conn). After bonding, all samples were stored in artificial saliva at 37°C for 24 hours and then tested in shear mode on a universal testing machine (Instron 4411, Canton, Mass). For shear testing, the specimens were held in the lower jaw of the machine so that the bracket base of the sample paralleled the direction of the shear force. The specimens were stressed in an occluso-gingival direction with a crosshead speed of 1 mm per minute, according to previous studies11-12. The maximum load (N) necessary to debond or initiate bracket fracture was recorded, after converted into MPa as a ratio of maximum load (N) by bracket surface area. After the mechanical test, the buccal surface of each sample was evaluated by the same operator using a stereoscopic magnifying glass (Carl Zeiss, Goettingen, Germany) at 8X magnification, so that the Adhesive Remnant Index (ARI) could be quantified according to the criteria established by Artun and Bergland13 as following: 0 = no adhesive left on the enamel surface Statistical analysis was carried out with the SPSS 13.0 Program (Apache Software Foundation, Chicago, Illinois). Descriptive statistics that included mean, standard deviation, median, and minimum and maximum values were calculated for the 10 groups. Analysis of variance (ANOVA) was applied to determine whether significant differences existed among the groups. For the post-hoc test, the Tukey’s test was run on the data. Kruskal-Wallis test was used for assessing the ARI scores. Results The descriptive statistics for the shear bond strengths of the 10 groups are given in Table 1. Significant difference was observed between groups C and 7.5% I (p=0.027), C and 7.5% 7 (p=0.028) and C and 7.5% 14 (p=0.042). No significant differences (p>0.05) were found among others Groups (Figure 1). The ARI scores for the 10 groups are listed in Table 2. There was no significant difference between following Groups: Group C and groups 35% I, among 35% Groups, between groups 6% 7 and 6% 14, and among groups 7.5% (p>0.05). The most of the breakings had occurred between the RMGIC and bracket. Discussion Little is known about the effect of hydrogen peroxide over the long term14. There has been a concern that vital bleaching could alter the surface topography of enamel and thus affect the bond strength of adhesives to enamel15-16. Alterations in bond strength might be significant with regard to clinical operative procedures that involve composite resin bonding, such as bonding orthodontic brackets, porcelain veneers, composite veneers or future composite restorations17. A previous evaluation assessed the shear bond strength of brackets bonded to enamel with resin-modified glass ionomer cement and which had been previously whitened with 35% hydrogen peroxide11. Nevertheless, the long-term effect of low concentrations of hydrogen peroxide-based agents on the bond strength of brackets bonded with resin-modified glass ionomer cement has not been reported in the literature. No statistically significant difference was found when 35% hydrogen peroxide was assessed under all the conditions of the study, thus corroborating the results of Cacciafesta et al.11. However, there is controversy in the literature regarding studies demonstrating either increased bond strength18,19 or unchanged bond strength20. When the effect of time is taken into account, one can note a slight increase in the bond strength in the present study, although no statistically significant difference was found. In addition, no difference was found between the groups using 6% hydrogen peroxide, i.e., for at-home use. However, lower strength values were found in comparison to the control group. Despite the lack of statistical differences the greater the time interval between the whitening and bonding procedures, the greater the bond strength11,14. In those situations in which 7.5% hydrogen peroxide was used, the bond strength values were found to be significantly lower in comparison to the control group, regardless of whether the bonding procedure was performed immediately or after the 7-14-day period of whitening process. Despite the differences between these groups and the control group, no statistical difference was found between them and the other groups submitted to different concentrations of hydrogen peroxide. Reynolds21 suggested that a minimum bond strength of 6 to 8 MPa is adequate for most clinical orthodontic needs. These bond strengths are considered able to withstand masticatory and orthodontic forces. In this experiment, all bond strength values were above this minimum requirement. Some authors suggested that residual bleaching agents affected the bonding process and were responsible for decreased bond strengths15,19. They recommended pumicing before bonding to reduce any residual hydrogen peroxide. They also suggested that bleaching should be ceased 1 week before orthodontic bonding to ensure adequate bond strengths19,22,23. Based on such findings, one can conclude that the time elapsed between the whitening and bonding procedures is not relevant since the increase in the bond strength was not found to be statistically significant. Permanent bovine teeth were used in this investigation. When stored, handled, and prepared in a prescribed manner, they yield bond strengths that are comparable to those obtained with human teeth24. The ARI scores indicated no significant differences among the various groups; all groups had higher prevalence of ARI scores of 2 and 3. This means that failure occurred at the bracket-adhesive interface, as reported in previous studies11,25. In the literature, only 3 similar investigations evaluated the ARI scores11,16,19. These results are of great interest as the enamel is thought to be better protected when the bonding material remains adhered to it following bracket removal. Therefore, it could be concluded that the shear bond strength of the Fuji Ortho LC material decreases in teeth whitened with hydrogen peroxide at different concentrations, although statistical difference was found only in the group using 7.5% hydrogen peroxide. Furthermore, in all groups the majority of fractures occurred at the bracket/adhesive interface, with ARI scores ranging from 2 to 3. References
© Copyright 2008 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os08003t1.jpg] [os08003t2.jpg] [os08003f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}