 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal Oral Sciences, Vol. 7, No. 24, Jan/Mar 2008, pp. 1497-1501 Does masticatory muscle hyperactivity occur in individuals presenting temporomandibular disorders? Delaine Rodrigues-Bigaton1 Rosemary Berto2 Anamaria Siriani de Oliveira3 Fausto Bérzin4 1Professor, Postgraduate Program in Physical Therapy, Health Science School, Methodist University of Piracicaba, Piracicaba SP, Brazil Received for publication: December 7, 2007 Accepted: March 25, 2008 Code Number: os08006 Abstract Aim: To verify whether patients with temporomandibular disorders (TMD) present masticatory muscle hyperactivity with the mandible in the rest position. Key Words: temporomandibular joint dysfunction syndrome, electromyography, masticatory muscles Introduction Temporomandibular disorder (TMD) is characterized by functional and pathological alterations that affect the temporomandibular joint (TMJ), masticatory muscles and, eventually, other parts of the stomatognathic system1. The clinical signs and symptoms of TMD are varied, such as sounds and/or TMJ pain, headaches, difficulty on chewing, muscular pain, muscular and/or TMJ sensitivity and limitation or disturbances in mandibular movement, which involve the masticatory muscles, TMJ or both simultaneously1-3. No consensus exists among researchers regarding the etiology, diagnosis and treatment of TMD due to the lack of standardization of assessment and diagnostic procedures4. In this context, kinesiological electromyography (EMG) has been widely used to aid in the diagnosis of TMD because EMG results allows assessing the quality of muscular contraction5, muscular behavior at rest6-7 and the presence of muscular hypoactivity or hyperactivity8. Some authors5,7,9-11 have reported that TMD individuals show increased EMG activity of the masticatory muscles with the mandible in the rest position, referring to this situation as muscular hyperactivity in a rest position. However, Lund12, Stohler et al.13 and Zarb et al.14 questioned the term masticatory muscle hyperactivity with the mandible in the rest position. According to Zarb et al.14, what the literature calls muscular hyperactivity in the rest position are actually RMS (root mean square) values of around 1 to 2% maximum voluntary contraction recorded in EMG analyses. These authors believe that it is an exaggeration to consider this small increase in myoelectric activity as muscular hyperactivity. Furthermore, Finsterer15 affirmed that the pattern of interference of the EMG signal must be considered in order to analyze myoelectric activity. According to this author, this interference pattern can be defined as the sum of the motor unit action potential (MUAP) that starts being registered at 10% of maximum voluntary contraction (MVC) in some muscle locations and is present in all muscle locations at 30% of the MVC. Therefore, EMG activity recorded below 10% of the MVC should not be considered an EMG signal interference pattern, whether the values are obtained in contraction or at rest. In view of this, the aim of this study was to investigate whether individuals with TMD also present masticatory muscle hyperactivity with the mandible in the rest position. For such purpose, the experiment sought to determine whether the activity recorded with the mandible at rest would be above or below 10% of maximal dental clenching, given that EMG activity above 10% of the MVC is required in order to be considered as an EMG signal interference pattern. Materials and Methods By means of surface EMG, the masseter muscle and anterior portion of the temporal muscle were analyzed bilaterally in 46 female volunteers. Fifteen subjects aged 18 to 32 years (mean age = 22.7 ± 3.52 years) were considered as clinically normal (control group) and 31 subjects aged 19 to 33 years (mean age = 22.7 ± 3.38 years) presented TMD (experimental group). The experimental group included individuals who referred pain in the masticatory muscles during functional activities (speaking and eating), occlusal parafunction for a minimum period of 1 year and maximum of 5 years, and pain and/or muscular tiredness on waking and joint clicking for a minimum period of 1 year. For the control group, the inclusion criteria were absence of occlusal parafunction, joint and/or muscular pain during functional activities and tiredness and/or muscular pain on waking. Individuals with dental loss, history of facial traumas and TMD, joint luxation, limitation of TMJ movement amplitude, history of systemic diseases, such as arthritis, arthrosis, diabetes and neurological pathologies, were excluded from the trial. The study purposes, experimental procedures, duration, risks and benefits were fully explained to the volunteers. The research protocol was approved by and conducted in accordance with the guidelines of the local Human Research Ethics Committee (Protocol No. 120/2001). EMG Signal Recording The EMG signal was captured in an electrostatic Faraday cage at the Electromyography Laboratory of the Dental School of Piracicaba, State University of Campinas, Brazil. It was used a 16-channel signal conditioning module (MCS-V2 model; Lynx Eletronics Ltda., São Paulo, SP, Brazil) with analogical/digital converter resolution of 12 bits (CAD 12/46 model, Lynx Eletronics Ltda), sampling frequency of 2,000 Hz and cutting frequency of 10.6 Hz in the high-pass filter and 509 Hz in the low-pass filter, performed by an analogical two-pole Butterworth-type filter. Aqdados software (Lynx Eletronics Ltda) version 4.18 was used for digitized signal acquisition and storage in data files. Simple differential surface electrodes (Lynx Eletronics Ltda.) were used, consisting of two parallel rectangular bars of pure silver (Ag) (10 x 2 mm) spaced at 10 mm and fixed in an acrylic resin capsule (23 x 21 x 5 mm), with input impedance of 10 GW, CMRR of 130 dB and 2 Faraday peaks, 100 times gain, with high-pass of 20 Hz and low-pass of 500 Hz and 1.5 m connecting cables. In addition, a rectangular stainless steel reference electrode (33 x 31 mm) was placed on the right wrist of all volunteers in order to reduce noise during EMG signal acquisition, The electrodes were placed on the thickest portion of the masseter muscle and the anterior portion of the temporal muscle, bilaterally, remaining parallel to muscle fiber direction, with the silver bars perpendicular to the fibers in order to maximize capture and minimize noise interference. The electrodes were placed on the skin, previously cleaned with a 70% alcohol solution, and fixed with adhesives. EMG signal was collected with the volunteers seated on a chair, with their backs completely supported by the back of the chair, Frankfurt plane parallel to the ground, eyes open, feet supported on the ground, and arms supported on the lower limbs. EMG signal was captured in two mandibular positions: 1) Mandible in the rest position, signal colleted for 5 seconds, 3 times, and 2) Maximal dental clenching, collected for 5 seconds, 5 times, with Parafilm “M®” (Chicago, IL, USA) material located between the premolars, maxillary and mandibular 1st and 2nd molars, with a 2-minute interval between signal captures, aimed at minimizing the effects of muscular fatigue. Data Analysis Mann Whitney U-test (α = 0.05) was used for comparative analysis of the mean RMS values of the masseter muscle and anterior portion of the temporal muscle, bilaterally, between the control and experimental groups, in the rest position and maximal dental clenching. In order to verify the interference pattern of the EMG signal at rest, the percentage of EMG activity in the rest position of the muscles studied in both groups was analyzed. The percentage of EMG activity was determined using the following equation: 
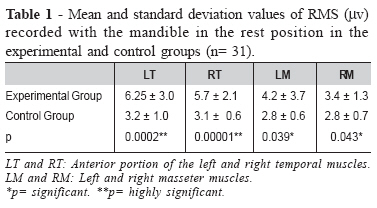
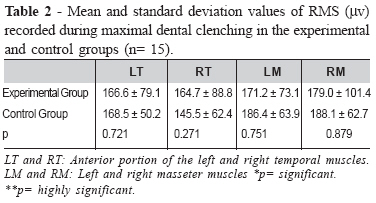
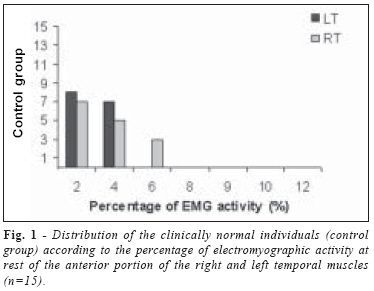
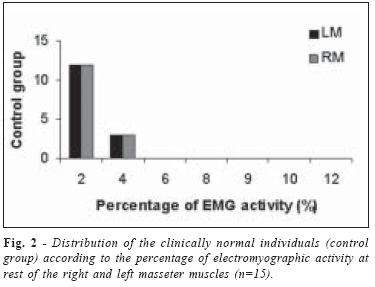
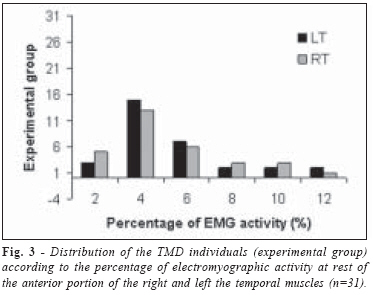
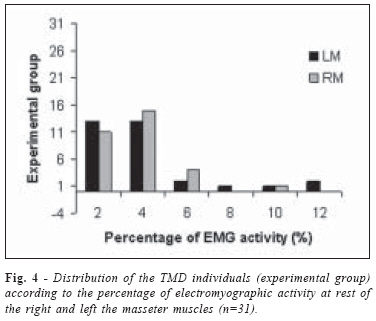
RMS clenching Where: Percentage (%) = percentage of EMG activity at rest; RMS rest = RMS values obtained with the mandible in the rest position; RMS clenching = RMS values obtained from maximal dental clenching. The purpose of this analysis was to demonstrate whether the rest activity of the mandibular elevator muscles was above or below 10% of maximal dental clenching. After the percentages were obtained, frequency distribution was performed, in which blocks 2, 4, 6, 8, 9, 10 and 12 were randomly defined. The values in percentages (%) were compared between the control and experimental groups by the Mann Whitney U-test. Results Table 1 presents the mean RMS values (µV) of the masticatory muscles in the rest position in both groups. The experimental group presented significantly higher RMS values at rest than the control group (p<0.05). Table 2 presents the mean RMS values of the masticatory muscles in maximal dental clenching in both groups. There was no significant difference between the groups (p>0.05). Figures 1, 2, 3, 4 show the values in percentage (%) of EMG activity in the rest position of the anterior portion of the temporal muscle and masseter muscle, bilaterally, in both groups. Figures 1 and 2 present the values of the control group. In this group, the values in percentages (%) ranged from 1 to 6% of maximal dental clenching. The only muscle that presented 6% of maximal dental clenching was the right temporal muscle. The values of the experimental group are presented in Figures 3 and 4. In this group, the values in percentage (%) ranged from 1 to 12% of maximal dental clenching. Discussion The results of the present study showed that in the rest position, individuals with TMD presented higher electrical activity of the mandibular elevator muscles than the control group, which was also observed in the anterior portion of the temporal muscle, bilaterally. In maximal dental clenching, no significant differences were observed between the groups. However, a statistically significant difference was observed between the experimental and the control groups regarding EMG activity at rest, which corroborates the findings of Bodéré et al.11 and Rodrigues et al.10 Considering the affirmation of Zarb et al.14 and Finsterer15 and the results obtained in the present study, we believe that the terminology muscular hyperactivity in the rest situation is unsuitable. As hereby demonstrated, few individuals presented EMG activity at rest between 9 and 12% of maximal dental clenching. Thus, in view of the present results and in agreement with Rodrigues et al.10, the increased EMG activity of the mandibular elevator muscles in the rest situation must be considered as a sign of TMD or a consequence of possible etiologic factors of TMD16-20, such as, postural alterations, malocclusion, emotional stress, among others, and not as a causal factor of the pathology. Although further studies are required to determine its causes, it is likely that the increased electromyographic amplitude of the mandibular elevator muscles at rest is due to sensorimotor interactions, in which pain, a symptom present in most TMD evaluated patients, may modify the generation of the action potential and, ultimately, the amplitude of the EMG signal. In the control group, EMG activity was observed with the mandible in the rest position in all evaluated muscles. These finding corroborate those of Widmalm et al.21, who reported that even in a sample of individuals without clinical symptoms, some muscles may present EMG activity with the mandible in the rest position. According to Graven-Nielsen et al.22,23, the amplitude of the EMG signal and force are diminished during maximal dental clenching in the presence of pain. This has also been observed in fibromyalgia24,25 and in TMD26. However, in the present study, in the same way as described by Rodrigues et al.10, no significant differences were observed between the EMG activity of individuals with TMD and those that were clinically normal. In view of the above-discussed issues, evidence as to whether or not EMG activity is reduced during maximal dental clenching in the presence of pain is still arguable and needs further investigation. Under the tested experimental conditions, it may be concluded that an increase in the electromyographic activity occurred at rest of around 1 to 12% of maximal dental clenching, particularly in the anterior portion of the temporal muscle. However, care should be exercised before naming this increase as muscular hyperactivity in this situation. The increase in myoelectric activity must rather be considered as an important sign of TMD and, therefore, accounted in the therapeutic proposal. References
© Copyright 2008 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os08006t1.jpg] [os08006f4.jpg] [os08006t2.jpg] [os08006f1.jpg] [os08006f3.jpg] [os08006f2.jpg] [os08006e1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}