 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
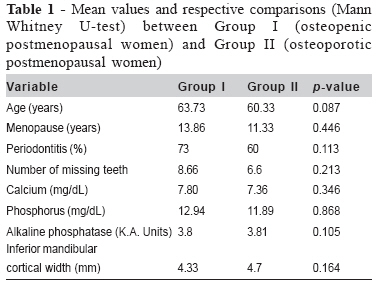
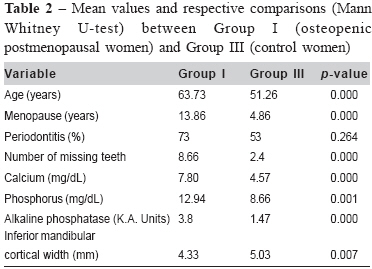
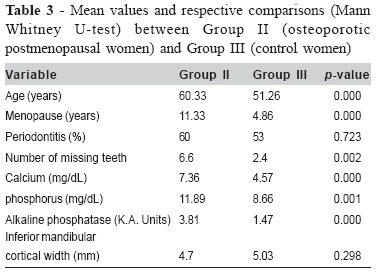
Brazilian Journal Oral Sciences, Vol. 7, No. 24, Jan/Mar 2008, pp. 1502-1506 Oral signs and salivary parameters as indicators of possible osteoporosis and osteopenia in postmenopausal women -A study of 45 subjects Siva Reddy1 Ramalingam Karthikeyan2 Herald Justin Sherlin2 Natesan Anuja2 Ramani Pratibha3 Premkumar Priya3 Thiruvengadam Chandrasekar4 1Postgraduate Student 2Senior Lecturer 3Assistant Professor 4Professor and Head, Department of Oral Pathology, College of Dental Surgery, Saveetha University, Chennai, Tamil Nadu, India Received for publication August 08, 2007 Accepted - April 07, 2008 Code Number: os08007 Abstract Aim: To correlate the oral signs, salivary calcium, phosphorus, alkaline phosphatase levels and dental radiographic findings in postmenopausal osteoporotic, osteopenic and non-osteoporotic women. Key words: osteoporosis, osteopenia, salivary alkaline phosphatase Introduction Osteoporosis is a chronic systemic skeletal disease characterized by low bone mass and micro-architectural deterioration, resulting in increased bone fragility and susceptibility to fracture. The World Health Organization (WHO) has defined osteoporosis and osteopenia based on normal bone mineral density (BMD). In the United States, osteoporosis affects more than 25 million people and predisposes patients to more than 1.3 million fractures annually1. Women are at greater risk for osteoporosis after menopause. Premenopausal estrogen levels are protective, as is hormone replacement therapy2-4. Early menopause, either naturally occurring, drug or surgically induced without hormone replacement therapy predisposes to osteoporosis5. Data suggest that panoramic radiograph findings, such as progressive periodontal disease, alveolar bone resorption, tooth loss and endosteal resorption of the mandibular inferior cortex, may indicate general osteoporosis. If low BMD can be related to certain oral signs, the possibility of latent osteoporosis might prompt dentists to refer these patients for medical evaluation6. Chemicals in serum and urine can serve as markers for monitoring bone loss, new bone formation and the effectiveness of therapy in patients with osteoporosis. A large number of markers have been discovered for both bone formation and bone resorption7-9. Over the years, several studies have been performed in order to establish methods for diagnosis or prognosis of oral disease with saliva. The value of saliva as an indicator of systemic disease has also been explored10. The aim of the study was to estimate the salivary calcium, phosphorus and alkaline phosphatase levels and correlate the salivary findings, radiographic changes and periodontal status in osteopenic osteoporotic and healthy postmenopausal women. Materials and Methods The study comprised postmenopausal women aged 45 to75 years recruited from the Outpatient Department of Orthopedics at Saveetha Medical Hospital, Chennai, Tamil Nadu, India. After being clinically examined by an orthopedic surgeon, the patients were assessed for BMD using an ultrasound densitometer (Furuno CM-100 Nishinomiya, Japan). According to the WHO, spine BMD is categorized as follows: Normal: T score is above -1.0; Osteopenic: T score is between -1.0 to -2.5 and Osteoporotic: T score is below -2.5. Based on these criteria and according to the BMD results, 45 subjects were selected and assigned to three groups. Group I (study group) comprised of 15 established osteopenic postmenopausal women, aged 45 to75 years, without any other preexisting systemic diseases, such as primary or secondary hyperparathyroidism, osteomalacia, rheumatoid arthritis and multiple myeloma; Group II (study group) comprised of 15 established osteoporotic postmenopausal women, aged 45 to 70 years, without any of the aforementioned systemic diseases; and Group III (control group) comprised of 15 postmenopausal women, aged 45 to 70 years, without osteopenia or osteoporosis or any of the aforementioned systemic diseases. The study and control groups were analyzed for the following parameters: measurement of mandibular cortical width, Russel’s periodontal index and salivary parameters, like calcium, phosphorus and alkaline phosphatase levels. Panoramic radiographs were obtained by using Kodak Tmat G/RA, 5x12 inch panoramic dental film. The mandibular cortical width was measured at the site of mental foramen on the radiographs, in accordance to Taguchi et al.11-12. Standard UCLA procedure was used for saliva collection13. Approximately 5 mL of saliva were collected from each subject and centrifuged at 2,500 rpm for 5 minutes. The centrifugation resulted in a saliva sample free of large particle debris and reduced viscosity, thereby allowing a more accurate and reproducible analysis. All samples were subjected to biochemical evaluation. Calcium was estimated by using a commercially available kit, based on the Ocresolphthalein complexone method (Crest bio-systems, Goa, India). Phosphorus was estimated by using a commercially available phosphorus kit, which functions on the basis of Gomori’s method. (Crest bio-systems, India). Alkaline phosphatase was estimated by using a commercially available alkaline phosphatase kit, which functions on the basis of Modified Kind & King’s method (Crest bio-systems, India). Statistical Analysis Means and standard deviations of age, menopause, periodontitis, number of missing teeth, salivary levels of calcium, phosphorus and alkaline phosphatase, and inferior mandibular cortical width were calculated for all groups. Mann-Whitney U test was used for comparisons between groups (α=0.05). Results Tables 1, 2 and 3 present the comparisons between Group I and Group II, Group I and Group III and Group II and Group III, respectively. The parameters of age, postmenopausal time, number of missing teeth, salivary levels of calcium, phosphorus and alkaline phosphatase, and inferior mandibular cortical width were statistically significant comparing the study groups to the control group. Periodontitis was not statistically significant in all comparisons. Regarding age, the osteoporotic, osteopenic and control groups had mean ages of 63.73, 60.33 and 51.26 years, respectively. There was a significant increase of age in osteoporotic and osteopenic group compared to the control women. The osteoporotic, osteopenic and control groups showed a postmenopausal mean duration of 13.86, 11.33 and 4.86 years, respectively. Salivary parameters, such as calcium, phosphorus, alkaline phosphatase levels and oral signs like the periodontal status, number of missing teeth and inferior mandibular cortical width were assessed. The normal/standard values mentioned as per literature were 5.2 mg/dL (1.35 mMol/L) and 17.18 mg/dL (5.5 mMol/L) for salivary calcium and phosphorus, respectively. No standard values were available for alkaline phosphatase levels in saliva. The mean number of missing teeth for the osteoporotic, osteopenic and control groups was 8.66, 6.6 and 2.4, respectively. The mean inferior mandibular cortical width in osteoporotic, osteopenic and control women was of 4.33 mm, 4.7 mm and 5.03 mm, respectively. Salivary calcium levels in the osteoporotic, osteopenic and control groups showed mean values of 7.80 mg/dL, 7.36 mg/dL and 4.57 mg/dL. There was a significant increase in calcium levels of the osteoporotic and osteopenic patients when compared to the healthy controls. Salivary phosphorus levels in osteoporotic, osteopenic and control groups showed mean values of 12.94 mg/dL, 11.33 mg/dL and 8.66 mg/dL, respectively. Alkaline phosphatase levels in the osteoporotic, osteopenic and control groups showed mean levels of 3.8, 3.81 and 1.47 K.A.Units, respectively. There was a significant increase in alkaline phosphatase levels in patients with osteoporosis and osteopenia when compared to the controls. Discussion Osteoporosis and osteopenia are chronic systemic skeletal diseases characterized by low bone mass and microarchitectural deterioration with a consequent increase in the bone fragility and susceptibility to fracture. According to the WHO, osteoporosis is present when BMD is 2.5 standard deviations (SD) below the normal value seen in young patients. Osteopenia is defined as bone density levels are between 1 SD and 2.5 SD below normal BMD. Density of the jaw bones differs according to the region, ranging from D1 to D4 where. D1 represents high-density regions like the anterior mandible and D4 represents lowdensity regions like the posterior maxilla. In procedures such as implant placement and prosthodontics, density of the jaw bones plays a major role in determining the outcome. There is evidence that osteoporosis and osteopenia have a direct effect on jaw bones, resulting in resorption and reduction in density. The osseointegration between bone and implants could also be compromised in such cases. Studies have shown that the generalized osteoporosis has a significant effect on the periodontal health status, thus compromising tooth support14. An early diagnosis and intervention strategy may lead to better treatment outcomes. Several oral signs, namely alveolar bone resorption15-21, periodontal condition14,20,22, number of missing teeth 20,23-26, mandibular BMD measured on oral radiographs14,16-19,27-32, thickness of mandible on panoramic radiographs6,11-12,20 and inferior cortex morphology30, have been evaluated in order to distinguish between normal and osteoporotic population. Over 50 years ago, Fuller Albright33 noted that postmenopausal women lost excessive amounts of calcium in their urine and thus introduced biochemical markers into the clinical arena. Subsequently, a number of markers have been discovered for both bone formation and bone resorption. Alkaline phosphatase and osteocalcin serve as markers for bone formation. Urinary calcium and type I collagen-related peptides serve as markers for bone resorption7-9. Common biochemical markers for osteoporosis include calcium, phosphorus, type I collagen-related peptides, alkaline phosphatase and osteocalcin, which are routinely assessed in the blood. Innumerable studies have tried to establish methods for diagnosis or prognosis of oral disease using salivary analysis. The value of saliva as an indicator of systemic diseases, such as autoimmune disorders, cardiovascular, endocrine, renal and infectious diseases and cancer, has also been explored10. Calcium and phosphorus are present as inorganic components of saliva, which quantitatively accounts as the main mineral component of the human skeletal system. Some of the alkaline phosphatase is also secreted into the saliva and may thus serve as a biochemical marker for bone turnover. The currently available techniques for in vivo bone mass measurement techniques are expensive and may not be effective to screen the general population. Hence, saliva, which is an ultra-filtrate of plasma, could be used as a simple, efficient, non-invasive and cost-effective diagnostic resource. Many studies have attempted to show a causal relationship between osteoporosis, osteopenia and periodontal disease. In the present investigation, 73% of the osteoporotic group and 60% of the osteopenic group were affected by periodontitis. In a case-control study, Von Wowern et al.14 found significantly greater periodontal attachment loss in osteoporotic women than in normal women. Elders et al.22 observed no significant correlation between periodontitis and spinal BMD. Likewise, Kribbs20 did not find significant difference between the osteoporotic and non-osteoporotic groups in mean probing depth of pockets or recession from the cementoenamel plus probing depth, which is a measurement of periodontal attachment loss. Studies have shown that age and menopause17,34-36 are the two main risk factors for osteoporosis and osteopenia in women. The results of the present study are supportive to these findings. In the present study, there was a significant increase in the number of missing teeth in the study groups compared to the control group, which suggests that tooth loss might be related to osteoporosis and osteopenia in postmenopausal women. Several authors20,23-26 have reported that tooth loss is related osteoporosis and osteopenia. The relationship between the cause of tooth loss and the general mineral status is not known. Tooth loss is caused by multiple factors, such as caries, periapical and periodontal disease and tooth fracture. Ward and Mason37 suggested that although osteoporosis may have no effect on the periodontal status, it may influence the rate of bone loss in chronic periodontitis. The findings of the present study are consistent with the current literature, which suggests that the number of missing teeth is higher in patients affected by osteoporosis and osteopenia. There was significant decrease of mandibular cortical width in osteoporotic women when compared to the control group. Taguchi et al.11,12 have shown that the mandibular cortical width was correlated to the mandibular cortical BMD, which rapidly decreases after the 5th decade of life in women. Kribbs et al.20 reported that osteoporotic women could not be distinguished from normal women on the basis of thickness of the cortex at the angle of the mandible. The mandibular bone is thicker than other bones in the body, like spine, hip and femur, which means that the mandible is significantly affected only by severe bone resorptive conditions, such as osteoporosis, when compared to less severe conditions, like osteopenia, as reflected in the present study. There was a significant increase in phosphorus levels in osteoporotic and osteopenic women compared to the healthy controls. Sewon et al.38 reported that there was significantly increased salivary calcium in the women with low BMD and no significant difference in phosphate levels. However, our study showed significantly increased levels of calcium and phosphorus between osteoporotic and osteopenic groups. Sewon et al.39 observed that hormone replacement therapy in postmenopausal women significantly decreases the salivary calcium levels. Estrogen deficiency in postmenopausal women is accompanied by increased bone resorption. This could be attributed to the loss of direct effects on osteoclasts and their precursors, but indirect actions on the immune system may also be involved. The productions of cytokines like IL-1, TNFá and IL-6 can potentially enhance bone resorption and can be suppressed by physiological doses of estrogen40. Studies have proven that an increased level of calcium in the urine is a marker for the resorption of bone7-9. Bone resorption releases calcium into the serum, which is filtered into the urine and excreted. The present study also showed an increased level of calcium in saliva, which is an ultra filtrate of plasma. To the best of knowledge, this is the first study to measure the salivary alkaline phosphatase levels in postmenopausal osteoporotic, osteopenic and non-osteoporotic/osteopenic women. Our data showed a significant increase in alkaline phosphatase levels in the osteoporotic and osteopenic patients when compared to the controls. Since there is no standard level published in the literature for salivary alkaline phosphatase, the values were compared to those of the control group. Alkaline phosphatase is a marker for bone turnover. Ross et al.9 and Taguchi et al.41 reported that the levels of serum total alkaline phosphatase and bone-specific alkaline phosphatase are increased in subjects with low BMD. Likewise, the present study showed significantly higher levels of salivary alkaline phosphatase in osteoporotic and osteopenic subjects than in the controls. However, before salivary parameters and oral signs can be used as predictors for these systemic diseases, further investigations are needed to support any definite conclusions. The results of the present study demonstrate that assessment of salivary parameters, such as calcium, phosphorus and alkaline phosphatase, along with some oral signs like periodontitis and number of missing teeth may be important indicators to aid in the diagnosis of osteoporosis and osteopenia in postmenopausal women. References
© Copyright 2008 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os08007t3.jpg] [os08007t2.jpg] [os08007t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}