 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
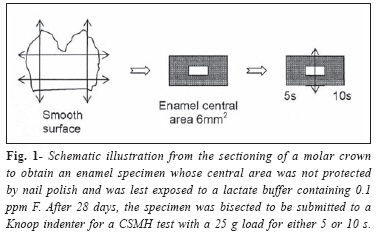
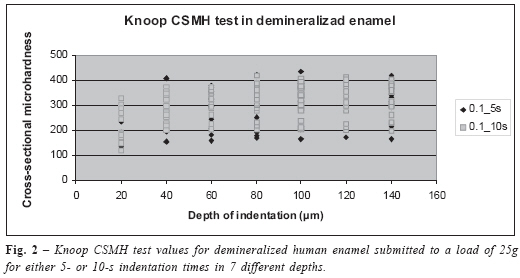
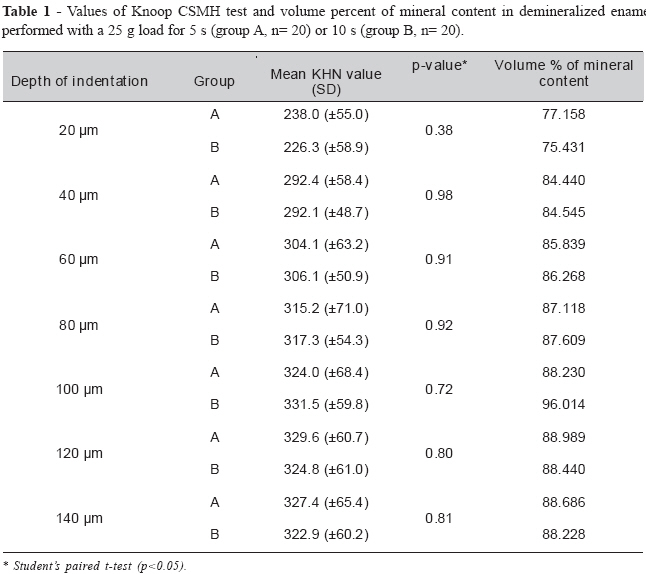
Brazilian Journal Oral Sciences, Vol. 7, No. 24, Jan/Mar 2008, pp. 1507-1511 Effect of time in hardness test on artificially demineralized human dental enamel Mirian de Waele Souchois de Marsillac, DDS, MSc, PhD1 Alberto Carlos Botazzo Delbem, DDS, MSc, PhD2 Ricardo de Sousa Vieira, DDS, MSc, PhD3 1Professor, Department of Community and Preventive Dentistry, State University of Rio de Janeiro, Brazil 2Professor, Department of Dentistry, Dental School of Araçatuba, State University of São Paulo, Brazil 3Professor, Department of Pediatric Dentistry, Dental School, Federal University of Santa Catarina, Brazil Correspondence to: Mirian de Waele Souchois de Marsillac Boulevard 28 de Setembro, 157 / sala 226, Vila Izabel, Rio de Janeiro – RJ. CEP 20.551-030 Telephone: +55 21 2587-6372 e-mail: mwsm63@terra.com.br Received for publication: June 06, 2007 Accepted: April 15, 2008 Code Number: os08008 Abstract A cross-sectional microhardness (CSMH) test was carried out in human dental enamel exposed to a demineralizing solution in order to evaluatetwo different times of indentation in sound tissue and artificially induced caries. Twenty caries-free extracted human molars had one of their smooth surfaces sectioned and the enamel surface was isolated with nail polish except for an area of 6 mm2 . These specimens were submitted to artificially induced enamel caries on a lactate buffer containing 0.1 ppm fluoride (F) during 28 days. All specimens were bisected to create groups A and B in which CSMH test was performed employing a Knoop indenter with a 25 g load for 5 or 10 s, respectively. Student’s paired t-test (p<0.05) was used to determine statistically significant differences between groups A and B in 7 depths. There were no significant differences between any of the analyzed depths. Since the present experiment showed no significant difference when comparing indentations made with a 25 g load during either 5 or 10 s in different depths, this method can be used with either one of the time intervals tested without compromising a CSMH test on artificially demineralized human enamel. Key words: dental enamel, tooth demineralization, hardness tests. Introduction A variety of hardness testing instruments have been used in the past to determine the hardness of mineralized dental tissues1. The Knoop indentation hardness instrument was developed by Knoop et al.2 to accurately measure hardness of various materials including dental materials and mineralized tooth structure. This instrument has an elongated diamond pyramid-shaped point (indentor) that is pressed onto the test material under a well defined load for a given time. The size of the resulting indentation is determined with the aid of a microscope. The indentor causes a surface area deformation at the mineralized tissue under analysis. Hardness values are a measure of the mechanical resilience of the enamel, dentin or cementum due to the penetration of an indenter. A combination of both inorganic and organic material on tooth structure renders a hardness value for its mineralized tissues. The indenter on the hardness testing instrument can be used either upon the prism ends at the enamel surface (surface microhardness - SMH) or perpendicular to the prism (crosssectional microhardness - CSMH). Knoop hardness number (KHN) is calculated based on the relationship of an applied force in grams (K) and the indentation length of the long diagonal in micrometers (L), using the equation3-4: KHN (kg/ mm2) = 14230 K / L2. When performing a SMH test on demineralized and remineralized human or bovine enamel, Feagin et al.5 found that a change of one Knoop hardness unit corresponded to about 0.04 moles of Ca++/cm2 in the respective surface. Therefore, the hardness values is closely related to the mineral content of normal and demineralized dental enamel in natural or artificial carious lesions. A correlation coefficient of 0.91 was found between the hardness test and the volume percent of mineral content. To determine the volume percent of mineral content, the following equation should be used: vol% mineral = 4.3(“KHN) + 11.3. Lesion depth (ìm) is defined by the distance from the outer surface to the position where the mineral content reaches 95% of the mineral volume from sound enamel6-8. Therefore, microhardness profiles can be used to measure hardness changes in enamel or dentin and the loss or gain of mineral content as in the processes of demineralization and remineralization3, 9. Whenever a force or load is inflicted to the tooth structure, it promotes tension and stress inside this tissue. Therefore, the alteration of the original dimensions in tooth structure results in an indentation of an elongated pyramid were the small and the large diagonal have a uniform proportion of 1:7 without neighboring deformation. In order to prevent alteration on indentation size or shape, the CSMH test has to be performed with a certain time interval so that the stress can be dispersed within dental structure. Thus, the time interval necessary to perform this test onto the mineralized tooth surface is very important to obtain the required accuracy and sometimes it can be time consuming. Studies have already been performed with a 25 g for 5 s in demineralized enamel10-12 Since the time interval is important to disperse the stress into the demineralized structure, the present study investigated the use of a Knoop indentor on a CSMH test in artificial demineralized human enamel applying a same load (25 g) during two different indentation times (5 or 10 s) in order determine whether significant differences exist between them. Material and Methods The research protocol was independently reviewed and approved by the Research Ethics Committee of the Federal University of Santa Catarina, Brazil. Twenty caries-free extracted human molars were selected, scaled to remove periodontal ligament remnants, cleaned with a mixture of deionized water and pumice in engine-driven rubber cups and thoroughly washed with deionized water. After ultrasonication (Ultrasonic Cleaner 1440D – Odontobrás, Ribeirão Preto, SP – Brasil) for 15 min in deionized water, all teeth were left to dry at room temperature on absorbent paper and a stereomicroscope at ´25(Olympus SZH10 - Olympus Optical do Brasil, Ltda., São Paulo, SP -Brazil) coupled to a digital imaging capturing system (Olympus DP12 - Olympus Optical do Brasil, Ltda., São Paulo, SP - Brazil) was used to discard specimens with enamel cracks, defects or discolorations. All teeth had their roots removed with a diamond wafering blade (Buehler - Lake Bluff, IL – USA) installed in an ISOMET 1000 cutting machine (Buehler - Lake Bluff, IL – USA) under cooling with deionized water. Each molar crown was sectioned in the same machine in such a way that one tooth originated a total of 4 fragments corresponding to the mesial, distal, buccal and lingual surfaces. Only one of the fragments was randomly allocated into demineralizing solution. A red nail polish was used to cover every aspect of the specimens, except for an area limited with a square shaped adhesive paper, sized 2 mm x 3 mm (6 mm2). This area was located in the middle of the smooth unbraided enamel surface. The adhesive paper was removed after the double-coated nail varnish had dried completely at room temperature. Iijima et al.7 used a clear nail varnish in their experiment and verified that the penetration into sound enamel surface was always less than 5 ìm. Specimens were individually immersed in 25 mL of a demineralizing solution without agitation at 37oC in plastic receptacles during 28 days. A lactate buffer was used to produce artificial caries lesions in all specimens and it was renewed every 14 days. Test solutions were prepared accordingly to White13 and contained: 0.1 mol/L lactate buffer/ 0.2% polyacrylic acid (Carbopol® 980 – DEG Importadora de Produtos Químicos Ltda., São Paulo, SP -Brazil)/ 50% saturated hydroxyapatite (Gen-phos HA -Hospitália Cirúrgica Catarinense Ltda., Florianópolis, SC Brazil)/ 0.1 ppm F (as sodium fluoride - NaF) at pH 5.0. Specimens were washed in deionized water for 30 s after demineralization8. After demineralization, each specimen was bisected at the center of the lesion, perpendicular to the tooth surface, using the diamond wafering blade of the ISOMET 1000 cutting machine. This procedure was performed under deionized water cooling and with a low rotating speed of 100 rpm. Thereafter, the nail polish was carefully peeled from each half after sectioning and specimens were embedded in polyester resin (Central do Fiber Glass Indústria e Comércio Ltda. Florianópolis, SC - Brazil). One half from a tooth was submitted to a 5-s indentation procedure (Group A) and the other half to a 10-s indentation procedure (Group B). The methodological steps followed to obtain the enamel specimens are illustrated in Figure 1. Before the CSMH test, all specimens were ground wet with 1200- and 1500-grit silicon-carbide sandpaper using deionized water as a coolant. Polishing was performed in 3 stages using Buehler polishing clothes and alumina waterbased suspensions (decreasing order of 1.0, 0.3 and 0.05 ìm). Both grinding and polishing were done with deionized water in a Politriz DP10 Struers machine (Panambra Industrial e Técnica SA, São Paulo, SP- Brazil) until a glass-like appearance was obtained. The specimens were washed and individually ultrasonicated for 15 min with deionized water after each grounding and polishing procedures. These laboratory steps were conducted according to Ferreira14. Measurement from the indentation in enamel had to be clearly outlined and flawless in order to be taken15. Three parallel rows of 7 indentations 100 ìm apart from each other were made. The first indentation was performed 20 ìm from the outer enamel surface up to a depth of 140 ìm and keeping a 20-ìm interval from each one, as described by Chedid and Cury11 and Paes Leme et al.16. The demineralized area was calculated to a point were the lesion depth had a value of 95% of the mineral content from the sound enamel underneath it6-8. Every indentation was carried out with a 25 g load based on Argenta et al.10 and using a Knoop cross-sectional hardness test (HMV Microhardness Tester - Shimatdzu Corporation, Tokyo – Japan). A computer-assisted measurement system for Windows (CAMSTM_WIN; Newage Testing Instruments Inc., Southampton, PA - USA) was used with this equipment. Comparison of two indentation times used in this experiment (5 or 10 s) on each evaluated depth was obtained by the Student’s t-test with a level of significance set up to p<0.05. Statistical analysis was performed using SPSS software (System for Windows, version 13, 2003). Results The results for all 7 depths of indentations of the Knoop CSMH test in demineralized enamel, performed with a 25 g load during either 5 s (group A) or 10 s (group B) are displayed on Figure 2. An artificial white spot lesion (WSL) was produced in this study when using a demineralizing solution prepared according to one of the acid lactic buffered solutions tested by White13. Lesion formation could be observed within a 2040 ìm depth according to the Knoop CSMH test values transformed into volume percent mineral content3 (Table 1). WSL could be detected by the naked eye after brief air drying of specimen surfaces. Results for the Student’s paired t-test (Table 1) show no statistically significant difference between groups A and B in any of the 7 evaluated depths. Discussion CSMH test is widely used in the dental literature to study demineralization and/or remineralization in human teeth3-4,1011,15,17 or in bovine teeth10,12,16,18. The operator error for hardness measurements was found to be less than 5% when reading either steel or enamel indentations. For this reason, the accuracy and reproducibility of this test indicates that its applicability is very reliable for sound or demineralized hard dental tissues4. A 25-g load was maintained in every indentation row from the most outer enamel layer (20 ìm) to the deepest one (140 ìm), as reported by Argenta et al.10 when evaluating SMH and cross-sectional CSMH of topical-fluoride treated and pH-cycled human dental enamel. The same load of 25 g with a 5-s time interval was also used in similar studies11-12. Initially, Craig and Peyton15 tested 25 to 200 g loads for 15 s on sound human enamel and dentin and concluded that a 50 g load could bring optimal results with well defined indentations and a minimum of fractures around the edges. CSMH test has also been carried out with a 50 g load for 10 s on sound or demineralized human and bovine enamel19-20. Usually smaller loads are used on superficial rows at the outer enamel portion to avoid cracks3,4,17,21. This technique implies that every time that the researcher changes the load, it is necessary to modify all parameters on the machine. Since laboratory work can be time-consuming, the authors chose evaluating a CSMH test on human artificially demineralized dental enamel using a 25 g load for either 5 or 10 s. In the present study the first row of three indentations was performed at a 20 ìm distance from the outer enamel surface based on Chedid and Cury11, Paes Leme et al.16, and Delbem and Cury18. The reason for this standardization occurred due to the cracking of the enamel outer surface when the indentation was done at a 10 or 15 ìm depth. Other workers34,10,12,17 do not mention cracks on specimens when carrying on a 7-15 ìm indentation from the outer enamel surface. According to previous studies10-11,16,18 an interval between the indentation on each row was kept at a 20 ìm distance. Some studies make larger intervals of 25 ìm3,9 or even smaller as 10 ìm4. A 20 ìm interval, in depth, between indentations was accomplished in order to avoid possible superpositioning of indentations as when working with a 10 ìm interval. A larger interval could compromise the observation of small hardness changes in different enamel depths. A variation in hardness Knoop measurements was observed on artificial carious lesion from different smooth surfaces among the 20 teeth used on this experiment. The reason why the artificial caries lesions were cut in half was that a same surface from a tooth could be investigated when submitted to either a 5-or a 10-s indentation under the same load (25 g). The degree of variation was found to be within acceptable limits as demonstrated by the standard deviation for group A (+55) and group B (+58.9) (Table 1). No hardness values obtained in this study was discarded as having a large deviation from the average. Fifteen percent of the hardness values from both sound enamel and dentin were out of the range of experimental error and were thus not considered in Craig and Peyton’s study15. Variations in hardness can be kept within acceptable limits when control and test groups are from the same teeth17. These findings are in accordance with those of other studies performed in sound and/or demineralized human enamel4,15,17,20. According to Purdell-Lewis et al.17, the hardness values from SMH in artificially demineralized human enamel were the same in different areas of a same tooth and very similar between different teeth. They also found that the drop in hardness values after demineralization was related to the original hardness of the sound enamel. Caldwell et al.22 stated that the observed variations in hardness values were not marked and could occur on a same surface, teeth from different individuals with different ages (primary, permanent and erupted or not), various surfaces from the same tooth, among different tooth types from the same person or from different individuals. When working with bovine enamel, the researcher has to have in mind that progression of artificial caries lesion is faster than in human enamel. The spreading in bovine enamel is smaller than in human enamel and so standard deviation in bovine enamel is always found to be smaller20. In the present study, Student’s paired t-test was not able to find significant difference when comparing indentations made with a 25 g load for 5 (group A) or 10 s (group B) in any of the evaluated depths. Based on these findings, it may be concluded that an operator can use a Knoop CSMH test with a 25 g load on artificial carious lesions produced in permanent human enamel for either 5 or 10 s using the described methodology. Acknowledgments The authors would like to thank Dr. Carla Moreira Pitoni (PhD) for handling statistical data. References
© Copyright 2008 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os08008t1.jpg] [os08008f2.jpg] [os08008f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}