 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
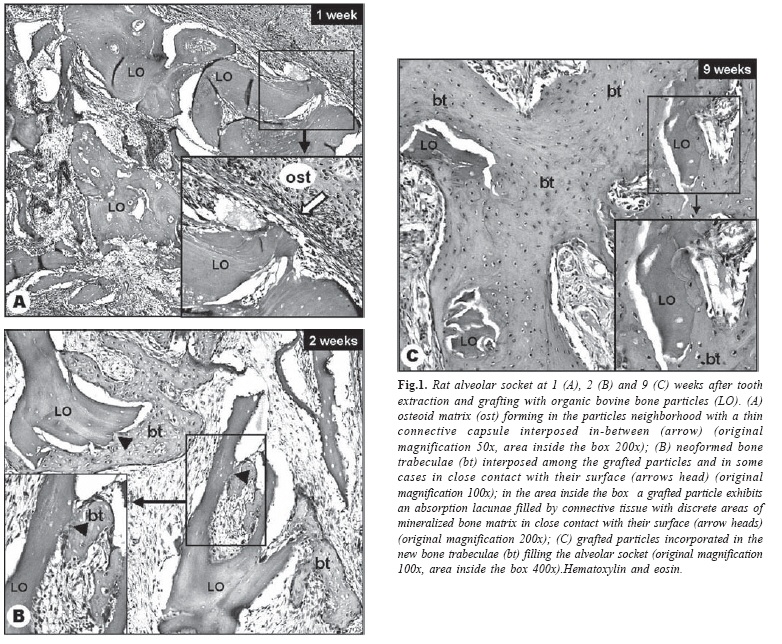
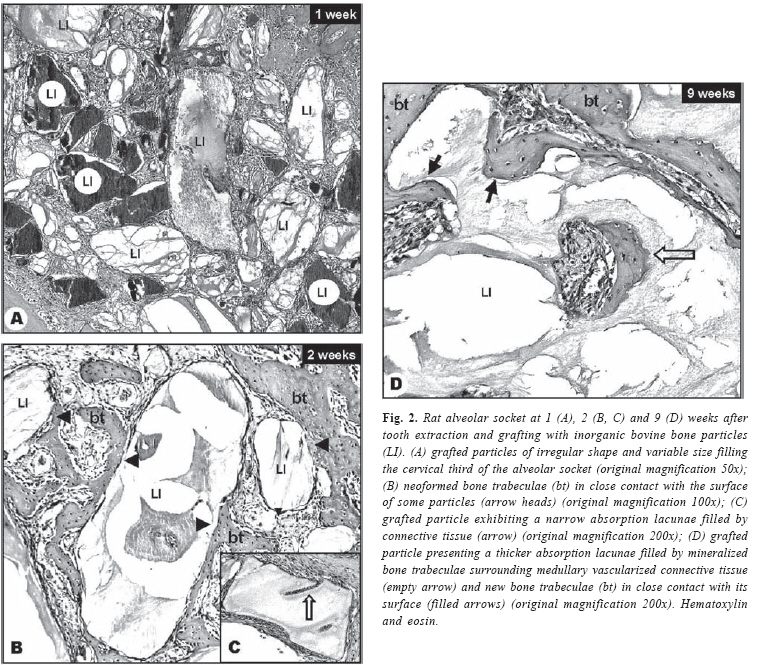
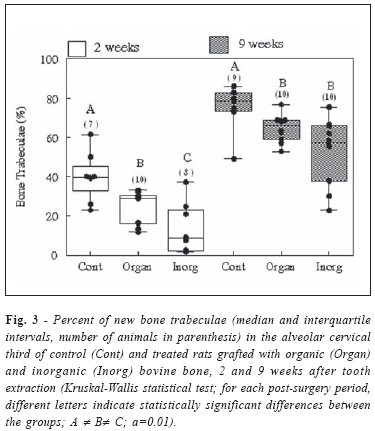
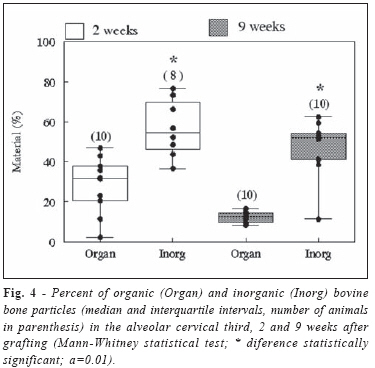
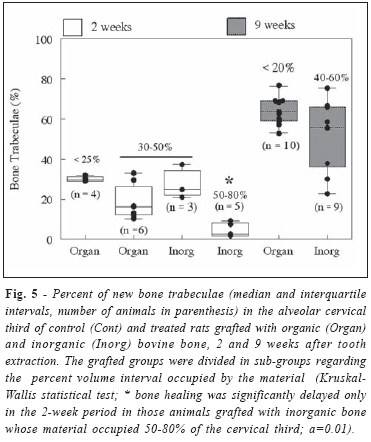
Brazilian Journal Oral Sciences, Vol. 7, No. 24, Jan/Mar 2008, pp. 1512-1519 Comparison of rat bone healing following intra-alveolar grafting with organic or inorganic bovine bone particles Romeu Felipe Elias Calixto1* Juliana Mazzonetto Teófilo2* Luiz Guilherme Brentegani2* Teresa Lamano2* 1Graduate Student in Oral Rehabilitation 2Professor, Department of Morphology, Stomatology and Physiology *Dental School of Ribeirão Preto, University of São Paulo, Ribeirão Preto, SP, Brasil Received for publication: December 10, 2005 Accepted: May 29, 2008 Code Number: os08009 Abstract Aim: This study compared, histometrically, the alveolar bone healing after grafting rats extraction socket with particles of organic or inorganic bovine bone. Key Words: organic bovine bone graft, inorganic bovine bone graft, alveolar healing Introduction The stomatognathic system is not infrequently submitted to a progressive bone deficit due to tooth extraction or loss, a situation that accelerates alveolar bone absorption and, when it triggers bone ridge atrophy, greatly hinders the placement of both conventional and implant-supported prostheses, while osseointegrated implants can barely be installed or are completely unusuable1-3. Therefore, preservation of the alveolar process in areas of tooth loss and adoption of procedures that minimize bone loss or recuperate the desirable alveolar ridge dimensions are important goals in dental practice. Clinical situations including those described above benefit from the use of biomaterials that may replace lost bone or stimulate osteogenesis. The most predictable results for replacement, reconstruction or filling of bone defects are still obtained with the use of autogenous porous bone grafts, despite their shortcomings such as surgical morbidity of the donor source and limited availability of healthy graft material. The alternatives to autografts include homogenous (allogenic) and heterogeneous (xenogenic) bone grafts4, besides a great variety of synthetic materials, each of which presents specific chemical composition and physical characteristics which are more adequate for particular applications. The wide availability and low cost of bovine bone, allied with the adequate processing that minimizes the risks of infection transmission, have led Brazilian, Canadian and European companies to produce bovine bone grafts for medical and dental applications1,4. Heterogeneous bone grafts may consist of inorganic fragments, in which the organic matrix components are removed and the mineralized elements, consisting mainly of hydroxyapatite, attain an osteoconductive surface behavior. The organic (decalcified) fragments, on the other hand, have their mineral components and cells removed, leaving only a protein scaffold composed mostly of type I collagen plus a small amount of other matrix proteins, including bone morphogenetic proteins (BMPs), potentially capable of osteoinduction4. Although studies on biomaterials have progressed considerably, the great variability of clinical and experimental models has hindered evaluation of the results that had sought to define the best material for specific dental or medical applications. Thus, the present study aimed to compare, by means of histological and histometric analysis, the behavior of organic and inorganic bovine bone particles grafted into the rat alveolar socket immediately after tooth extraction, as well as their interference in alveolar bone healing. Carried out in the same animal specie and in an identical experimental model, the specie-specific and among receptor bones differences, which might make comparisons unviable, have been reduced. Material and Methods Male Wistar rats (250 g initial body weight) were anaesthetized with 2,2,2-tribromoethanol (Aldrich, Milwaukee, USA; 25 mg/ 100 g body weight i.p.) and the upper right incisors were extracted. Immediately after tooth extraction, the alveolar socket of half of the animals were filled with particles (from 0.25 to 1.00 mm in diameter) of either Organic or Inorganic Liofilized Bovine Bone Matrix (Gen-ox®, Genius®, Baumer, São Paulo, SP, Brasil) mixed with a minimum volume of sterile saline and introduced with the aid of flexible polyethylene canule and embolus. The wounds in the control (non-grafted) and grafted animals were sutured with mononylon 4-0 (Ethicon, Johnson & Johnson, São José dos Campos, SP, Brazil) and a single dose (0.2 mL per rat, intramuscularly) of a polyvalent veterinary antibiotic (Pentabiótico Veterinário; Wyeth, São Bernardo do Campo, SP, Brazil) was administered. The rats were housed under climate-controlled environment (12 h light/12 h dark; 22 ± 3oC) with free access to standard laboratory chow and tap water. All procedures were conducted in compliance with ethical principles for animal research, as approved by institutional guidelines (Protocol 04.1.669.53.4). The animals were killed with an intraperitoneal overdose of sodium pentobarbital 1, 2, 3 and 9 weeks postoperatively (n=5 per group in the 1 and 3-week groups, for histological analysis, and n=10 per group in the 2 and 9-week groups, for histological and histometric analysis) and the heads were immersed in 10% formalin solution for 48 h. After fixation, the maxillae were dissected free, decalcified and processed for paraffin embedding. Semi-serial longitudinal 6-µm-thick sections of the hemi-maxillae containing the alveolar sockets were cut at 60µm intervals and stained with haematoxylin and eosin. Histometric analysis The degree of new bone formation inside the alveolar socket was estimated at the end of the 2nd and 9th postoperative weeks in the cervical alveolar third (where the grafted particles were located), by a differential point-counting method using an integration eyepiece with 100 equidistant points. A total of 500 points were counted in five histological sections per alveolus (final magnification X100), the percentage of points lying on the particles, on the connective tissue or on bone trabeculae being proportional to their volume density. The measures were standardized in the grafted and non-grafted sockets to avoid interference of regional differences in the rate of bone healing. The healing process, which in this phase consists of a gradual replacement of connective tissue by bone trabeculae, was estimated by new bone volume fraction (% bone trabecule relative to bone trabeculae plus connective tissue). Differences among groups were analyzed by the non-parametric Mann-Whitney and Kruskall-Wallis tests (α = 0.05 for statistical significance). Results Both organic and inorganic bone graft particles of irregular shape and variable size were observed partially filling the cervical third of the alveolar sockets (Figures 1A, 2A) and evoked neither a foreign-body reaction nor a persistent inflammatory response. By the end of the 1st week, the organic bone graft particles were surrounded by a granulation tissue rich in fibroblasts and newly formed capillaries with scarce osteoid matrix forming proximally but interspersed with a thin connective capsule (Figure 1A). By the 2nd and 3rd weeks, as the reparational osteogenesis developed, the particles were progressively enclosed by increasing amounts of newly formed bone trabeculae that were interposed intermittently among the particles and, in some cases, in close contact with their surface. Variable degree of absorption was observed in some particles, forming lacunae filled by connective tissue with discrete areas of mineralized bone matrix (Figure 1B). By the end of the 9th week, a conspicuous decrease in the particle size was observed and some of these particles were completely incorporated into the new bone trabeculae filling the alveolar socket (Figure 1C). Regarding the inorganic bone graft, by the end of the 1st week an osteoid matrix forming from the inner surfaces of the alveolar walls approached the particles but did not establish contact with their surface. By the 2nd week, newly formed bone trabeculae were in close contact with the surface of some particles (2B) and in a few of them narrow absorption lacunae filled by connective tissue were observed (Figure 2C). By the 3rd and 9th weeks, the amount and maturation of new bone trabeculae interposed among the particles had progressed and in some cases a close contact between them was observed. The amount of particles presenting wider absorption lacunae filled by connective tissue increased and, by the 9th week, in a few particles thicker absorption lacunae filled by mineralized bone trabeculae surrounding medullary vascularized connective tissue were noted (Figure 2D). Histometric data confirmed a progressive new bone formation from the 2nd to 9th weeks post-extraction in both grafted and control groups and showed that the presence of either organic or inorganic bone grafts impaired alveolar bone healing. Moreover, in the 2-week period the delay in bone healing was more pronounced in the animals grafted with inorganic bone than in those grafted with organic bone particles (Figure 3). The volume fraction of inorganic bone particles filling the alveolar socket was larger than that of organic bone particles in both the 2- and 9-week groups (Figure 4). In order to investigate a possible association between the relative amount of material and the degree of bone healing, each grafted group was divided in sub-groups according to the relative volume interval filled by the particles (Figure 5). In the 2-week period, in 4 animals grafted with organic bone the material occupied less than 25% whereas in 6 animals the material occupied 3050% of the cervical alveolar third. In the same period, inorganic bone particles occupied 30-50% in 3 animals and 50-80% of the cervical third in 5 animals. Multiple comparisons among grafted sub-groups showed that bone healing was significantly delayed only in those animals grafted with inorganic bone whose material occupied more than 50% of the cervical third. Regarding the 9-week period, all the animals grafted with organic bone had less than 20% particle filling whereas in the animals grafted with inorganic bone the particles occupied 40-60% of the cervical alveolar third. In this period, despite the greater volume fraction of inorganic bone graft the percent of bone healing was not statistically different from that observed in the animals grafted with organic bone. Discussion In the present study, the different phases of alveolar healing were recognized by histological examination in the sockets of control and grafted rats from 1 to 9 weeks after tooth extraction. The chronology of bone healing that follows tooth extraction has been well established in human and in different animal species. The healing process starts with filling of the extraction socket with a blood clot, which is gradually absorbed and replaced by immature connective (granulation) tissue, and culminates with its filling by new trabecular bone5. Although histological analyses have suggested that rat alveolar healing is completed by the end of the 3rd week after tooth extraction6, quantitative studies have shown a discreet but significant increase in bone neoformation up to the sixth5 or eighth7 week. Nevertheless, it has been proven that the greatest proportion of bone formation8 and the maximum mineral bone density7 take place by the end of the 2nd week. In the present study, the histometric analysis of bone healing was carried out at the end of the 2nd and 9th weeks after tooth extraction, thus comprising both the period of maximum new bone formation and the end of the healing process. Both organic and inorganic bone graft particles were always observed partially filling the cervical third of the alveolar sockets. Despite an attempt to achieve a more profound implantation, due to the curvature of the extraction socket and also to the pressure exerted by bleeding, the materials were located superficially at all times, which constitutes one of the inconveniences of this experimental model, particularly in small animals. The volume fraction of inorganic bone particles filling the cervical alveolar third was larger than that of organic bone in both the 2- and 9-week groups. Despite an effort to standardize the grafting procedures, it was not possible to determine the precise amount of particles introduced into the sockets. It is worth emphasizing, however, that the small variability among animals observed in the material volume density allowed statistical comparison of the data. In addition, it is known that organic and inorganic bone grafts are absorbed at different rates in biological fluids. A rapid absorption of organic bovine bone grafted in the extraction socket9 and in bone defects created in guinea pig calvaria10 was confirmed in the present study by a noticeable decrease in particle size observed by the end of the 9th week, with some of these particles being completely incorporated into the new bone filling the alveolar socket. In contrast, absorption lacunae were observed only in a few particles of inorganic bone at the same time point, thus confirming the extremely slow absorption rate of this graft material11-13. In a recent review of biomaterials for human maxillary sinus augmentation, inorganic bone was considered a nonabsorbable grafting material14. The presence of either organic or inorganic bone particles impaired the intra-alveolar bone healing. The tooth extraction socket is a place of hard asepsis procedures which heals by means of cells originating from the periodontal ligament remnants, so that any material contacting the periodontal ligament remnants is expected to prolong the inflammatory phase and retard the coagulum organization, thus retarding the reparative new bone formation15. Besides, despite the frequent need to use biomaterials to preserve or restore bone mass, it should be considered that any material introduced into a bone defect may slow down the healing process since graft absorption is a prerequisite for the completion of healing. The biocompatibility as well as the osteointegrative and osteoconductive properties attributed to inorganic bovine bone graft were corroborated in the present study, which also confirmed that the material can delay bone healing. Experimental and clinical studies from the 50s and 60s have recommended inorganic bone grafts for the correction of oral and craniofacial bone defects. This material, however, has been reported to elicit an intense and persistent inflammatory reaction in the tooth extraction socket of rats, consequently delaying alveolar bone healing15,16 for references. Bio-Oss® (Geistlich Sons Ltd, Wolhusen, Switzerland) is a grafting material chemically and structurally comparable to that used in the present study, and has been tested in medical and dental clinics since the 90s with reports of biocompatibility, osteointegrative and osteoconductive properties13,17. Both clinical and histological analyses in humans have suggested that this material is adequate for filling tooth extraction sockets18 and correcting both alveolar bone ridges19 and periodontal osseous defects20. STAVROPOULOS et al.11, however, emphasized that most of the clinical reports are descriptive and vague, lacking appropriate controls, and warned that conclusions based merely on clinical and radiographic studies may be imprecise. The authors also suggested that the reports of clinical success probably refer to their use in small bone defects. Furthermore, although histometric studies of maxillary sinus augmentation21 and extraction socket healing22 in humans have suggested that the volume density of reparational bone is not negatively affected by Bio-Oss®, it is worth mentioning that both studies also lack appropriate (non-grafted) controls. Experimental studies showing a possible benefit from Bio-Oss® for correction of calvaria bone defects in rats and of mandibular bone defects in dogs have also been contested11 (for references). A histometric study in rats also confirmed that grafting Bio-Oss® as an adjunct to guided tissue regeneration arrests new bone formation in mandibular bone defects11. The presumed osteostimulatory property of organic bone grafts was not confirmed in the present experimental model. Since the pioneering study by Urist23, several studies in the 70s and 80s confirmed the capacity of demineralized bone powder to promote ectopic osseous formation and to stimulate bone healing in both craniofacial and long bone defects in different animal species9 for references. It has been considered that bone demineralization renders the matrix proteins (particularly the BMPs and some growth factors which account for the osteostimulatory potential of the organic bone matrix) bioactive and available for interaction with local cells24 for references. However, the osteoinductive efficacy of organic bone grafts of both laboratory and commercial origin, ectopically or orthotopically grafted, has been confirmed in some but not all experimental and clinical reports and appears to depend on the embryologic origin of the graft, on the age and physiological state of the donor as well as on the processing method and particle size25,26. The favorable response of human bone defects to organic bone grafts has been suggested in dental clinical practice by histological and radiographic observations27 and a recent review proposed the efficacy of this material in the treatment of human periodontal osseous defects28. Conversely, histological examination of human extraction sockets revealed no evidence of bone formation up to 12 weeks after grafting with organic bone particles29. Since the unpredictability of the results has cast doubts on the use of organic bone as an osteoinductive graft material in the dental clinic, mainly as an adjunct to periodontal therapy, LI et al.30 carried out an investigation to determine whether there were detectable levels of 2- and 4-BMPs in 3 commercial preparations of organic bone grafts and reported no detectable amount of either protein in the tested samples. Experimentally, favorable results have been reported in response to homogenous organic bone powder grafted in the rat tooth extraction socket9 and in response to commercially available organic bovine bone grafted in critical defects produced in rats and guinea-pig calvaria10, 31, 32. Conversely, homogenous organic bone particles grafted in the dog tooth extraction socket exhibited no osteoinductive property up to 12 weeks post-implantation33; 12 commercially produced organic bone grafts ectopically implanted induced only insignificant amounts of bone formation34; blocks of bovine porous organic bone ectopically grafted in rats were almost totally absorbed after 4 weeks without any sign of osteogenesis1. Comparison of literature reports concerning the behavior of biomaterials has been hampered by lack of quantitative or histometric data as well as by factors such as differences in animal species, implantation sites, the amount and size of grafted particles, and in the follow-up periods14. In the present study, two different biomaterials having the same particle size were compared in the same experimental model and the results showed a significant degree of negative interference with alveolar bone healing outcome due to a combination of factors such as the nature and relative amount of the materials and also the phase of the reparative process. In the initial phase (2 weeks), the same degree of impairment was triggered by organic and inorganic bone grafts, provided that similar relative volumes of the alveolar socket were occupied by both materials; greater relative volumes of inorganic bone, however, resulted in a more deleterious effect on the reparative process. In the 9-week period, both materials appeared to prompt the same degree of negative interference with alveolar bone healing, independently of their relative amount. These results demonstrate that, lacking a proposed osteoinductive property, the organic bone graft may behave as an osteoconductive surface, as is expected for inorganic bone grafts. In conclusion, the present results showed that, considering the particularities of the present experimental model, although biocompatible and capable of different degrees of osseointegration, both organic and inorganic bovine bone grafts hindered the alveolar bone healing process. Although a direct extrapolation to medical and dental applications is nonviable, the present results affirm the need for a reexamination of the selection of biomaterials to replace lost bone or to stimulate osteogenesis. Acknowledgments The authors are indebted to Edna A. S. Moraes, Antônio de Campos, Adriana M. G. Silva e Gilberto A. Silva, for technical assistance, and to Genius-Baumer which gently supplied the implant materials. Research supported by CNPq (300599/ 2003-0). References
© Copyright 2008 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os08009f5.jpg] [os08009f1.jpg] [os08009f2.jpg] [os08009f4.jpg] [os08009f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}