 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
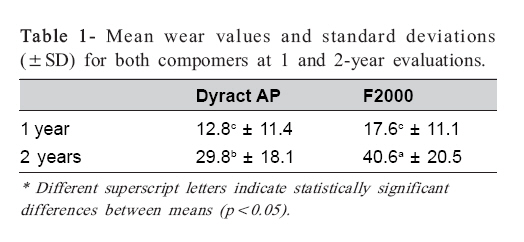
Brazilian Journal of Oral Sciences, Vol. 7, No. 25, Apr-Jun, 2007, pp. 1539-1542 Two-year clinical wear performance of two polyacid-modified resin composites (compomers) in posterior permanent teeth Rafael Guerra Lund1 ; Evandro Piva2; Flávio Renato Reis de Moura3; Flávio Fernando Demarco1; Janaína de Oliveira Lima4; Paulo Eduardo Capel Cardoso4 1DDS, PhD student, Department of Restorative Dentistry, Dental School, Federal University of Pelotas, Brazil Received for publication: March 31, 2008 Accepted: July 1, 2008 Code Number: os08014 Abstract Aim: The aim was to compare the clinical wear of two compomers (F2000; 3M/ESPE and Dyract AP; Dentsply) placed in occlusal cavities in permanent molars within a two-year follow-up period using an indirect method of evaluation. Key Words: Dental restoration wear; Compomers; Clinical trials; Dyract AP; F2000. Introduction Polyacid-modified resin composites, also called compomers, have been developed to improve the physical and mechanical properties of conventional glass ionomer cements (GICs)1, and have been classified as intermediate materials between GICs and composite resins2. When compared to resin-modified glass ionomers (RMGICs), compomers contain larger amounts of monomers in their formulation and release low fluoride levels with a recharge capacity. The better clinical performance of compomers when compared to GICs has been demonstrated3. Moreover, compomers offer excellent esthetics and are ease to handle, which are some of the reasons for their popularity4, especially in pediatric dentistry5 6. Compomers are basically composed of dimethacrylates, modified monomers and fluoride-releasing charges, and contain a proportion of hydrophilic monomer in their organic matrix. The monomer has carboxylic acid groups and polymerizable methacrylate groups, which enables a free-radical polymerization by light curing and an acidbase reaction if water is present. Due to continuous improvements in their physical properties and clinical performance, compomers have been used to restore primary teeth and cavities in stress-bearing areas on permanent teeth7-8. The wear resistance is an important property to be evaluated in materials indicated for posterior teeth. The restoration should not only be satisfactory at the time of placement, but also remain this way over time. Toothbrushing, interdental contacts and masticatory movements are some of the wear-inducing factors. The abrasive agents abrade the resin matrix and exposes fillers, which may then be exfoliated from surface. The increase of surface roughness causes accumulation of bacterial biofilm, pigments and food debris, which impairs the longevity of the restoration9 . Taylor et al.10 evaluated the wear of posterior composite restorations using a series of methodologies. Two of them were widely used measuring techniques: a direct evaluation, based on the clinical observation of the restoration, and an indirect method that measures the wear in models obtained from restorations in the mouth. While the direct method provides a subjective evaluation, the indirect method provides a numeric estimative, using standard models of worn restorations. This method is more objective and eliminates many variables. Compomers have shown a good performance in primary molars6,11-13. When used in ultraconservative cavities in permanent posterior teeth, the clinical performance of these materials was considered as satisfactory14-15. Other studies investigating the behavior of compomers in stress-bearing areas7,16-17 have also observed a good clinical performance. The purpose of this study was to compare the clinical wear of two compomers placed in occlusal cavities in permanent molars within a two-year follow-up period using an indirect method of evaluation. Material and Methods Patient Selection Patients attending the Operative Dentistry clinic at the Dental School of the Federal University of Pelotas for routine restorative care were examined as eligible patients for the trial. Subjects were enrolled if they needed at least one pair of restorations in the posterior permanent teeth and if the cavities were no larger than 1/3 of the intercuspal distance. Patients with tooth loss, parafunctional habits or prostheses were not included in this study. Twenty-five patients aged 20 to 32 years (mean age = 25 years) were selected. Before any restorative procedure, patients were informed about the study purposes and signed a written informed consent. The research protocol was approved by the Research Ethics Committee of the Federal University of Pelotas (Medical School). Restorative Procedures Right after medical history review, clinical and radiographic examinations were performed. Local anesthesia was administrated and the procedures were carried out under rubber dam isolation. Cavity preparation was restricted to caries removal with dentin excavators and round carbide burs under air/water cooling. Cariesdisclosing agents were used to help distinguishing the outer and the inner carious dentin layers and perform minimal dentin removal without affecting adhesion18. In deep cavities, indirect pulp capping was performed with a calcium hydroxide-based cement (Hidro C; Dentsply Ind. e Com. Ltda., Petrópolis, RJ, Brazil) prior to the adhesive protocol. Fifty cavities were prepared in molars (24 maxillary and 26 mandibular). Both materials were applied in the same patient and they were equally distributed between maxillary and mandibular teeth. For the adhesive restorative protocol, the cavities were etched with a 35% phosphoric acid gel (Dentsply, Milford, DE, USA) for 20 s, rinsed and gently dried with a mild air stream for 5 seconds at a distance of approximately 10 cm from tooth surface in order to keep the dentin moist. Two coats of Prime & Bond 2.1 (Dentsply) or Single Bond (3M/ ESPE, St. Paul, MN, USA) were applied and then the cavities were incrementally filled with either Dyract AP (Dentsply) or F2000 (3M/ESPE), respectively. Each increment of less than 2 mm was light cured for 40 seconds using a halogen light-curing unit with irradiance higher than 450 mW/cm2 (XL3000; 3M/ESPE) as measured with a curing radiometer. The occlusion was checked after removal of rubber dam. The restorations were finished and polished one week later using multi-blade carbide burs (KG Sorensen, Alphaville, SP, Brazil), Enhance Polishing System (Dentsply) and diamond polishing pastes (Diamond; FGM, Pomerode, SC, Brazil). Only one operator performed all the procedures. Wear Evaluation Polished restorations were considered the baseline and impressions were taken with polyvinylsiloxane (Express; 3M/ESPE). To be included in the clinical evaluation, restorations should be classified as Alfa for all the items of the criteria of modified USPHS system19. A single examiner blinded to the materials used in each case and not the researcher who placed the restorations, performed all evaluations. After 1 and 2 years, the same examiner revaluated the restorations clinically and took new impressions. Models for indirect evaluation of wear were obtained with type IV die (Durone; Dentsply). Twenty-one patients with 42 restorations (84% recall rate within 2 years) returned in all clinical appointments. Models of the Leinfelder scale were used to perform the visual readings of wear in comparison to the models obtained from the compomer restorations. The scale was composed by models of different simulated wear in occlusal cavities: 0, 25, 50, 75, 100, 125, 150, 175, 200, 250, 300, 350, 400, 500, 600, 700, 800 and 900 ìm. An experienced examiner made the comparisons at the Laboratory of Dental Materials of the University of São Paulo, Brazil. The occlusal surface of each tooth was uniformly divided in four parts (quadrants). The mean of maximum wear in each quadrant (deeper area at restorations margins) was recorded and a mean wear value was obtained for each tooth. Statistical Analysis The values at baseline, 1 year and 2 years were used for the statistical analysis. Data had a normal distribution and equal variances, allowing parametric tests to be performed. A paired t-test was used to compare each material in both follow-up periods and a t-test was used to identify differences between materials for each evaluation period. A 95% confidence level (p<0.05) was set for all tests and SigmaStat 3.0 for Windows statistical package (Systat Software Inc., Chicago, IL, USA) was used. Results Table 1 presents the mean wear values and standard deviations (±SD) for both compomers after 1 and 2-year evaluations. The paired t-test, applied for comparisons at the different periods for each material showed an increase in the wear of the restorations after 2 years compared to the results obtained at 1 year (p<0.001). F2000 had a significantly higher wear mean value at 2 years compared to Dyract AP (p<0.05). The materials had similar behaviors at 1-year evaluation. For both materials, the wear of the restorations at 2 years was approximately 2.3 times greater than that recorded at the 1-year evaluation. Discussion In vitro studies are less expensive and faster than clinical trials, and play a key role as an initial characterization of the mechanical properties of restorative materials. On the other hand, only long-term clinical evaluations can determine the real performance of the materials in the oral environment20. A clinical evaluation period of at least 2 years has been recommended before any dental restorative material can be launched to the market21 . In the present study, compomer restorations were placed used after a total-etch adhesive technique. According to Dyract AP’s manufacturer, TCB (tetracarboxylic butane acid), a hydrophilic monomer with two methacrylate and two carboxylic groups was added to this product. Therefore, 50% of the reactive groups of each molecule are composed by carboxylic acid. These groups are responsible for the bonding of the material to the dental structure. In the present study, the total-etch technique was used to improve bonding ability20 because there are more mechanical requirements in class I cavities in permanent posterior teeth than in cavities prepared in primary teeth. The size of the inorganic fillers can influence the clinical performance and may account for the differences observed in this study. While Dyract AP has 2.5 µm strontiumaluminum-fluoride-silicate glass filler, with a mean filler size of 0.8 µm, F2000 contains a glass filler of fluoridealuminum-silicate, with 3-10 µm size range and mean particle size of 6.5 µm. In addition, colloidal silica is added to increase the packability of the inorganic matrix. It is well known that smaller fillers provide better resistance to wear89,22. Data from the 1-year evaluation, first stage of the present clinical trial16 showed greater surface roughness for F2000 restorations compared to Dyract AP restorations. A rougher surface can accelerate the abrasion caused by foods, leading to an increase in the restoration wear9 . The interaction between the matrix and water is probably the reason for the higher wear of the compomers when it is compared to the composites22. The desired fluoride release from compomers can cause material dissolution23, leading to superficial degradation of the restoration. This finding could also influence the increase in clinical wear observed at the 2-year follow-up. Clinical studies in primary molars6 and permanent molars8,16 have showed satisfactory performance for Dyract AP. In the present study, Dyract AP exhibited better performance than F2000 after 2 years, which may be related to the improvements undertaken in Dyract AP formulation. Dyract AP received an additional crosslinker, and the size of the glass particles was reduced to improve the resistance to wear6 . In the present study, occlusal Class I cavities with a maximum intercuspal distance of 1/3 were prepared in permanent teeth. Manhart et al.24 demonstrated that Class I restorations are more likely to have a good clinical performance than Class II restorations. In a 17-year clinical evaluation of posterior composite restorations, Rodolpho et al.25 verified that the survival rates decreased significantly for 2, 3 and 4-surface restorations compared to 1-surface occlusal restorations. Comparing the follow-up periods of the present investigation, the restorations were submitted to clinical conditions responsible for material aging and higher wear values was recorded in the second moment. There is a positive correlation between the length of the evaluation period and the failure rate. Thus, short-time studies have the tendency to produce more favorable results for the tested materials24-26 . Two experimental groups were evaluated in this study and a control group was not employed, which an important limitation of the study. The use of a control group with a well established composite could provide important parameters for comparison. However, if another group were used in this study, we would probably have some difficulties to fulfill all requirements for inclusion criteria, i.e., the number of Class I cavities needed per patient with similar characteristics. The indirect method used in the present study (Leinfelder scale) has been considered a good resource to evaluate the wear of dental materials in clinical studies27. However, the Leinfeder’s method assess only marginal wear and not the wear on contact-free area/occlusal contact area. It should be highlighted that small cohesive failures at restoration margins and degradation events other than tooth and food attrition may also affect wear, which means that clinical wear is a complex process. Three-dimensional laser digitizing technique has been advocated and could be significantly more effective than subjective evaluations, like cast models evaluations (Leinfelder scale) in establishing restoration wear rates28. Additionally, the cast model-set employed for wear measurements is critical because significant differences can be found with different scales (M-L scale and Leinfelder scale)10 . Manhart et al.24 performed a review reporting the longevity of restorations in stress-bearing posterior cavities in permanent teeth. The mean (SD) annual failure rates in posterior cavities for some materials were: 3.0% (1.9) for amalgam restorations, 2.2% (2.0) for direct composites, 1.1% (1.2) for compomer restorations, 7.2% (5.6) for regular glass ionomer restorations, 6.0% (4.6) for ART glass ionomers, 2.9% (2.6) for composite inlays, 1.9% (1.8) for ceramic restorations, and 1.4% (1.4) for cast gold inlays and onlays. However, most cavities prepared to receive compomer restorations were more conservative than those prepared for direct composites. The adhesive technique used in the present study provided an adequate retention level along 2 years of clinical wear evaluation. The wear observed for both materials (approximately 30 and 40 µm for Dyract AP and F2000, respectively) is within the range required for full acceptance of materials intended for use in posterior restorations, according to ADA acceptance guidelines requirements29. The mean wear values found for both compomers do not indicate the need for either repair or replacement of the restorations. References
© Copyright 2008 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os08014t1.jpg] |
| |||||||||

{kind=link}