 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 7, No. 25, Apr-Jun, 2007, pp. 1543-1549 Susceptibility of Candida spp. Oral isolates for azolic antifungals and amphotericin B Vivian Fernandes Furlletti1,2; Rita de Cássia Mardegan1,2; Gustavo Alberto Obando-Pereda1; Paula Cristina Aníbal1,2; Marta Cristina Texeira Duarte2; Reginaldo Bruno Gonçalves1; José Francisco Höfling1 1Department of Microbiology and Immunology, Dental School of Piracicaba, University of Campinas - UNICAMP, 13414-903 Piracicaba, SP, Brazil. Received for publication: May 8, 2008 Accepted: July 31, 2008 Code Number: os08015 Abstract Aims: Among the oral infections, candidosis may be considered the most frequent, and C.
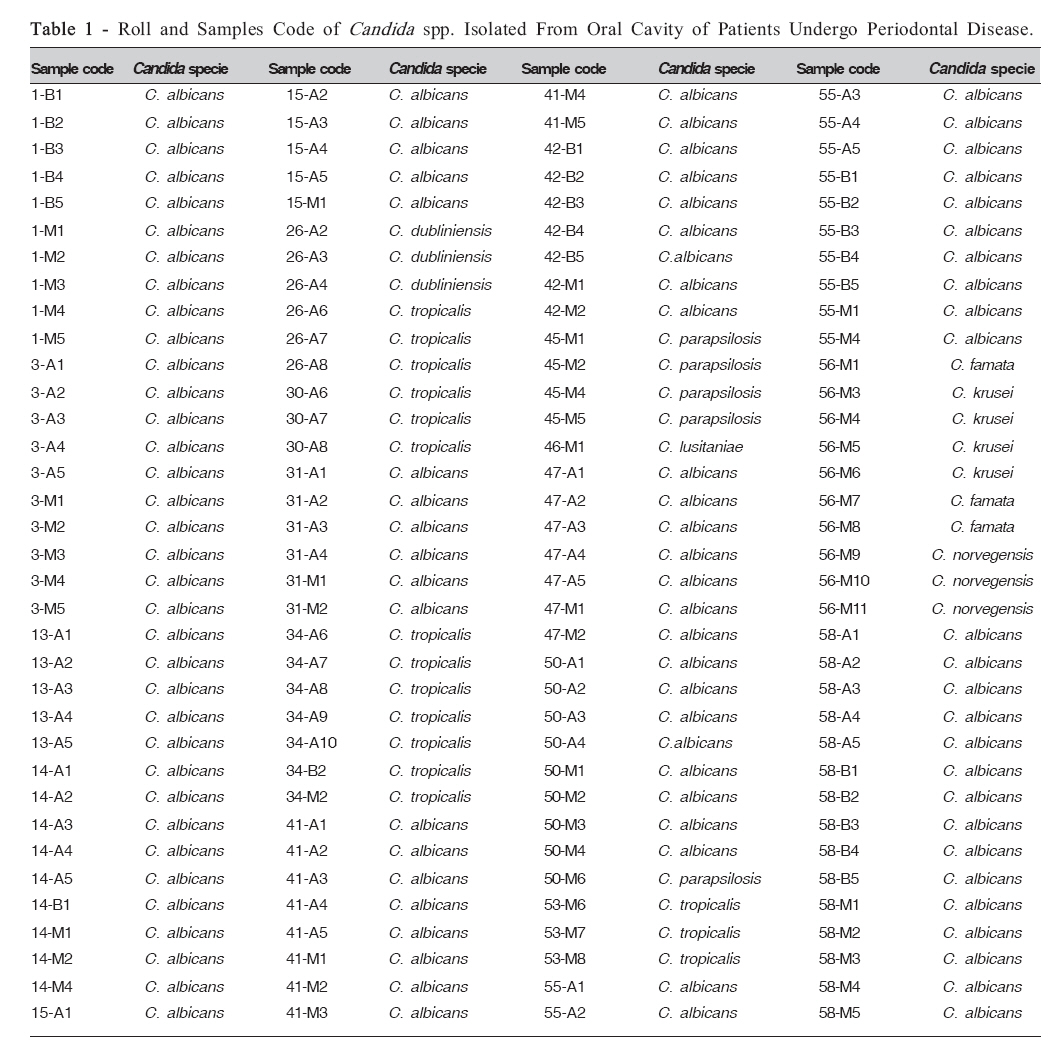
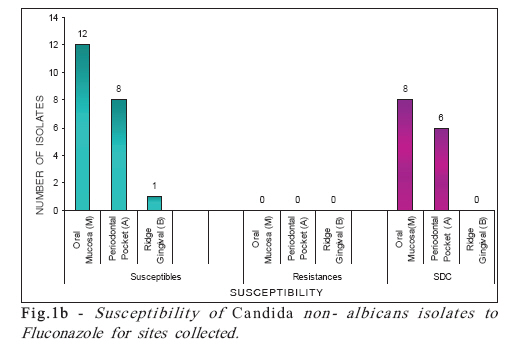
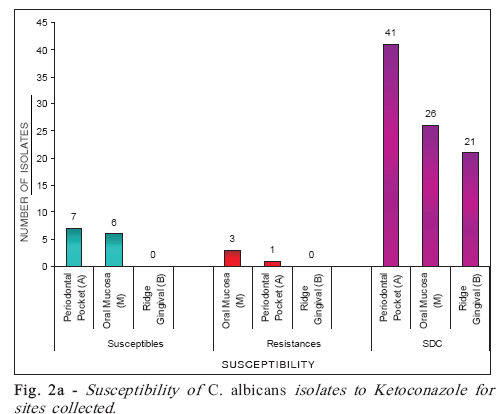
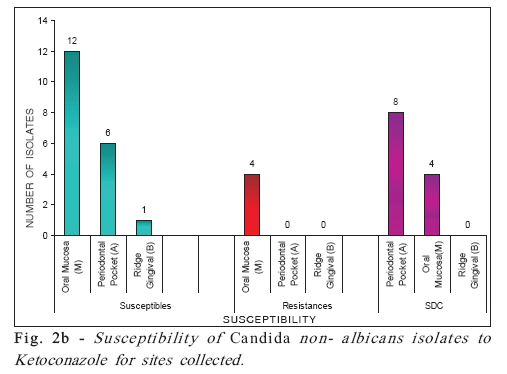
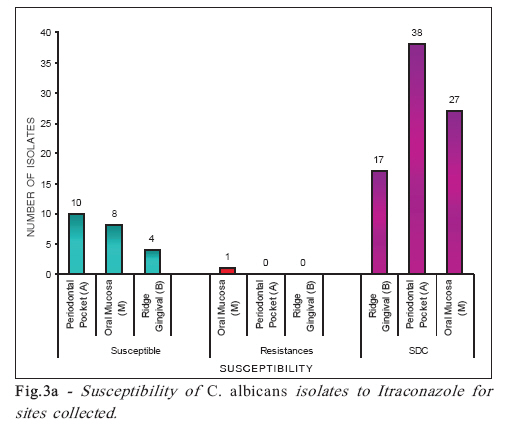
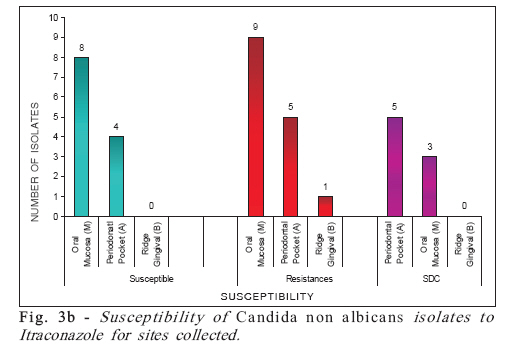
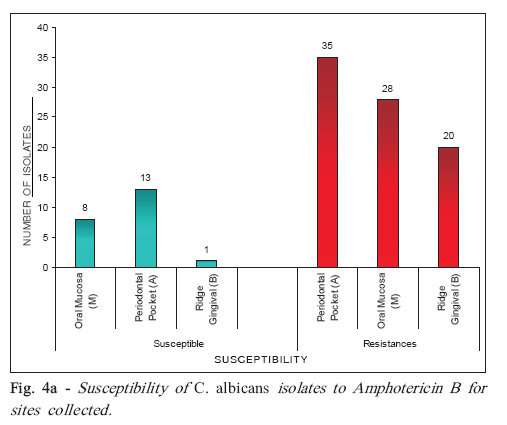
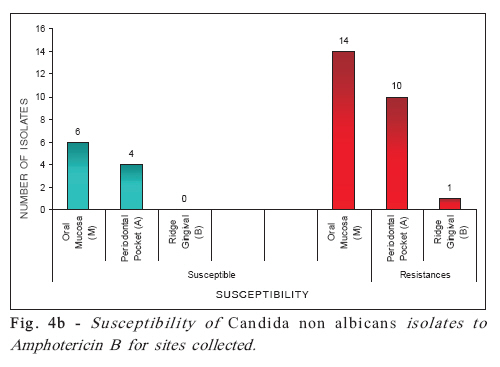
albicans the most prevalent species. Meanwhile, the non-albicans species may also be related to other infections processes and be able to affect the oral cavity, including periodontal disease. In this sense, understanding the relationship between Candida spp. and host, it is necessary and justified the search of mechanisms modulators of infections and treatments against diseases associated with these yeasts. Key Words: Periodontal disease, Candida spp., antifungical, minimal inhibitory concentration. Introduction Fungal infections are more common today than ever before. There are a number of reasons for this. People are living longer, and older people are more likely than younger people to have compromised immune systems, a major risk factor for fungal infection. Similarly, the widespread use of antibiotics has contributed to the growing infection rate (fungal infections are known to occur after antibiotic therapy, which has the effect of killing the beneficial bacteria that normally suppress fungi). Finally, the success in treating diseases like HIV/AIDS has created a subgroup of the population susceptible to fungal infections1 . The most common organism implicated in fungal infections is the ubiquitous Candida , which is found in the human digestive tract, mouth, and genital region2 . Under normal circumstances, levels of Candida are controlled by commensal bacteria. However, if the bacteria-fungi balance is upset by the use of antibiotics, for example, or if the immune system is compromised, an overgrowth of Candida could occur, resulting in infection3 . More than 20 different species of Candida have been reported as etiologic agents of invasive candidiasis in humans4-5 though more than 90% of invasive infections due to Candida spp. can be attributed to species C. albicans , C. glabrata, C. parapsilosis, C. tropicalis , and C. krusei . The roll of reported species continues increasing as laboratories are pushed to provide an identification to the species level as an aid in optimizing therapy of candidal infections6-10 . Likewise, the diverse array of opportunistic yeasts and yeast-like fungi and their variable susceptibilities to both new and established antifungal agents has made the need for prompt identification of non-Candida yeasts from clinical material much more compelling6,11-12 . Our understanding of the frequency of occurrence and the antifungal susceptibility of both Candida and non-Candida yeasts has been enhanced in recent years through the efforts of several large surveillance programs conducted throughout the world8,13-20 . Fungal overgrowth is encouraged by certain pH levels and the availability of sugar (glucose) 21-23. People with the right conditions for fungal infection, such as a high sugar diet, are at higher risk. Also, Candida infections can be spread to vulnerable people with depressed immune systems who are in the hospital, where the fungus is commonly found on the hands of caregivers and where indwelling catheters can allow an infection to take hold. The number of available drugs for the treatment of systemic fungal infections is limited. The antifungals known nowadays can be classified into azolic and polienics. The azolics are elected in the first instance for treating these diseases and are generally fungistatics, while the latter are fungicides. Among azolic are the fluconazole, ketoconazole and itraconazole. Among polienics we found the amphotericin B and nystatin. In recent years, the amphotericin B and azoles mainly ketoconazole, fluconazole and itraconazole - have been the drugs of choice in therapy24. The mechanism of action of the azoles drugs is based on the inhibition of sterol-14-to-desmetilase, an enzyme system dependent microsomal cytochrome P450, hindering the synthesis of ergosterol in cytoplasmic membrane and leading to accumulation of 14-to-methylsterols. These methyl-sterols not have the same form and physical properties that ergosterol and lead to the formation of the membrane with properties changed, that does not perform the basic functions necessary for the development of the fungus. The polienics connecting to a portion sterol, basically ergosterol present in the membrane of fungus is forming pores or channels. The result is an increase in permeability of the membrane that allows the escape of several small molecules, leading to cell death. The amphotericin B is a broad-spectrum antibiotic fungicide and powerful, but its use is associated with significant adverse effects such as nephrotoxicity with chills and fever, and acute reaction to the intravenous infusion, since the pharmacokinetics of this drug does not allow oral administration24. New formulations of amphotericin B, in the form of liposomes and colloidal dispersion, produce fewer side effects, as a result of redistribution of the drug in tissue and the selectivity of release, but the price of these formulations is often greater than that of old 25-27. The azoles cause less adverse reactions that the amphotericin B, but are less powerful than the same. They may have action fungistatic or fungicide. Excessive use of azoles led to the emergence of resistance in species susceptible. Moreover, the azoles still have the disadvantage of cross-resistance24, 28. The availability of information microbiological and epidemiological helps the doctors to choose the most appropriate antimicrobial agent for the treatment of infections. These susceptibility tests measure the ability of a microbial agent inhibit the growth of microorganisms in vitro. The microorganisms can be classified in categories according to drugs susceptibility, which may be sensitive (S), concentration dependent susceptibility (SDC) or resistance (R). Sensitive is the microorganism whose infection caused by it are prone to respond to treatment with the drug; sensitivity concentration dependent is the one whose infection depends on adequacy of dose to be controlled and resistance is the body that does not respond to a particular drug regardless of adequacy of the dose29. The aim of this study was to determine the pattern of susceptibility of yeast for some azoles antifungals and amphotericin B. Material and Methods Samples. C. albicans, C. tropicales, C. parapsilosis, C. krusei, C. famata, C. norvegensis, C. dubliensis and C. lusitaniae. The yeasts were selected from Microbiology and Immunology Laboratory Collection – Piracicaba Dental School, University of Campinas (FOP-UNICAMP), Piracicaba, SP, Brazil, including 140 isolates from three different sites of the oral cavity from 19 patients with periodontal disease, known as: periodontal pocket (A), oral mucosa (M) and ridge gingival (B). After activation, the identification of isolates was confirmed in Chromogenic Chromagar Candida® (Difco), API 20 system® kit (Aux System - BioMérieux, France) and microculture. The samples were maintained in Sabouraud Dextrose Agar (Merck) covered with glycerol at 4 oC and Yeast Peptone Dextrose with 15% glycerol at – 70 oC. The roll and samples code of Candida spp isolates are presented in Table 1. The codes of samples correspond to number of voluntary and precedence, being: A: periodontal pocket; B: healthy ridge gingival and M: oral mucosa. Antifungal drugs. The following antifungal drugs were used for susceptibility tests: fluconazol, ketoconazol, itraconazol (azolics) and amphotericin B (polienic) - Neon®. Susceptibility assay -Minimal Inhibitory Concentration (MIC) test. The yeasts was grown overnight at 36 °C in Sabouraud Dextrose Agar (Merck) plates. Inocula for the assays were prepared by diluting scraped cell mass in 0.85% NaCl solution, adjusted to McFarland scale 0.5 and confirmed by spectrophotometric reading at 580 nm. Cell suspensions were finally diluted to 104 UFC mL”1 in RPMI-1640 medium (Difco) for use in the assays. MIC tests were carried out according to CLSI (2002)30 , using tissue culture testplate (96 wells), containing 100µ L RPMI-1640 medium.The stock solutions of the antifungals were diluted and transferred into the first well, and serial dilutions were performed so that concentrations in the following range were applied in the wells: fluconazol, 640 - 1.25 µg mL+1; ketoconazole, 80-0.15 µg mL+1, itraconazole, 40-0.078 µg mL+1 and amphotericin B, 160-0.3 µg mL+1. The yeast inocula were added to all wells and the plates were incubated at 36 °C for 24 h. Antimicrobial activity was detected by change in the RPMI-1640 medium color (the pink color of the medium change to yellow after yeast growth by pH alteration). Results A total of 140 yeasts belonging to Microbiology and Immunology Laboratory Collection (FOP-UNICAMP) were tested for drugs susceptibility, as C. albicans (105 isolates), C. tropicales (16 isolates), C. parapsilosis (5 isolates), C. krusei (4 isolates), C. famata (3 isolates), C. norvegensis (3 isolates), C. dubliensis (3 isolates) and C. lusitaniae (1 isolate). The isolates of Candida spp. were studied for the susceptibility to antifungals fluconazole, ketoconazole and itraconazole, and were classified as sensitive (S), susceptibility dependent of concentration (SDC) and resistant (R), according to CLSI30 presented in Table 2. For amphotericin B, the MIC has been identified as the lowest concentration of drugs in middle-free growth of yeast, and classified as sensitive (S) or resistant (R). The results are shown in Figure 1a and 1b, 2a and 2b, 3a and 3b, and 4a and 4b. Discussion Among the 53 patients investigated, 19 undergo oral colonization by Candida spp, and 14 of them (26.4%) had colonization in the periodontal pocket. The presence of yeast in periodontal pockets has been reported in about 20% of patients with severe periodontal disease31-32 . Although not fully defined the participation of these organisms in the pathogenesis of this disease, the results are suggestive, considering the fact that all patients had not analyzed systemic diseases or factors that may contribute to the development of yeast infections, such as immunosuppression by use of antibiotics or steroids. The occurrence of resistance to azoles antifungal was greater for the group of Candida non-albicans (42.8%) compared to that seen in C. albicans (3.6%). It was possible to observe the occurrence of cross resistance between the antifungal ketoconazole and itraconazole, for five samples of three patients. Although the occurrence of resistance was low for azolic, there is a decrease in susceptibility to these antifungals, demonstrated by the high level of SDC, especially for ketoconazole and itraconazole. The fluconazole show to be the most effective for most samples from all tested species of Candida. Studies have shown that the susceptibility to antifungals azolic among isolates of Candida spp. of periodontal pockets can be variable; occurring cross resistance33-34 also highlighted the occurrence of cross resistance between the antifungal azolic, based in the presence of similar mechanisms of action. This shows different patterns of susceptibility of these strains to drugs tested1.This fact is corroborated recent data, which indicate a growing resistance among species of Candida to azoles antifungals, suggesting that the oral cavity could be a reservoir of resistant yeast35-36. A correct diagnosis should be considered in microbiological periodontal lesions refractory to conventional treatment. The joint application of antifungal treatment can be useful in cases of opportunistic infections by Candida spp. in periodontology, especially in patients at high risk of developing systemic candidiasis37. The high incidence of resistance to Amphotericin B found between the species analyzed indicates the need to make more accurate studies for this antifungal. Actually, considering the potential of azoles antifungal fungistatics and fungicide potential of amphotericin B (polienics) would be expected to find greater number of isolates sensitive to the latter and not the other drugs. Considering the relevant literature, it was found that there is a pattern of behavior of unusual clinical isolates regarding susceptibility to antifungals tested, since different authors found different results in this respect38 concluded in their work, that the effectiveness of two types of drug amphotericin B and fluconazole was equivalent. Thus, the results of this research may be suggestive of the occurrence of of strains resistant selection to conventional amphotericin B. The same has not happened with another form of presentation of amphotericin B, lipossomal, whose formulation allows the release gradual, but constant, the principle active38-40. This formulation has been regarded as a better therapeutic option in cases of resistance. Thus, the preliminary identification of microorganisms causing the disease and the appropriate concentration of the drug are important factors to avoid the selection of resistant strains. Ruhnke41 described the development of resistance to fluconazole in a patient with AIDS infected by C. albicans and C. dubliniensis simultaneously. The patient had recurrent oral candidosis because of the two species and under use of fluconazole for four years. Molecular analyses showed persistence of isolates during the same period, affecting the development of resistance in the two species. Researchs involving studies on the growth and susceptibility of Candida spp strains to a wide variety of antifungal drugs has expressed cross-resistance to antifungal amphotericin B and azoles in individuals who had or not contact with them, suggesting that it is not an effect on the metabolism of sterol, but that new mechanisms of resistance are involved in clinical isolates30,42-43. These data, added to those obtained in this study, suggest that to achieve effective therapy are necessary comparative studies between the various azolics and polienics antifungal normally used, confronting their mechanisms of action and factors of local origin as bad oral hygiene, presence of caries and prostheses, which caused the microbial accumulation. In addition, must still be considered factors of a systemic disorder related to the metabolism of the host, immunosuppressive therapies, malnutrition and infection by the HIV virus since the union of these conditions to the opportunistic microorganism contributes to the worsening of the disease33,44. The development of a program that includes routine tests for sensitivity to antifungal for tracking oral samples is necessary to determine the drug and the efficient concentration for the treatment. This also would avoid the selection of resistant strains whose susceptibility depends on the concentration of the drug33,44. Studies that will contribute to a greater understanding of the relationships between organisms and antimicrobials should be carried out in order to elucidate the complex mechanisms involving microbial resistance to drugs. Concluding, patients with periodontal disease showed relevant levels of colonization by Candida spp., mainly in the oral mucosa and periodontal pocket. Species of C. albicans was the most prevalent yeast in the oral microbiota considering the various sites analyzed, which confirm the previous findings. There is also an increase in the incidence of non-albicans species in these sites, together with a greater resistance to the latest drugs tested. Moreover, the patterns of susceptibility from C. albicans and non-albicans isolates to different antifungal studied differ considerably. There was no occurrence of resistance to fluconazole and small part of Candida spp. isolates showed susceptibility dependent on concentration (SDC) in relation to this drug, experiencing the opposite for ketoconazole and itraconazole. Most isolates are resistant to amphotericin B. Acknowledgments This research was supported by a grant from CNPq (Brazil). References
© Copyright 2008 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os08015f2a.jpg] [os08015t1.jpg] [os08015f4a.jpg] [os08015f2b.jpg] [os08015f3b.jpg] [os08015t2.jpg] [os08015f1a.jpg] [os08015f4b.jpg] [os08015f3a.jpg] [os08015f1b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}