 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
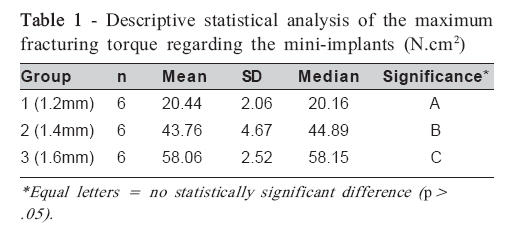
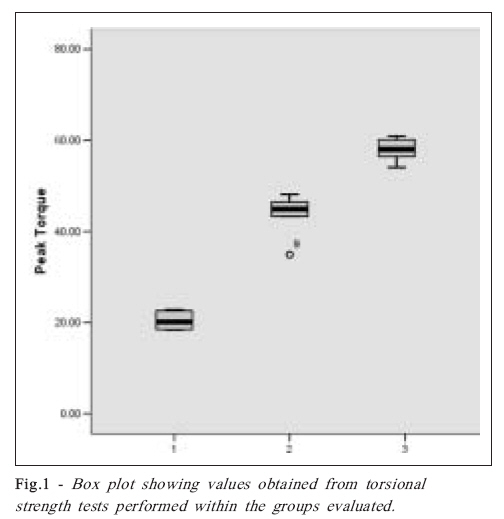
Brazilian Journal of Oral Sciences, Vol. 7, No. 25, Apr-Jun, 2007, pp. 1563-1565 In vitro evaluation of torsional strength of orthodontic mini-implants Matheus Melo Pithon1; Rogério Lacerda dos Santos1; Carla D’Agostini Derech2; Carlos Nelson Elias3; Antônio Carlos de Oliveira Ruellas4; Lincoln Issamu Nojima4 1DDS, Specialist in Orthodontics, Dental School, Federal University of Alfenas, Brazil; Student of the Doctor’s Degree Program in Received for publication: April 16, 2008 Accepted: August 23, 2008 Code Number: os08019 Abstract Aim: The aim of this study was to assess the maximum torsional strength of orthodontic mini-implants of different diameters.
Key Words: Mini-implants, anchorage, orthodontics. Introduction Anchorage is an issue of great relevance in the orthodontic planning. Crucial decisions are made depending on how orthodontic anchorage is delineated for a given treatment plan, that is: whether permanent teeth will be extracted, whether orthognathic surgery is needed, whether soft tissues are changed, whether the patient is cooperative, and whether the treatment will be simplified and shortened1. Literature in recent years has described several advantages from Dental Implantology such as mini-plates2-3, onplants4, conventional osseointegrated implants5-6 and miniimplants7- 9, all proved to be efficient as orthodontic anchorage. The use of mini-implants, however, has recently received great attention compared to other devices as a new concept of orthodontic anchorage because it is based on the absolute lack of movement of the anchorage unit due to orthodontic mechanics10. Similarly to the conventional dental implant systems, those practitioners inserting mini-implants should take special care both during the surgery itself and during the phase of orthodontic force application, since deformation or even fracture of such mini-implants is more likely to occur when inserting or removing them11-12. Mini-implants of reduced size provide greater variability in relation to the installation sites and decrease the risk of root damage13-14. On the other hand, mini-implants with reduced dimensions have less mechanical strength15, thus impending the application of maximum torsion force without causing deformation and fracture11,16. Based on such a supposition, the present work aimed at quantifying the maximum fracturing torque of orthodontic mini-implants of different diameters. Material and Methods A total of 18 commercially available orthodontic screwable mini-implants made from Ti6Al4V alloy and measuring 10 mm in length were allocated into three groups, according to their diameter: G1, G2 and G3 had miniimplants of 1.2, 1.4, and 1.6 mm in diameter, respectively. Mini-implants manufactured by SIN (Sistema de Implantes, São Paulo, SP, Brazil) were used in all groups. The mini-implants were mounted onto devices specially designed for this study according to Elias and Lopes15 . The torsional strength testing device consisted of a head containing a mandrel to hold the sample’s extremities, a hook to hold the opposite end of the mini-implant, and an axis from which a thread was attached to a battery cell (500 N) aimed to measure the force exerted on the miniimplants15 . Once the specimens were attached to the torsional strength testing device, a universal testing machine (Emic DL 10.000; Emic, Equipamentos e Sistemas Ltda.,São José dos Pinhais, PR, Brazil) was used running at a speed of 1 mm/s. The thread passing through the pulley system was pulled to rotate the mandrel so that the mini-implants were consequently twisted until they fracture. At this moment the maximum torsional strength exerted on the mini-implant was recorded by a software (Mtest program 1.01 version). The torsional strength test was carried out in the Laboratory of Biomaterials and Mechanical Assays of the Military Institute of Engineering (Rio de Janeiro, Brazil). The values of maximum fracture torques were analyzed by analysis of variance (ANOVA) and Tukey’s test at a level of significance of 0.5 %. Results Statistically significant differences (p<0.0001) in the torsional strength values were observed among the three groups (Table 1). Those mini-implants with greater diameter (Group 3) had the highest mean torsional values, whereas those with smaller diameter (Group 1) had the lowest ones (Figure 1). Discussion Size reduction and immediate load are required for optimising and simplifying the methodology of a rigid intra-osseous anchorage using mini-implants. The reduced diameter of the mini-implants provides greater variability in relation to insertion locals and decreases the risks of root lesion as well. However, such a reduced size also decreases the mechanical strength of the mini-implant, thus reducing the maximum torsional strength and resulting in deformation and fracture11. Mini-implants are more likely to break when osseous-integration occurs, since they have to be removed following orthodontic treatment16. As a result, new surgical procedures for removing or “entombing” the mini-implant are needed13 . When the maximum torque strength of a given material is to be assessed, one can use the mechanical torsional essay in which a force is applied on the samples or finished products in order to induce rotational movement around their strength centre15 . The objective of the present study was to assess the torsional strength of orthodontic mini-implants of different diameters. It was used the methodology proposed by Elias and Lopes15, who developed a specific device for mechanical torsional essays. Orthodontic mini-implants of different diameters produced by the same manufacturer were compared, it was found that their torsional strength values increased as their diameters also increased. This means that insertion torques for installing small diameter mini-implants into high-density bones is near the fracture torque, thus requiring more attention on the part of the practitioners. The clinical importance in determining the optimal torque for a given mini-implant is based on selecting specific screws for certain areas of the oral cavity, since they have different osseous density. This clinical finding is corroborated by Songa et al.14, who showed torque variations in both insertion and removal of several types of mini-implants for different bone densities. Despite being useful in certain situations (e.g. cases involving high-density bones), insertion torques should not be excessive. Motoyoshi et al.17 have demonstrated that increase in insertion torque of mini-implants is directly related to failure rates. The authors show a direct correlation between mini-implants successfully inserted and insertion torques ranging from 5 to 10 Ncm2 . Elias et al.11 have stated that the greater the diameter of a mini-implant the greater the insertion torque, since torque is proportional to the contact area between mini-implant and bone. Therefore, increased torque is necessary for larger areas. The results found in the present study meet satisfactorily the clinical needs as, according to Elias et al.11 insertion torque for high-density bones ranges from 12.6 to 23.2 N cm2 and for low-density bones ranges around 9.6 N cm2 . As can be seen, the values cited above are below the minimum ones found in the present study on fracture strength of mini-implants. The torsional strength essay for mini-implants has showed that fracture torque is relatively high compared to that used for mini-implants inserted in osseous substrates. Furthermore, the use of greater-diameter mini-implants provides safer conditions regarding fracture. References
© Copyright 2008 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os08019t1.jpg] [os08019f1.jpg] |
| |||||||||

{kind=link}
{kind=link}