 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
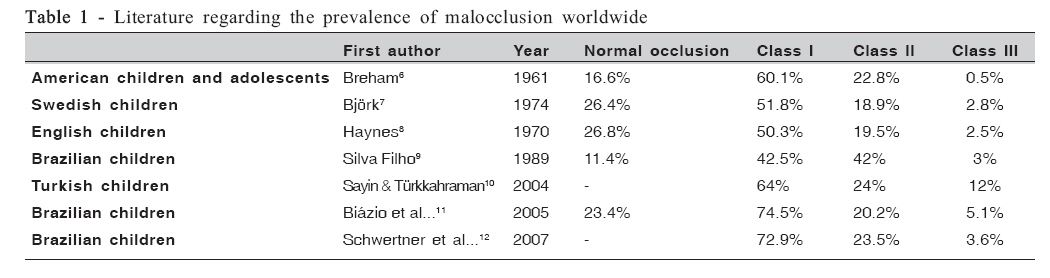
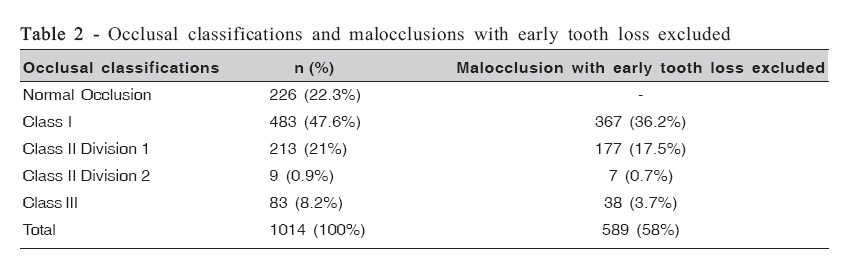
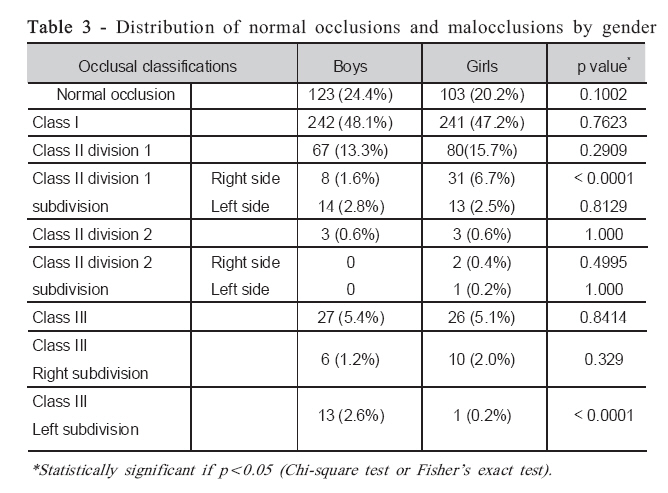
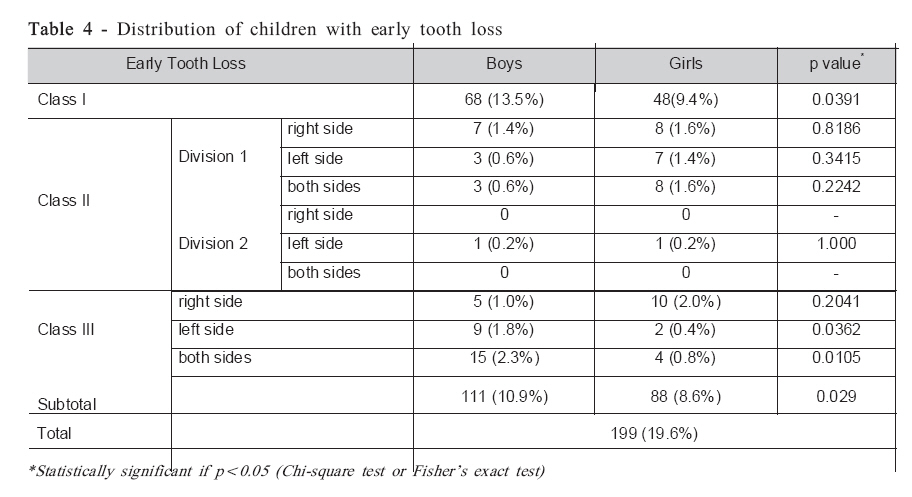
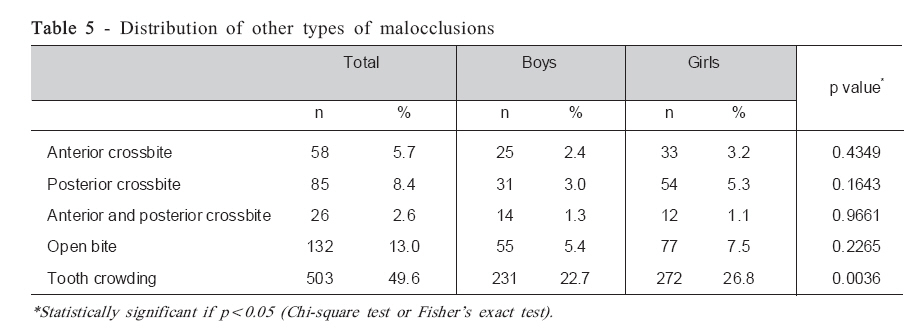
Brazilian Journal of Oral Sciences, Vol. 7, No. 25, Apr-Jun, 2007, pp. 1563-1565 Prevalence of malocclusion in a brazilian schoolchildren population and its relationship with early tooth loss Ricardo Alves de Souza1 ; Maria Beatriz Borges de Araújo Magnani2 ; Darcy Flávio Nouer2; Fábio Lourenço Romano3 ; Manuela Ribeiro Passos4 1DDS, MS, Assistant Professor, Department of Heath, State University of Bahia Southwest, Brazil Received for publication: September 23, 2007 Accepted: June 12, 2008 Code Number: os08020 Abstract The purpose of this study was to evaluate the prevalence of malocclusion in a Brazilian schoolchildren population in the mixed dentition, assessing its relationship with early tooth loss. The study population consisted of 1,014 7-11-year-old children of both genders, with low socioeconomic backgrounds and multiracial characteristics, living in the city of Jequié, in the Northeast region of Brazil. The clinical examination was carried out by an adequately calibrated orthodontist in the children’s classrooms. Data were analyzed statistically by either chi-square or Fisher’s exact test (a=0.05). Angle’s classification revealed that 22.3% of the population had normal occlusion. Class I malocclusion was observed in 47.6%, Class II division 1 in 21%, Class II division 2 in 0.9% and Class III in 8.2% of the children. Excluding the subjects (n=199) with early tooth loss, which is a condition that can modify malocclusion status, the distribution was as follows: Class I (36.2%), Class II division 1 (17.5%), Class II division 2 (0.7%) and Class III (3.7%). Early tooth loss was more commonly observed in boys (Class I, Class III left side, and both sides simultaneously). Anterior crossbite was observed in 5.7% of the subjects, posterior crossbite in 8.4%, anterior and posterior crossbite simultaneously in 2.6%, open bite in 13% and crowding in 49.6%. In conclusion, Class I malocclusion was the most prevalent alteration. The occlusal pattern of Class III was more common than Class II division 2, among the examined individuals. Key words: malocclusion, orthodontics, open bite, crossbite, tooth loss. Orthodontic care in Brazilian public dental services is still rare, probably due to the high treatment cost and the lack of specific public assistance policies. A systematic and well-organized dental care program for any target population in a community requires some basic information, such as the prevalence of the condition to be assessed1. Jequié is a city in the State of Bahia, in the Northeast region of Brazil, with a population from a low socioeconomic background. The population is mainly composed of biracial subjects with characteristics between white and black, which is a multiracial condition commonly observed in the State of Bahia. However, few epidemiological studies have been conducted with regard to the prevalence of malocclusion in this region. As socioeconomic factors interfere significantly with oral health, developing nations still have problems with children suffering from early tooth loss mostly due to caries2-4. This situation is directly related to malocclusion being an important factor for its establishment as well as for changing the malocclusion classification interpretation due to tooth migration. The Angle’s classification5 method has been widely used as a qualitative epidemiological tool for malocclusion assessment. Moreover, the prevalence of malocclusion has been extensively investigated worldwide6-12 (Table 1). The high prevalence of malocclusions implies that public health efforts are required, as such conditions affect negatively the individual’s quality of life, particularly in the case of children and adolescents, who are sensitive about their appearance13-18. A previous study with 395 Canadian children also found a high caries prevalence in primary teeth, reporting percentages of 30.4% and 20.6% for children aged 6 and 9 years, respectively19. An epidemiological study with 493 Nigerian children of different socioeconomic groups emphasized the need for treating crowded teeth (18.9%), carious lesions (14.8%), oral habits (7.3%), crossbite (10.3%), late primary tooth loss (6.9%), and early primary tooth loss (4.3%)20. The early loss of primary teeth can often result in malocclusion in a later moment21 involving the sagittal, vertical and transverse planes, thus becoming priority cases needing dental treatment22. Therefore, the purpose of this study was to evaluate the prevalence of malocclusion in a Brazilian schoolchildren population in the mixed dentition, assessing its relationship with early tooth loss. Material and Methods The study population consisted of 1,014 7-11-year-old children (mean age = 9.52 ± 1.16 years) of both genders, being 503 boys (49.6%) and 511 girls (50.4%), who lived in the city of Jequié, in the Northeast region of Brazil. The population presented low socioeconomic backgrounds and multiracial characteristics. Five public primary schools, representing different districts, were randomly selected from over 20 schools. After obtaining informed consent from their parents, and also approval from the school authority to conduct the study, one orthodontist (C.O.O.) examined the students clinically under natural illumination, using a sterile wooden spatula, mask and disposable gloves. Assessment of the anteroposterior relationship of the dental arches was based on Angle’s classification5. Other occlusal problems, such as anterior and posterior crossbite, open bite and tooth crowding were observed in this study. Data referring to early primary or permanent tooth loss, and patient identification, gender, age, address, and telephone number were also recorded by another dentist. In assessing the occlusal classification, the teeth were in maximal intercuspation, which was achieved by asking the subject to swallow and then to clench the teeth. Occlusions with minor deviations from the hypothetical concept of the ideal in permanent dentition, which did not cause esthetic or functional problems, were classified as normal. According to the 2003 Education census23, a total of 35,740 schoolchildren were attending local or state schools in the city of Jequié (excluding private and federal institutions), the great majority (n = 32,933) being public elementary schoolchildren. As a result, the sample selected for the present survey (n = 1,014) had a high reliability for epidemiological studies. Sampling error of 2.46% was calculated for the studied population with 95% confidence interval. Intraexaminer reliability, tested by re-examining 40 subjects after an interval of 2 to 4 weeks, was very high (r = 0.97; p<.001). The research protocol was independently reviewed and approved (process #066/2005) by the Human Ethics Research Committee of the Dental School of Piracicaba (FOP-UNICAMP). Statistical Analysis The data were submitted to statistical analysis by using either chi-square test or Fisher’s exact test for bivariate analysis at 5% significance level (p<0.05). Data analysis was performed using SPSS statistical software for Windows v.10.0 (SPSS Inc., Chicago, IL, USA), which also includes frequency distribution and test of association. Results Normal occlusion was found in 22.3% of subjects (Table 2). The prevalence of malocclusion changed when the individuals with tooth loss were excluded. In Class I and Class III individuals, malocclusion prevalence dropped from 47.6 to 36.2% and from 8.2 to 3.7%, respectively. As regards gender (Table 3), no statistically significant difference (p>0.05) was observed between boys (75.6%) and girls (79.8%) regarding malocclusion prevalence. Statistically significant difference (p<0.05) was observed in children with Class II division 1 right side subdivision (boys = 1.6% and girls = 6.7%) and Class III left subdivision (boys = 2.6% and girls = 0.2%) malocclusions. The distribution of early tooth loss (Table 4) was statistically different (p<0.05) comparing Class I (boys = 13.5% and girls = 9.4%), Class III left subdivision (boys = 1.8% and girls = 0.4%) and Class III both sides (boys = 2.3% and girls = 0.8%). Table 5 shows the distribution of other occlusal problems observed in the studied population. Anterior crossbite, posterior crossbite and open bite were found in 5.7, 8.4 and 13% of the subjects. Statically significant by gender was observed only for tooth crowding (p<0.05). Discussion The rate of normal occlusion observed in the present study (22.3%) differed from another study reported in the southern region of Brazil (11.47%)9. However, the normal occlusion score in Jequié was similar to that in Swedish (26.4%)7 and English children (26.8%)8. In African-American children, it has been reported that 17% of the children had normal occlusion24, while another study found a prevalence of 16.6% in white American children6 . There are several etiologic factors (e.g.: early tooth loss, oral habits) for malocclusions that modify all occlusal development. These factors are more important than the racial characteristics. In the present study, Class I malocclusion was found in 47.6% of the sample versus 55% found in a city of the Southern Brazil9. However, when the children with early tooth loss were excluded from the analysis, the percentage dropped to 36.2% in our study. Exclusion of individuals with early tooth loss from malocclusion prevalence studies has been considered as relevant for reducing significantly the number of children with Class I malocclusion. The findings of the present survey showed that early tooth loss interfered with malocclusion classification. Tooth migrations also changed the occlusal characteristics of the subjects in Class II Division 1, with a decrease from 21% to 17.5%, and in Class III malocclusion, from 8.2% to 3.7%. This finding does not agree with the results of a previous study involving 1,201 white Brazilian children aged 6 to 12 years, which reported a percentage of 43.4% and 1.2% for Class II and Class III malocclusions, respectively25. In Class II division 1, differences also occurred from other studies: Onyeaso1 (12.3%), Haynes8 (12.5%) and Foster and Day26 (27.2%). The methodologies and/or the characteristic of the samples could explain the differences. In this study, the prevalence of Class III with early loss tooth agrees with the rates reported by Foster and Day26 (3.5%), but presented differences from those reported by Haynes8 (2.5%) and Goose et al....27 (2.91%). In this study, there was a higher percentage of Class III malocclusions (3.7%) than Class II division 2 (0.7%). Onyeaso1 demonstrated a trend towards more Class III malocclusion in black children (11.8%), which seems to be related to the miscegenation of the schoolchildren in the Jequié sample. In order to evaluate the differences between ethnic groups and malocclusion prevalence, A previous study28 involving low-socioeconomic level black and white 8-9-year-old children was carried out in Pretoria, South Africa and found a significantly higher percentage of white children presented with Class II malocclusions, while black children showed a higher tendency for the Class III malocclusion. According with Table 4, early tooth loss in Class III left side was more significant for boys than girls (p=0.0362), which accounted for the significant differences in Class III subdivision left between genders in Table 3 (boys = 2.6% and girls = 0.2%). The tooth early loss in Class III on both sides elevated the severity of Class III (mandibular early loss). If the migrations occurred in the maxillary arch, the malocclusions were probably changed into Class I or Class II. The high differences in Class I (Table 2) promoted a significant value increase in the subtotal of early tooth loss (p=0.029); this condition would appear to be because of better oral hygiene care in girls than in boys. Early tooth loss should be taken into account for research as it is an important etiological agent with severe consequences for occlusion22. The differences between boys and girls in the Class II division 1 subdivision right and Class III subdivision left seemed to be due the early loss (Table 3). Several studies1,7-9 showed that no statistically significant sex differences were founded in the prevalence of malocclusions. Other occlusal problems (Table 5), such as anterior crossbite (5.7%) and open bite (13%) were in agreement with the previous data of Ramos et al....29, who observed that 6.7% of 218 children had anterior crossbite, and 15.4% of the sample presented open bite. However, differences were observed in the prevalence of posterior crossbite (8.4%), tooth crowding (49.6%) and early tooth loss (19.6%) compared to the results of another study29, which were 14.4%, 34% and 30.7% for posterior crossbite, tooth crowding and early tooth loss, respectively. A greater prevalence of crowding was observed in our study. The results of the present investigation demonstrated the importance of early tooth loss as an etiologic factor of malocclusions. Moreover, further studies involving multiracial populations are necessary in the Brazilian population, which requires increased attention from the public health system regarding dental assistance and preventive orthodontic care. Acknowledgements The authors would like to thank the Jequié authorities, particularly Dr. Tânia Diniz Correia Leite de Britto, Secretary of Health, and Dr. Domingos Sávio Perpétuo Coelho, Dentistry Coordinator, for the endeavor to create an inedited database on the prevalence of malocclusion in this city. References
© Copyright 2008 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os08020t4.jpg] [os08020t1.jpg] [os08020t5.jpg] [os08020t2.jpg] [os08020t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}