 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Effects of bonded rapid maxillary expansion appliance (brmea) in vertical and sagittal dimensions: a systematic review Moara De Rossi, DDS, MSc1; Renata Andréa Salviti de Sá Rocha, DDS, MSc1; Maria Beatriz Duarte Gavião, MD, PhD2 1PhD Student in Pediatric Dentistry Received for publication: March 07, 2008 Accepted: June 12, 2008 Code Number: os08021 Abstract Aim: The aim of this systematic review was to evaluate the existing literature about the effects of bonded rapid maxillary expansion appliance (BRMEA) on vertical and sagittal dimensions, and the possible advantages of its use. Key-words: Palatal expansion technique, cephalometry, orthodontics. Introduction Rapid maxillary expansion (RME) is a treatment modality for maxillary transverse discrepancy that was introduced by Angell in 18601. Since this time, different appliances have been developed to open the midpalatal suture, such as Hass-type, Hyrax-type and BRMEA (bonded rapid maxillary expansion appliance). While Haas and Hyrax appliances are banded to posterior teeth, the BRMEA is bonded to posterior teeth by a full acrylic surface coverage that encloses all occlusal surfaces. Regarding the maxillary and mandibular responses to RME, several studies2-7 have shown downward and forward maxilla displacement, dental extrusion, lateral rotation of the maxillary segments and cuspal interferences. These events lead to posterior rotation of mandible, open bite and increased vertical face dimension, which can be undesirable for patients with pronounced vertical facial growth patterns. BRMAs have been reported to help eliminating some of the extrusive effects of palatal expansion, due to the additional surface coverage, which limits unwanted tipping and rotation of teeth by increased rigidity8-9. However, there are contradictions in the literature concerning vertical and sagittal changes following RME performed with BRMEA. Therefore, the purpose of this systematic review is to evaluate the existing literature about the effects of BRMEA on vertical and sagittal dimensions, and the possible advantages of its use. Material and Methods This literature review consisted of a comprehensive search in the Medline (from 1966 to week 1 of March 2008), Pubmed (from 1966 to week 1 of March 2008) and Web of Science (from 1945 to week 1 of March 2008) electronic journal databases to retrieve English-language articles that referred to BRMEA. The inclusion criteria to initially select the abstracts were:
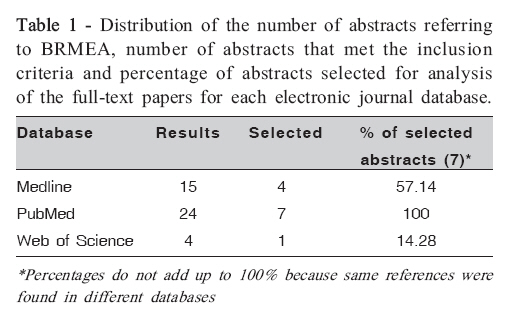
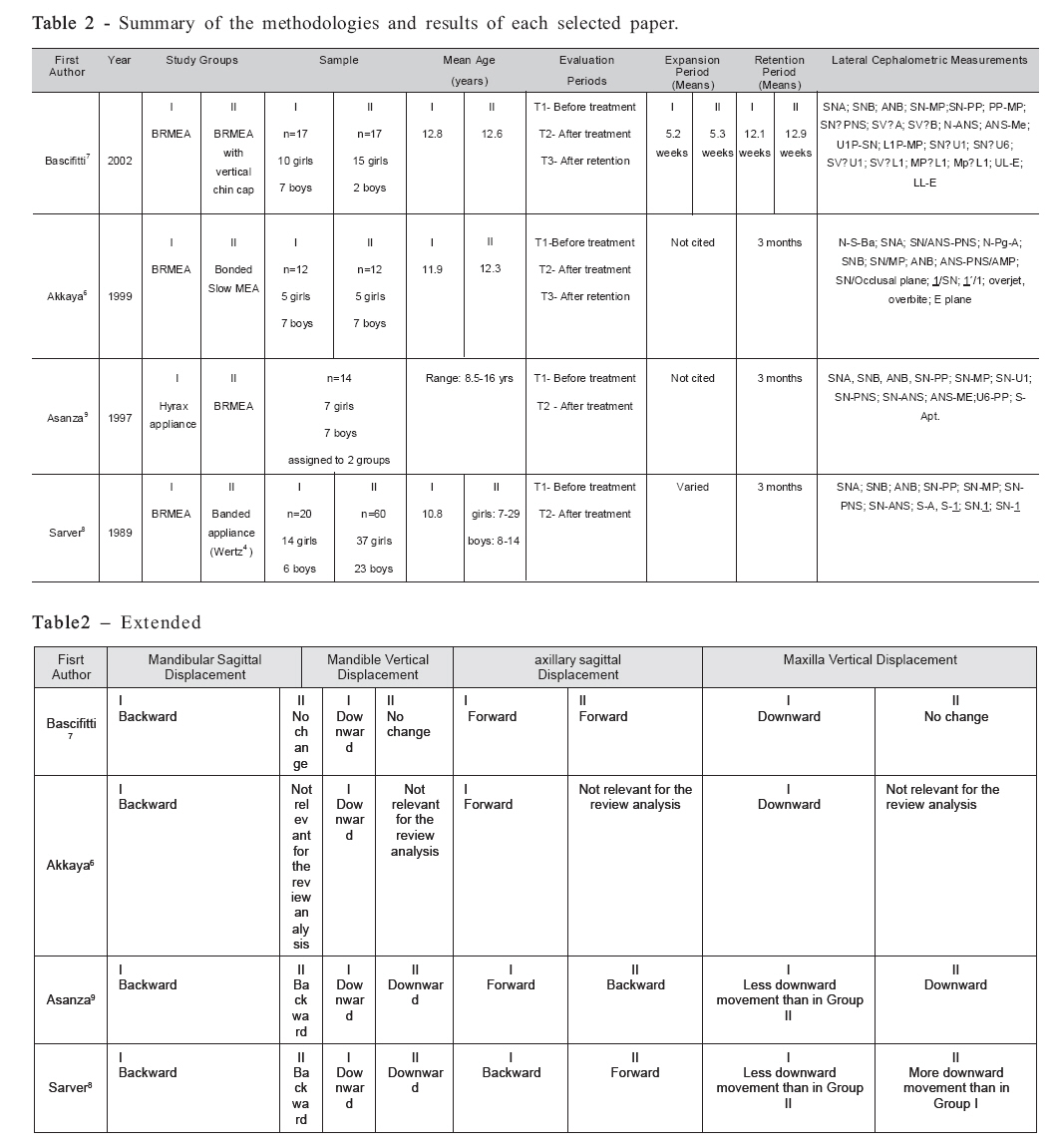
Results The distribution of the number of abstracts referring to BRMEA, number of abstracts that met the inclusion criteria and percentage of abstracts selected for analysis of the full-text papers for each electronic journal database is presented on Table 1. Four articles found in Web of Science were also found in Medline and Pubmed. Fifteen abstracts found in Medline were also found in Pubmed. Pubmed provided the largest number of selected abstracts. Three articles found in Pubmed were not found in the other databases. Only 7 out of 24 abstracts initially selected actually met the inclusion criteria. Four of them referred to studies that used other appliances associated with BRMEA7,10-12. After reading of the full-text articles, 17 of those 4 articles was maintained because it had a group of patients who wore only BRMEA. The other 3 articles10-12 were discarded after analysis because the subjects wore BRMEA and other appliances at the same time, and thus the obtained results could be attributed to the combination of the BRMEA with other therapies, such as edgewise orthodontics10,12, incisor intrusion11 and vertical pull chincup therapy11-12 . In the end, only 4 four articles remained6-9. The methodologies and results of each selected paper are summarized in Table 2. Discussion A critical review of the full-text articles a great heterogeneity in the methodologies regarding the evaluation periods, sample characteristics, such as age and gender, linear and angular cephalometric measurements. Sarver and Johnston8 reported the effects of BRMEA and compared their results to those of Wertz4, whio used a banded appliance. The anterior movement of the maxilla in the bonded sample was lower than that observed in the banded sample. According to the authors8, limited anterior movement of the maxilla with the BRMEA would be an indication for use in Class II patients. This study showed that there was lesser extrusion of the maxilla with the BRMEA and postulated that the thickness of the acrylic acts as a deterrent for extrusion. Asanza et al.9 also studied the difference between a banded appliance and the BRMEA and found anterior movement of the maxilla in Group I (Hyrax) and posterior displacement in group II (BRMEA). In Group I, the maxilla moved inferiorly with subsequent posterior and downward displacement of the mandible. The group treated with the BRMEA showed less inferior movement of the maxilla and a relative stability in the lower face height. These findings can be of importance in the treatment of patients with a long face, in which extrusion of the maxilla or the maxillary dentition would worsen the open bite situation and create more difficulty to treat vertical pattern8-9 . It is important to note that these two studies presented similarities in their methodologies8-9: the evaluation periods were “before treatment” and “after 3 months of retention period”, the appliances were similar, and 7 of the cephalometric measurements were the same in both studies. This could explain the similar results obtained in both articles. Akkaya et al.6 determined the vertical and sagittal effects of bonded rapid and slow maxillary expansion procedures, and compared these effects between the groups. Comparing these two treatment modalities is not the goal of the present review, but Akkaya’s et al.6 study clearly demonstrates the effects of treatment with BRMEA (Group I). The maxilla showed anterior displacement, and there was a posterior rotation of the mandible after use of BRMEA. Bascifitci and Karaman7 compared the effects of BRME therapy alone to those of BRME combined with vertical chin cap. In Group I (BRMEA only), the mandible rotated downward and backward and the lower anterior facial height increased. In Group II (BRMEA with vertical chin cap), the mandibular plane decreased, and vertical displacement of the maxilla occurred only in Group I, which is in agreement with the findings of Akkaya et al.6 but differ from those of Sarver and Johnston8. The long lower facial height moved anteriorly in both groups. The authors affirm that the use of vertical chin cap during and after RME is important to control the vertical dimension, especially in subjects exhibiting long lower facial height. Although the BRMEA has been shown to cause less vertical alterations than the banded appliances, some alterations were still present8-9. Downward movement of the maxilla, downward and backward rotation of the mandible using BRMEA alone were verified6,10. Bascifitti and Karaman9 showed a forward displacement of the maxilla. However, in Asanza’s et al.7, and Sarver and Johnston’s8 samples, some subjects exhibited a forward displacement of the maxilla, which can be seen by the SNA variation, that ranged from -5° to +1°, and from -3.6° to 1.7°, respectively. These differences may be attributed to changes in the sample characteristics to the distinct responses that each individual present to the treatments. The patient’s facial pattern is also an important issue to be considered and can interfere with the choice, response and prognosis of the whole orthopedic and orthodontic treatment. In all research articles retrieved for the present review, the subjects were enrolled without any consideration to their skeletal facial pattern. In this way, we believe that there is a need to study RME with BRMEA considering the patient’s facial patterns in order to determine whether this appliance is actually efficient to control the undesirable effects of RME in all situations. It has been reported that after RME therapy the maxilla will partially3 or completely4 return to its original position. Haas2 has stated that active facial sutures and bones force the maxilla to return to its original position. The tendency of the maxillary skeletal segments to return to their origin can also be attributed to accumulated forces in the circummaxillary articulations13, occlusal forces, surrounding buccal musculature14, and stretched fibers of the palatal mucosa15. Thus, the long-term changes can be of little, if any, clinical significance. The studies presented on this review6,7,9,12 showed that the vertical effects are only partially controlled with bonded devices. However, their observations were limited to the time of use of the BRMEA, including a 3-month stabilization period. This way, further studies should evaluate the dimensional changes occurring at longer periods after removable appliance retention. To the present, the orthodontist should be aware that BRMEA is an option for treatment of bilateral maxillary posterior deficiency, regardless of patient’s facial patterns. Based on this systematic review, it maybe concluded that: the BRMEA caused less downward and backward displacement of the mandible than the banded appliances, but these alterations were not completely absent; there is no consensus in the literature regarding the maxillary sagittal displacement after RME; there is not sufficient evidence to support the use of BRMEA to control the undesirable effects of RME. Acknowledgements This paper was prepared in the discipline “Advanced Pediatric Dentistry Issues” from the PhD program in Dentistry of the Dental School of Piracicaba, State University of Campinas. The authors acknowledge FAPESP ((Process 05/03472-4)and CNPq for the PhD scholarships granted to 1st and 2nd authors, respectively, and the Professors of the Department of Pediatric Dentistry, of the Dental School of Piracicaba, State University of Campinas, for their incentive. References
© Copyright 2008 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os08021t2.jpg] [os08021t1.jpg] |
| |||||||||

{kind=link}
{kind=link}