 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
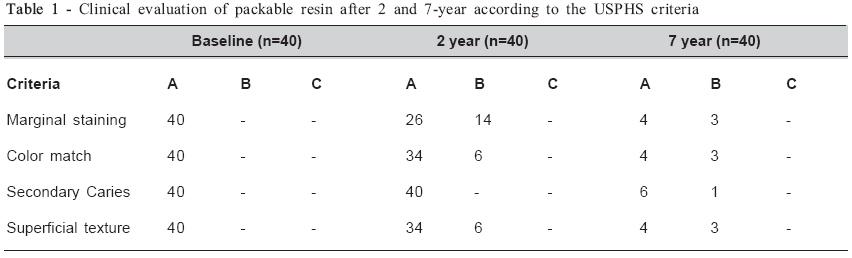
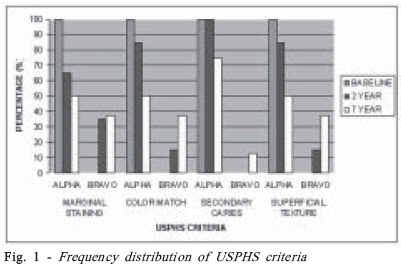
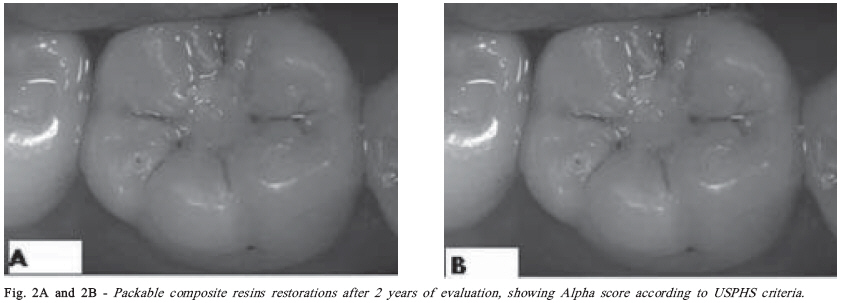
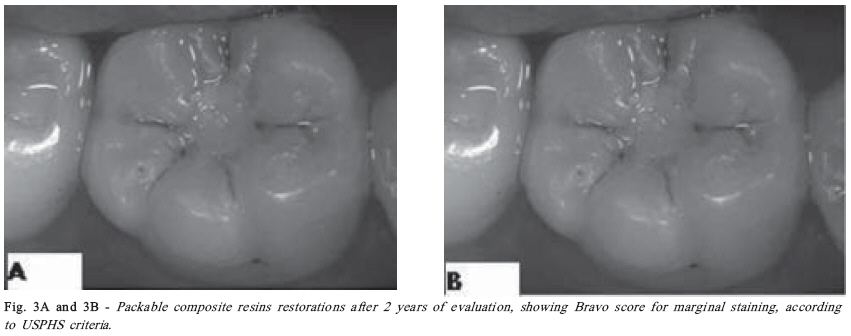
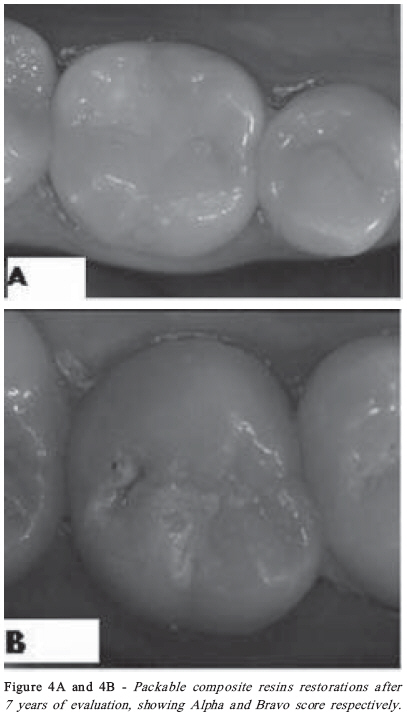
Brazilian Journal Oral Sciences, Vol. 7, No. 26, Jul/Sept, 2008, pp. 1585-1590 Clinical evaluation of packable resin Class I restorations after 7 years João Batista Novaes Junior1; Patrícia Valente Araújo2; Fernanda Damas3; Alfonso Gala-Garcia2; Maria Esperanza Cortés4 1DDS, MS, PhD, Associated Professor, Department of Clinic, Pathology and Surgery, CPC Received for publication: May 06, 2008 Accepted: September 09, 2008 Code Number: os08024 Abstract Aims: Compactable composite resins have been indicated as amalgam substitutes. However, longitudinal clinical trials are necessary to verify their wear resistance and integrity maintenance. The purpose of this study was to evaluate the clinical performance of a packable resin in Class I restorations after 7 years. Key words: Packable resin, USPHS criteria, clinical evaluation. Introduction In recent years, the placement of resin-based direct composite restorations has become a routine and wellestablished dental procedure. Despite the excellent longterm results obtained with amalgam restorations, speculation about the possible healthy risks associated with mercury and the demand for esthetic restorative materials have contributed to the increase use of composite resins in posterior applications. In addition, bonded restorations provide a more conservative cavity preparation by preserving valuable tooth structure1 . Composite resins were introduced in the 1970s, but their clinical use revealed serious problems such as excessive wear, leakage, secondary caries and postoperative sensitivity2 . Some modifications were done and with the improvement of the physical and chemical properties, the composite resins started being indicated for posterior teeth restorations. At the present moment, they are substantially superior to those produced years ago, even though secondary caries and wear resistance still continue being reasons for investigation. In face of these difficulties, changes in the handling In recent years, the placement of resin-based direct characteristics of composite resins have been made with composite restorations has become a routine and well-the aim of improving the composite placement, and several established dental procedure. Despite the excellent long-new products, called condensable or packable resin term results obtained with amalgam restorations, composite, were introduced to the dental market3. The speculation about the possible healthy risks associated packable resins present a linear thermal contraction with mercury and the demand for esthetic restorative coefficient of 1.8% and 80% of load percentage in volume. materials have contributed to the increase use of composite The particles occupy their space more efficiently and due resins in posterior applications. In addition, bonded to a greater percentage of loads, the volume of matrix is restorations provide a more conservative cavity reduced, resulting in a much smaller curing contraction preparation by preserving valuable tooth structure1 . and producing a superior marginal integrity than the Composite resins were introduced in the 1970s, but their conventional composite resins. The packable resins are clinical use revealed serious problems such as excessive indicated to recover areas of great masticatory efforts wear, leakage, secondary caries and postoperative because of their capacity to resist to the deformation and sensitivity2. Some modifications were done and with the because they have better viscoelasticity than the amalgam4 . improvement of the physical and chemical properties, the For some authors the wear resistance is similar to the one composite resins started being indicated for posterior teeth of the amalgam5-6. Nevertheless, when these materials were restorations. At the present moment, they are substantially compared with conventional resins, the chemical superior to those produced years ago, even though components were practically the same, only differing in secondary caries and wear resistance still continue being proportions7, and the mechanical properties did not present reasons for investigation. great differences8-9 . Although analysis of mechanical and physical properties provides valuable information, no in vitro method can totally subject the materials to the comprehensive and hard test conditions of the oral cavity. Ultimately, the clinical qualification can only be obtained in clinical studies3 . A clinical evaluation of restorative materials, by clinical observation, was described by Cvar and Ryge10 in 1971 and used in the method United State Public Health Service (USPHS). This method has been used in several studies in the evaluation of direct restorative materials, mainly for materials that would replace the amalgam restorations. The purposed evaluation made a longitudinal analysis of the restorative material, independent of other factors that could interfere with their clinical performance11 . The aim of this in vivo study was to evaluate the clinical performance of Classe I restorations restored with a packable resin, after 7 years, using the USPHS method. Material and Methods This study was approved by Research Ethics Committee of Federal University of Minas Gerais. Patients in treatment in the Primary Attention Clinic 1 and 2 of the Dental School of the Federal University of Minas Gerais were selected. Forty restorations were made in patients at ages ranging from 13 to 30 years. The clinical and radiographic diagnosis indicated the need of restoration of occlusal lesions. After a suitable disease control, including plaque control and sealing cavities to eliminate any microbial niche, the restorative treatment was executed. The packable resin used was Prodigy/OptiBond-KERR® . The restorations were done by following clinical steps: rubber dam isolation, removal of decay, preparation of the cavity and protection of the dentin-pulp complex. The specific operating steps of the material like acid conditioning, application of adhesive systems, material insertion and photopolymerization followed the manufacturer’s instructions. The restorations were made by the students supervised by the professors. The re-evaluations were made at baseline and after 2 and 7 years, by two calibrated operators. The criteria and codes used were those of method USPHS, as described below: Color match Alfa (A): No mismatch of color, shade and translucency between restoration and adjacent tooth Bravo(B): Slight mismatch of color shade and translucency, but within normal clinical limits Charlie (C): Mismatch of color and non-esthetic appearance. Unacceptable clinically. Marginal staining Alfa (A): No penetration of staining at the marginal interface Bravo (B): Penetration along the margin, but not in a pulpal direction Charlie (C): Penetration at the margin to the level of dentin or in a pulpal direction. Unacceptable clinically. Secondary caries: Alpha (A): No caries lesions present in the restoration margins; Bravo (B): Caries lesions present in the restoration margins, indicating change of the restoration. Superficial texture: Alpha (A): Smooth superficial texture similar to that of the enamel, as compared by the explorer; Bravo (B): Superficial texture slightly rougher than that of the enamel. Acceptable clinically; Charlie (C) Superficial texture moderately rougher than that of the enamel. Sandy surface texture, similar to that of chemically polymerized resins. Acceptable clinically; Delta (D): Rough surface in depth and extension stopping the sliding of the explorer in the surface in a continuous way. When disagreements arose during evaluations, consensus was reached between examiners. Because of the non-normal distribution observed by the Shapiro-Wilk test, the Mc Nemar test non parametric was performed at a significance level of á= 0.05. The analysis was performed with the data collected at baseline, 2-year and 7-year period. Results The results are summarized in Table 1. At baseline, the 40 restorations evaluated received Alpha score in all categories. All restorations were re-evaluated after 2 years, and an increase in marginal staining could be observed. No secondary caries was observed after 2 years (100% Alpha). Nevertheless, some restorations presented postoperative sensitivity and had to be replaced. After 7 years, only 8 restorations could be evaluated. One of them had been replaced by amalgam in the period between the evaluation of 2 and 7 years. There was no postoperative sensitivity in any of the restorations evaluated after 7 years, and only 1 presented secondary caries. All restorations evaluated in this study demonstrated acceptable clinical performance within the evaluation period based on the Alfa and Bravo ratings for clinically satisfactory restorations. Figure 1 shows the frequency distribution of the evaluated criteria. The Figure 2 and 3 show the restorations evaluated after 2 years, presenting Alpha and Bravo criteria and the Figure 4 shows restorations evaluated after 7 years. A statistically significant difference (p<0.05) was observed for marginal staining, surface texture and color match after 2 years follow-up and there was no significant difference (p>0.05) regarding secondary caries during this period. Although a statistically significant difference (p<0.05) could be observed for the above-mentioned criteria, all restorations were considered clinically acceptable, since this difference was attributed to variations between Alpha or Bravo criteria, both considered satisfactory from a clinical standpoint. Because of the low rate of patients evaluated after 7 years, statistical analysis was not possible. Discussion Resin-based composites have been increasingly used as restorative materials and the new brands have been marketed in the same rate. Thus, the greatest problem with clinical trials in the evaluation of posterior composite restorations is that the brands are constantly changed by manufacturers. However, clinical investigations with composite resins are important for predicting the longevity of current and future ones2-3 . Interest in clinical studies focuses on the reasons for clinical failures. While Collins et al.12 described the most common types of failures in composite resin restorations as bulk fractures and secondary caries, Burke et al.13 reported secondary caries as the most prevalent reason for replacement of restorations. In the present clinical study, secondary caries were not observed in any of the restorations after 2 years and in only 1 restoration after 7 years. A possible explanation for this good clinical performance is the fact that all restorations were done in conservative cavities with all margins in enamel, which probably contributed for the more effective sealing, reducing marginal infiltration. In addition, all patients were instructed about oral hygiene and the restorations were done after a suitable disease control, including plaque control and sealing cavities. The marginal seal is another important parameter to be considered in a clinical evaluation. Regarding marginal adaptation, a restoration could be considered clinically acceptable when no visible evidence of crevice along margin can be detected by explorer (Alpha score) or when the crevice is detected, but without exposure of the dentin or base (Bravo score). The Charlie score presents dentin or base exposed and in the Delta score the restoration is mobile or fractured. These last two scores are considered clinically unacceptable. Although in this study we did not include this criterion in the clinical evaluation using USPHS method, the lower percentage of secondary caries could indicate a good marginal adaptation. Moreover, during the follow-up investigation fractures were not observed. Other studies demonstrated a good marginal adaptation after clinical evaluation: in a 3-year evaluation, Loguercio et al.3 observed that only 10% of the restorations showed evidence of a slight crevice along the marginal interface (Bravo score). Burke et al.13 evaluated the packable resin Solitaireâ and found good results for marginal adaptation, when 88% of the restorations were considered Alpha or Bravo after a 2 years evaluation. Although almost all restorations were considered clinically acceptable in the evaluated period, being rated Alpha mostly and Bravo in some cases, important findings were noted and must be mentioned. The most affected criterion was the marginal staining, where 35% of the restorations received Bravo score after 2 years. This is consistent with findings of Lopes et al.2, who reported that the performance of the Prodigy Condensable/Optibond Solo® (KERR) after 2 years was different from that at baseline. This composite resin showed a significant increase in marginal staining2 . After 7 years, 37% of the evaluated restorations had Bravo score for marginal staining. According to Lopes et al.2 , this might be due to the patients, especially their habits, oral hygiene, and the extent to which they are influenced by external factors such as drinks, food, cigarettes and other things that possess stain elements. The alterations in surface texture can be attributed to many variables related to the inorganic filler of resin composites like size, hardness and amount of inorganic loading. The color match is thought to be involved with the organic matrix of resin composites. However, the interaction of these factors, should not be overlooked, as materials with a very rough surface will retain plaque and stains more easily, which can certainly contribute to color mismatch3 . This interaction could be noted in the present study, because in both evaluation periods, 2 and 7 years, all restorations that had Bravo score for surface texture, showed the same score for color mismatch. Changes in surface texture and color match could be used to indirectly measure the wear using the USPHS criteria13 . Prodigy® condensable resin (Kerr® ), by the use of rheological control additive (RCA) and a high filler loading (80% by weight), presents “packable” characteristics14. This material is characterized by a high filler load and a filler distribution giving them a stiffer consistency than hybrid composites. The preferential wear of the softer matrix over time may cause the protrusion of some high-sized particles. Bayne et al.15 suggested that the presence of these large particles may theoretically cause greater wear of the restorative material and the antagonist enamel. According to this author, the stress concentration through the filler particle and into the resin matrix when the restoration is under masticatory function will lead to the easy removal of these particles in the surface, exposing the organic matrix and accelerating the wear process even more. The good clinical performance observed after 7 years, where 50% of the restorations were scored Alpha and 37% Bravo for surface texture, could be attributed to the cavity size. The conservative outline form, preserving tooth structure, allows less occlusal contact on the restoration and reduces roughness and wear. Certainly, the more conservative cavity contributed for the maintenance of an adequate surface texture during the evaluated period. Over the years, composite resins with different formulations such as macrofilled, microfilled, hybrid, and “packable” resins were introduced into the dental market14. The average annual wear of several recent-generation posterior resins has been shown in laboratory and clinical studies to be equivalent to that of silver amalgam14. According to Lopes et al.14, the use of composite resins for the restoration of posterior teeth still presents other problems such as microleakage, postoperative sensitivity, secondary caries, and technical difficulties, although these problems have not been observed in the present study . It is important to observe that only 8 restorations could be evaluated after 7 years. The recall rate after 2 years was excellent, and all the restorations were re-evaluated. Therefore, after 7 years, some difficulties were found as the recall of patients was done. Firstly, it is important to mention that the Dental School changed its address between the 2- and 7-year evaluation and the new school is located very far from the old one. Consequently, many patients did not update their records and then could not be reached. Secondly, patients’ age was a problem. When they were first evaluated they were adolescents, with a more flexible schedule and after 7 years many had jobs and were therefore unable to attend the re-evaluations, since the class time at the university coincided with the working hour of the patients. The USPHS method has been used for most the clinical studies1-3,14,16 and this method was selected for this study to facilitate the comparison with other studies. According to this method, after 3 years of use, no more than 10% of the total of restorations can be classified as “Charlie” or unacceptable. Such values must be maintained for 5 years. No stipulation is made for the minimum percentage of restorations classified as “Bravo”. Long term evaluations have demonstrated little variation of criteria USPHS. A 7 year investigation on posterior composite restorations (n=70) using Z100® (3M), Clearfil Ray-Later® (Kuraray) or Prism TPH® (Dentsply) showed that 4 restorations failed due to the presence of secondary caries. No statistically significant difference was found between the materials when the color match, anatomic form and secondary caries were compared. Clearfil Ray-Later® (Kuraray) presented a rough surface texture different from the surrounding enamel, and it was statistically significantly different from the other materials evaluated. Z100 (3M) showed more marginal staining compared to other resins after 5 years. All materials had marginal adaptation problems after 7 years, but their clinical performance was acceptable17 . Yip et al.18 evaluated 57 Class I and 45 Class II composite resin restorations in permanent teeth, according to the USPHS method. The packable resin used was SureFil® , (Dentsply) and the conventional hybrid resin was Spectrum TPH® (Dentsply). Three SureFil® restorations failed before their initial evaluation. For both composite resins, the Alpha score for marginal staining was given in 90% of the restorations. A small percentage of restorations was classified as Alpha for color match, marginal integrity and gingival health. Occasional postoperative sensitivity was verified in 4 SureFil® and Spectrum TPH® restorations Both restorative materials had a satisfactory clinical performance after 1 year and no difference in the evaluated parameters was perceived. Regarding the evaluation period, few differences were detected and a failure rate of 6% was considered not significant in some studies19. These authors19 evaluated 47 restorations with SureFil® (Dentsply) after three years. In 31 restorations, no differences were observed regarding color match. Two restorations of the same patient were lost after 1 month and were rated as Charlie until the end of the study. After 3 years, only 5 restorations were classified as Bravo and 1 as Charlie for marginal staining. The score Bravo was found in 5 restorations for marginal adaptation, and in 3 restorations for anatomic form (p<0.05). According to the authors, the clinical performance of these Class II restorations was considered excellent. Based on the results obtained in this study, it may be concluded that the evaluated packable resins exhibited satisfactory clinical performance after 7 years with respect to color match, surface texture, marginal staining and secondary caries. Acknowledgments The authors thank to PRPq (Pró-Reitoria de Pesquisa da UFMG), which supported this project, and to Kerr® for supplying the material to be tested. References
© Copyright 2008 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os08024f4.jpg] [os08024f1.jpg] [os08024f2.jpg] [os08024f3.jpg] [os08024t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}