 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal Oral Sciences, Vol. 7, No. 26, Jul/Sept, 2008, pp. 1591-1595 Appraisal of oral lesions status of HIV/AIDS patients in South Western Uganda Ezera Agwu1; John Cletus Ihongbe2; Jackson Francis Tirwomwe3; Victoria Pazos4; Michael Tirwomwe5; Luis Casadesus6 1MSc, PhD, Student, Lecturer and Head, Department of Medical Microbiology Received for publication: May 12, 2008 Accepted: September 09, 2008 Code Number: os08025 Abstract Aim: To establish a regional surveillance data that may contribute to improvement of oral health prevention/control programs in South Western Uganda. Key words: Oral lesions, HIV/AIDS, Uganda Introduction Once infected with Human Immunodeficiency Virus (HIV), progression to Acquired Immunodeficiency Syndrome (AIDS) and death is the reality for most people in resource poor countries1. The impact of HIV on individuals and families in sub-Saharan Africa is still very great2 and therefore increasing research attention is being given to prevention, control and management HIV/AIDS victims3 . In Uganda, and most lowincome settings, the relationships of these parameters are far less clear, partly because of the scarcity of cohorts with complete laboratory testing and diagnostic capabilities4 . The oral cavity is an essential part of the body and
contributes to total health and well-being. It is evident
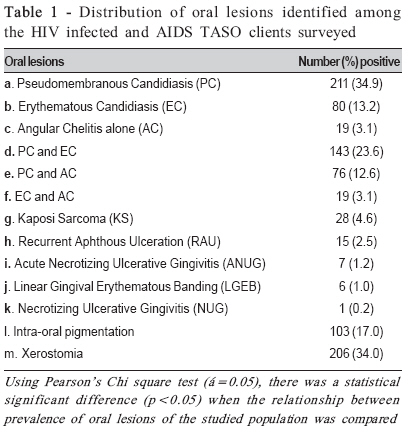
that poor oral health affects general health and that some Oral lesions correspond to the decline in numbers of CD4+ cells and an increase in viral load and are also independent indicators of disease progression7-8 . Bacteria are the predominant component of resident oral flora and its high species diversity reflects many endogenous derived nutrients and the varied types of habitat for colonization. The composition of the oral bacterial flora in disease and in health may not be different and any adverse changes resulting from immunosuppression predispose to infections9 . Conditions at the sites and compositions of oral microorganisms vary with respect to oxygen level, availability of nutrients and exposure to salivary secretions, immunosuppression, and oral hygiene10 . Despite many African reports on oral lesions associated with HIV/AIDS, similar reports from Uganda are highly limited10-11. In this study, we appraised the current status of oral lesions among HIV patients presenting to “The AIDS Support Organization-(TASO)” centers in South-West Uganda. The ultimate goal of this study is to obtain a regional surveillance data on oral lesions among HIV patients so as to determine the role of oral lesion surveillance in HIV prevention programs. This is expected to improve our existing diagnostic and management protocols of oral lesions among people living with HIV in this region. Materials and Methods Sample area, size and inclusion criteria Three main centers of The AIDS Support Organization “TASO”, located in three districts (Masaka, Rukunguri and Mbarara), and five outreach TASO centers (Katungu, Motoma, Kigarama, Ibwanda and Nyihanga), located in two districts (Bushenyi and Mbarara) all in South Western Uganda were used for this investigation. The inclusion criterion for TASO centers was based on center participation in a previews study12 in a similar cohort which revealed different kinds of oral manifestations of HIV/AIDS infection. The conditions for which patients were included in this study were that patients: must have tested positive to HIV using an Enzyme linked Immunosobent Assay (ELISA) and any other immuno-serological method; must have had his/her HIV/AIDS clinical staging done not earlier than one month prior to time of sample collection; must be a current TASO Client above 18 years of age Although 826 patients have consented to participate in this study, 605 were qualified. This was guided by the upper limit required to give 95% level of confidence at an expected prevalence of about 55%12 using the precise prevalence formula: Sample size (N) = Z2P (100-P)/D2 (Epi-info version 3.2 data-base; 1995), where Z is a constant given as (1.96), P is expected prevalence (55%), and D is acceptable error (5%). Informed consent was sought and obtained from the following: Uganda National Council of Science and Technology, Kampala International University Research and Ethics Committee, The AIDS Support Organizations (TASO) at both local and National level and TASO clients (patients) through their informed consent. Mouth examination and sample collection The diagnostic criterion for the oral lesion was according to World Health Organization’s established clinical criteria for HIV-associated oral lesions13. The mouth examination of the TASO clients was done by a previously trained and calibrated11 oral clinicians. The three oral clinicians included a dental surgeon, a clinical microbiologist and a public dental health officer. Prior to field survey, the three oral clinicians were standardized for consistencies in examination of oral lesions to minimize inter examiners variability using guidelines reported by Muwazi et al11 . Briefly, a gold standard (benchmark) examiner showed the examiners some photographic slides with clinical examples of classical oral lesions expected to be seen during the survey. This was done to determine the examiners’ ability to uniformly identify oral lesions with minimum inconsistency. The clients were examined in a room with a natural light while seated on an office chair and facing the window. The mouth was examined using natural light and a mouth mirror. A disposable wooden tongue depressor was used to retract the cheeks. Some clinical photographs of classical examples of the lesions were taken using digital camera. Results The overall prevalence of individuals with oral lesions was 73.2%, occurring both as single and double manifestations, as showed in Table 1. Pseudomembranous candidiasis (PC) showed the highest overall prevalence of 71.1% (34.9% single and 36.2% mixed oral manifestations), followed by 39.9% prevalence of Erythematous Candidiasis (EC), (13.2% single and 26.7% mixed oral manifestations); 18.8% prevalence of Angular Chelitis (AC) (3.1% was single and 15.7% was mixed oral manifestations). Out of 605 oral manifestations diagnosed from single and mixed infections, 143 (23.6%) were PC and EC; 76 (12.6%) were PC and AC and 19 (3.1%) were EC and AC. Other oral lesions also observed in this study included: 4.6% Kaposi Sarcoma (KS); 2.5% Recurrent Aphthous Ulceration (RAU); 1.2% Acute Necrotizing Ulcerative Gingivitis (ANUG); 1.0% Linear Gingival Erythematous Banding (LGEB); and 0.2% Necrotizing Ulcerative Gingivitis (NUG). Intra-oral pigmentation was 103 (17.0%) prevalent among the studied population. Using Pearson’s Chi square test of independence (X2; á=0.05, 0.01), there was a statistical significant difference (p<0.05; 0.01) when the relationship between prevalences of oral lesions of the studied population were compared. Out of the 605 patients diagnosed with oral lesions, the result of pre-exposure of patients to antimicrobial agents was as follows: Clotrimazole 44 (7.3%); Fluconazole 27 (4.5%); Ketoconazole 62 (10.2%); Nystatine 68 (11.2%); Anti-retroviral agent (unspecified) 48 (7.9%) and patients not exposed to anti-fungal/viral agents 356 (58.8%). There was a significant statistical difference (p<0.01) when Chi square (X2; á=0.01) was used to test for independence of the different antimicrobial agents used. Discussion In resource poor countries, sporadic prevalence reports with no longitudinal cohort studies have made oral lesions an increasing concern, mainly in immunocompromised patients14. The observed 73.2% prevalence of oral lesions among the consenting population of HIV infected and AIDS TASO patients, is in line with the 30-80% oral lesions among HIV/AIDS patients in developing countries, reported by Arendiof et al.5 and Patton et al.15, as well as with a survey conducted on a subset of TASO clients in the same region in the year 200512. Moreover, Tirwomwe et al.12 found similar prevalence of oral lesions, meaning that HIV/ AIDS patients benefiting from TASO services need essential oral health care. In this region more effort is therefore required to reduce the current prevalence of oral lesions among TASO patients and other HIV patients to the barest minimum. On the other hand, the found prevalence in the present study was different from a former survey in a rural Uganda community, which showed 42% manifestation of oral lesions16, probably due to the inclusion of non HIV/ AIDS individuals. Latiff et al.17 reported a prevalence of 75% in India and a higher prevalence, 90%, was found by Fidel18 in the Wester18 . Lower result should have been expected from India and the Western because of expected increased support from government and donor agencies and better strategies for management and control of this infection. Umedevi et al. 19 in Johannesburg, South Africa, found significant differences in the occurrence of oral lesions between HIV-positive and -negative women, thus highlights the usefulness of oral lesions in the detection of early and unknown HIV infections. The wide range of oral manifestation (Table 1), from 0.1% (NUG) to 71.1% (PC), is slightly lower than reports in South Africa7 and the United States20 (1.5 % to 94%). Slightly lower range of oral manifestation observed in Uganda TASO HIV population points to a positive impact of TASO services to the people living with HIV in Uganda. Hodgson et al.8 had considered that the wide range found in African studies could be due to the improper calibration in methodologies. Lack of adequate resources to warrant in-depth qualitative laboratory study so as to confidently and more accurately formation of lesion groups, as recommended by E-C Clearinghouse17, may be a contributing factor for the wide range in prevalence of different oral lesions found in African studies. Meanwhile, it is interesting to note that the 17.0% prevalence of unique IOP found in this study is lower than the 26.3% reported in South Indian HIV population21 . In documenting the population with oral pigmentation seen after HIV infection, 48 (7.9%) patients with oral lesions and who were taking unspecified antiretroviral therapy, including those who possessed oral pigmentation from birth, were excluded. Having ruled out possible racial melanination by hereditary and pigmentation due to side effect of antiretroviral therapy, the next most probable cause of oral pigmentation among the patients studied could be increased release of α-melanocyte stimulating hormone (α-MSH) due to deregulated release of cytokines in HIV disease and less likely due to use of antifungals21- 22. This observation warrants further investigation so as to hypothesize that HIV disease is more likely to cause oral pigmentation in Indians than in Africans. The observation of 40.9% mixed infection of PC with other oral lesions (PC with EC: 29.3% and PC with AC: 11.6%; Table 1) gives this study another unique importance because such finding is rare in many African studies. There was a statistical significant difference (p<0.05 and p<0.01) when the relationship between prevalence of different oral lesions identified among the studied population were compared. This implies that the interaction of different oral lesions noted in this study was due to other factors (such as change in CD4 level and viral load) and not by chance alone. Therefore, in addition to the reported possible correlation of single or grouped oral lesions to CD4 cell levels23, we hereby suggest that CD4 cell levels could also be correlated with the levels of mixed manifestations of oral lesions in severely immunosuppressed patients. Thus the level of mixed oral infection may herald emergence and progression of HIV disease. Despite the fact that the critical immunological defects, which are responsible for the onset and maintenance of mucosal candidiasis in patients with HIV infection, has not been elucidated, the devastating impact of HIV infection on mucosal Langerhans’ cell and CD4+ cell populations may most probably be central to the pathogenesis of mucosal candidiasis in HIV-infected patients24. However, these defects may be partly compensated by preserved host defense mechanisms (calprotectin, keratinocytes, CD8+ T cells, and phagocytes), which individually or together, may limit Candida albicans proliferation to the superficial mucosa25 . A close comparison with a Tirwomwe et al.12 study reveals minor improvement in some lesions and worsening condition in other ones. Oral hairy leukoplakia which was 0.3%12 was not seen in the present study. LGEB was reduced by 6.8% (7.8%: 1.0%), while Kaposi sarcoma was reduced by 0.2% (4.8%: 4.6%) in the present study. The slight reduction in the relative prevalence of oral lesions, two years after the lesions were identified and recommendations made on the need to follow improved management protocols, shows that the goal of improvement of oral health condition among people living with HIV in Uganda may be achievable. Therefore, more efforts should be made to increase the reduction rate of these oral lesions observed among the people with HIV in Uganda. On the other hand, the incidence of PC among HIV patients diagnosed with oral lesions increased by 30.7% (40.8%: 71.1%), Angular Chelitis increased by 1.2% (17.6%: 18.8%), EC increased by 1.0% (38.9%: 39.9) and NUG was increased by 0.9% (0.3%: 1.2%) respectively. Information obtained from this study (Table 1) shows that from 71.1% individuals with PC, 58.8% were not taking any antifungal and antiviral therapy, whereas 11.2% were taking Nystatine at the time of this investigation. Furthermore, from the 39.9% individuals with EC, about 35% were not taking any antifungal and antiviral therapy while 4.9% were on Azoles. Finally, from 18.8% patients with AC, 7.9% were on unspecified anti-retroviral therapy and 10.9% were on azoles antifungals. Therefore, observed increase in the relative prevalence of Candidiasis in this study may be due to antifungal resistance and inadequate treatment. Proper oral care of patients especially in remote villages where TASO render their services once in a month or two were clearly lacking. This is because TASO services do not include routine oral inspection and care of their HIV/AIDS patients. Inclusion of trained Dental officers among TASO healthcare team is hereby recommended. This recommendation is paramount to the overall effort in reduction of oral infection among people living with HIV in Uganda and other developing resource poor countries. In conclusion, oral infections are still highly prevalent among HIV/AIDS patients in South Western Uganda. Inadequate provision of antimicrobial agents and absence of oral and dental care were suggested to have contributed to upsurge of oral infections among TASO patients in this region. Increasing prevalence of oral candidiasis among HIV/ AIDS patients stresses the fact that HIV/AIDS is still a terminal disease especially among people living in resource poor countries. Provision of adequate resources and qualified personnel to warrant in-depth clinical and qualitative laboratory study is supreme to achieving the goal of overall improvement of oral health condition of these patients. There is an urgent need to train primary health care workers in management of oral lesions associated with HIV/AIDS. More studies are needed to evaluate oral lesions and to assist health care providers in the early detection of HIV/AIDS in the studied population. Acknowledgement This study was supported in part by Kampala International University, Western Campus. We are grateful to management and staff of The AIDS Support Organization both at the Headquarters in Kampala and in the three centers located in South Western Uganda for their support. We also thank all TASO clients whose consent and participation made this investigation possible. References
© Copyright 2008 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os08025t1.jpg] |
| |||||||||

{kind=link}