 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
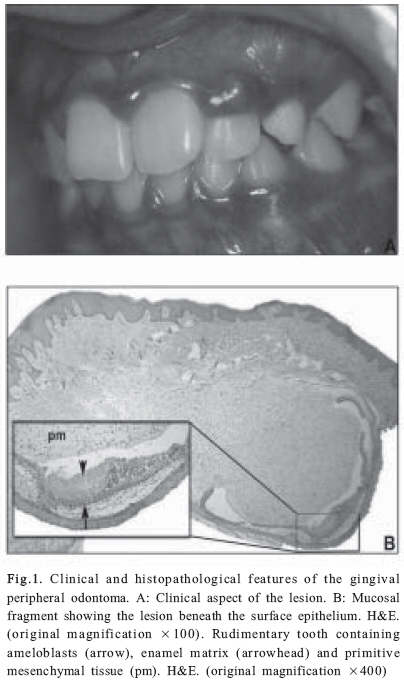
Brazilian Journal Oral Sciences, Vol. 7, No. 26, Jul/Sept, 2008, pp. 1624-1626 Gingival peripheral odontoma in a child: case report of an uncommon lesion Vanessa de Fátima Bernardes1; Luis Otávio de Miranda Cota1; Fernando de Oliveira Costa2; Ricardo Alves Mesquita2; Ricardo Santiago Gomez2; Maria Cássia Ferreira Aguiar2 1DDS, MS, Graduate student, Department of Oral Surgery and Pathology, School of Dentistry, Federal University of Minas Gerais, Brazil 2DDS, MS, PhD, Adjunct Professor, Department of Oral Surgery and Pathology, School of Dentistry, Federal University of Minas Gerais, Brazil Received for publication: July 30, 2008 Accepted: September 09, 2008 Code Number: os08031 Abstract Odontoma in an extraosseous location represents a challenge for diagnosis. This article reports a case of peripheral odontoma and its clinical presentation, histological evaluation and treatment. A 12-year-old boy reported a firm asymptomatic gingival mass in the anterior maxilla with two years of evolution. The procedures for diagnosis included intraoral examination, excisional biopsy and histological analysis. The diagnosis was peripheral odontoma. The follow-up revealed no sign of recurrence. Peripheral odontoma is rare and the differential diagnosis with other gingival masses is rather difficult and must include inflammatory and reactive processes. The definitive diagnosis is based on microscopic features. Key Words: Extraosseous odontoma, diagnosis, gingival lesion. Introduction Odontomas are considered hamartomatous malformations of odontogenic origin in which all dental tissues are represented, occurring in a more or less disorderly pattern1 . These lesions are usually diagnosed in the second decade of life and have no predilection for sex2 . The intraosseous (central) odontomas represent the odontogenic tumors of greatest incidence3. Otherwise, odontomas arising in the extraosseous soft tissue, also known as peripheral odontoma (POs), are extremely uncommon4. PO shows the histological characteristics of an intraosseous odontoma, but occurs only in the soft tissue covering the tooth-bearing portion of the mandible4. To the best of our knowledge only eight cases have been previously reported2,5-10. This article presents a case of PO in a child referred to our Dental Clinic for treatment. Case Report A 12-year-old white boy was referred to Dental Clinic of the School of Dentistry, Federal University of Minas Gerais, with a single, asymptomatic nodule on the gingiva in the region of the left lateral incisor. The patient reported that the mass had a slow growth and two years of evolution. Physical and intraoral examination showed a healthy boy with a slightly reddish, circumscribed, firm 4-mm-diameter nodule. The overlying gingiva had normal texture (Figure 1A). Neither signs nor history of trauma or infection were detected. Teeth were visually free of caries and adjacent tissues were clinically normal. The hypotheses of diagnosis included pyogenic granuloma, periodontal abscess, and peripheral ossifying fibroma, and an excisional biopsy was performed for confirmation. No bone involvement was observed during the surgery. The specimen was immediately placed in 10% neutral buffered formalin, processed in the usual manner and submitted for histopathological analysis. Histologically, a developing rudimentary tooth was observed in the submucosal tissue. Enamel matrix, dentin, pulp tissue and ameloblasts were present (Figure 1B). Ghost cells were also noted (not shown). The lesion was completely separated from the overlying epithelium by a capsule composed of connective tissue with fibroblasts, blood vessels and islands of odontogenic epithelium. On the basis of the clinical and histopathological findings, the lesion was diagnosed as a developing peripheral compound odontoma. The two-week postoperative follow-up showed that the area had already healed. Two years later, there is still no clinical sign of recurrence. Discussion Two types of odontoma are histologically recognized: compound and complex lesions. The compound lesion is comprised of tooth-like structures while the complex lesion is comprised of a mixture of odontogenic tissues without dental organization2. Clinically, three types of odontoma are described in literature: central (intraosseous), erupted, and peripheral odontoma (extraosseous or soft tissue)6 . Intraosseous odontomas represent the most common type. These extraosseous lesions are quite rare and the reports in the literature are limited7. The lesions are usually diagnosed between the first and the second decade of life but may be found at any age. The most common location for this type of lesion is the maxillary anterior region8 , and most odontomas are relatively small, rarely exceeding 1 cm in diameter9 . Histological examination shows rudimentary denticles or tooth-like structures and epithelial elements may be absent10. In the present case, the relationship among the structures suggested a compound odontoma. The presence of ghost cells, as noted in this case, is not a pathognomonic sign. It has been described in odontoma as well as in other lesions, such as calcifying odontogenic cyst, ameloblastoma, ameloblastic fibroma and ameloblastic fibroodontoma11-13. The radiographic examination may show three different developmental stages based on the amount of calcification present at the time of discovery. Unfortunately, no radiographic exam was performed in this case. The histogenesis of PO is controversial. POs are speculated to arise from the soft tissue remnants of the dental lamina. Gingival rests of Serres seems to retain the ability to pursue necessary epithelial-mesenchymal interactions, thus leading to an odontoma formation10. The specific etiological factors responsible for their development have not been determined. Theories have included physical trauma, infection and hereditary influence5,9. PO occurs in gingival tissue, appearing as an exophytic mass that can be mistakenly diagnosed as other more common exophytic gingival lesions. The differential diagnosis includes lesions of inflammatory origin (e.g., periodontal abscess) and reactive proliferations (e.g., pyogenic granuloma, peripheral ossifying fibroma, peripheral giant cell granuloma)2,5,8. Because of their rarity, peripheral odontogenic tumors are usually not included in differential diagnosis. When considered, the first suggestion is the peripheral odontogenic fibroma. Peripheral ameloblastoma, peripheral calcifying odontogenic cyst and peripheral calcifying epithelial odontogenic tumor can also be suspected. However, they are extremely rare and usually occur in the third and sixth decade of life5,12. Since these lesions are considered hamartomatous with a very limited growth potential, surgical removal should be conservative with no real expectation of recurrence10. The histological examination is mandatory for an accurate diagnosis9. In the present case, two years of follow-up indicate no sign of recurrence. Acknowledgements The authors thank the Brazilian National Council for Scientific and Technological Development (CNPq) and the The Minas Gerais State Research Support Foundation (FAPEMIG) for assistance and financial support. Mesquita RA, Gomez RS, and Aguiar MCF are research fellows of the CNPq. References
© Copyright 2008 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os08031f1.jpg] |
| |||||||||

{kind=link}