 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
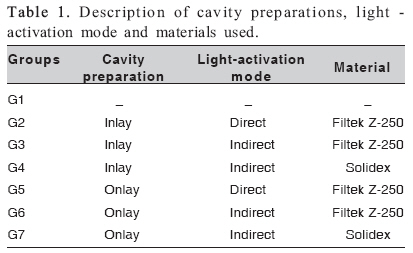
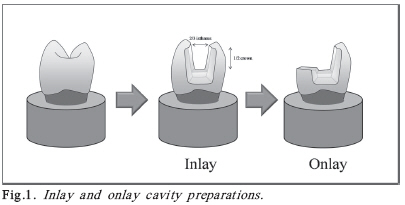
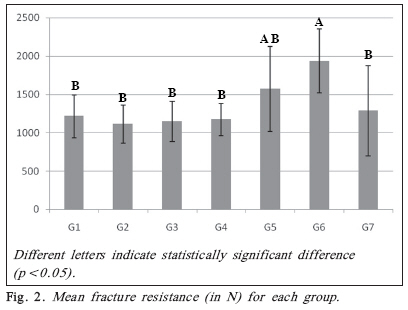
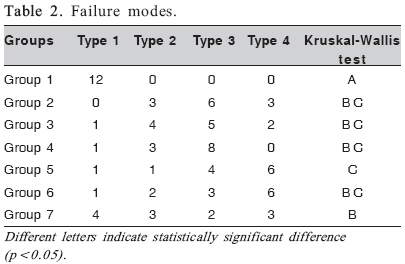
Brazilian Journal Oral Sciences, Vol. 7, No. 27, Oct/Dec, 2008, pp. 1636-1640 Effect of cavity preparation design on the fracture resistance of directly and indirectly restored premolars Denise Sá Maia Casselli1 ; André Luis Faria e Silva2 ; Henrique Casselli3; Luis Roberto Marcondes Martins4 1DDS, MSc, PhD Professor, Department of Dentistry, São Leopoldo Mandic Dental School-Unit Ceará Fortaleza, Ceará Brazil. Received for publication: April 01, 2008 Accepted: September 09, 2008 Code Number: os08035 Abstract Aim: The aim of this study was to evaluate the fracture resistance of human premolars with extensive cavity preparations of the inlay and onlay types, for performing direct and indirect composite resin restorations. Key Words: composite resin, fracture resistance, cavity preparation, restorative technique, indirect restoration. Introduction Sound teeth rarely fracture during normal masticatory stress1 . The presence of the palatal and buccal cusps with intact mesial and distal ridges forms a continuous circle of dental structure, reinforcing and maintaining tooth integrity. However, cuspal fracture can frequently occur in teeth that have been weakened by caries, large cavity preparations and reduction of dental structure as a result of erosion or abrasion2 . Studies have shown that teeth with cavity preparations become weaker as the occlusal isthmus is widened, and they fracture more easily than intact teeth2,3 . Therefore, it is important to preserve the integrity of the dental structure to maintain its resistance2-4 . Recently, there has been increasing use and acceptance of the acid-etch technique to bond various materials to tooth substrate3-5 . With the introduction of dental composites and the development of adhesive systems, it was possible to reduce significantly the amount of healthy dental tissue removed during cavity preparation. This has enabled more esthetic restorations to be performed and to reestablish the fracture strength lost due to cavity preparation. Composite materials potentially have many applications, such as anterior and posterior restorations, indirect inlay/ onlays and pit-and-fissure sealants4,6 . One of the main drawbacks of current composites is the shrinkage during polymerization, which creates stress on the restored tooth and may result in poor marginal integrity, as well as inadequate durability and longevity in the oral environment7 . Furthermore, it is difficult to obtain proximal contacts, and anatomic reproduction, finishing and polishing are limited in more complex clinical situations. In order to overcome these limitations, the choice for indirect restorations with laboratory-processed resins is a feasible option. The composite resin Solidex (Shofu, Kyoto, Japan) is an example of intermediate laboratory-processed resin that is polymerized by light-curing unit of xenon stroboscopic light. This high-intensity light source with intermittent pulses has been reported to improve hardness, compressive strength and flexural strength, and to reduce water absorption and water solubility of composite materials8 . Despite these advantages, indirect composite resins are approximately twice more expensive than direct composite resins. Recently, Casselli et al.8 demonstrated that the direct composite resin Filtek Z-250 (3M/ESPE, St. Paul, MN, USA) presented better diametral tensile strength than the indirect composite resin Solidex. In addition, this mechanical property was improved when the composite resin was heat light-polymerized using an EDG-lux high-intensity xenon photo-curing unit (EDG, São Carlos, SP, Brazil). Therefore, the aim of this study was to evaluate the fracture resistance of human premolars with extensive inlay and onlay cavity preparations, restored with indirect and direct composite resins. The direct composite was used both directly and indirectly. The null hypothesis was that the material, the restorative technique and the type of cavity preparation would not interfere with the fracture resistance. Material and Methods Eighty-four human, single-root maxillary premolars, unrestored, non-carious, free of cracks and defects, extracted due to periodontal or orthodontic reasons and stored in 10% formalin solution (pH = 7) for up 3 months, were used in this study. Teeth with similar size and shapes were selected by crown dimensions after measuring the buccolingual and mesiodistal widths, allowing a maximum deviation of 10% from the determined mean. After cleaning with periodontal curettes, the teeth were mounted in polystyrene resin cylinders, with simulated periodontal ligament, exposing 2 mm of root surface below the cementoenamel junction9 . To simulate the periodontal ligament, a radiographic film with a centralized circular hole was used to stabilize the teeth during the inclusion procedure. First, the root was covered with wax and then a 25-mm-diameter plastic cylinder was placed over the root. The polystyrene resin was inserted into the cylinder and, after polymerization, the tooth was removed from the resin and the wax removed from the root. The resin cylinders were filled with a polyether material (Impregum F; 3M/ESPE) and the teeth were reinserted and the excess polyether material was removed. The teeth were randomly assigned to seven experimental groups, according to Table 1. Tooth preparations were made with a standardized preparation machine, which consists of a high-speed handpiece (Kavo do Brasil, Joinvile, SC, Brazil) coupled to a mobile base that moves vertically and horizontally. This movement is controlled with aid of a micrometer (Mitutoyo, Tokyo, Japan), accurate to 0.1 mm. A tapered cylinder diamond bur # 4137 (KG Sorensen, Barueri, SP, Brazil) was used under water cooling for the cavity preparation. The isthmus width was 2/3 of the distance between the cusp tips, and the pulpal depth was ½ the crown height (Figure 1). Cavity width was checked in the occlusal portion and the pulpal depth was measured with a digital caliper in relation to the buccal cusp tip. The cavities were finished with the same diamond bur in a low-speed handpiece. This preparation was classified as inlay. For direct restorations, each cavity was etched with 35% phosphoric acid (Scotchbond etchant; 3M/ESPE) for 15 s, washed with an air-water spray and dried with absorbent paper. Two consecutives layers of the adhesive system Single Bond (3M/ESPE) were applied and light cured for 20 s (Degulux, Degussa Hülz, Frankfurt, Germany) after solvent evaporation with an air stream. The composite resin Filtek Z-250 was inserted in 2-mm thick increments and polymerized for 40 s with the same halogen light-curing unit. For indirect restorations, impressions were made of the prepared teeth using a polyvinyl siloxane impression material (Aquasil, Dentsply De Trey, Konstanz, Germany) in a 2-step technique, and the impressions were poured with a type IV stone (Durone, Dentsply, Petrópolis, RJ, Brazil) after 30 min. The cavity dimensions of the onlay preparation were similar to those of the inlay preparation, with additional removal of the palatal cusp. The impressions of this preparation were also made in the same manner as described before. The restorations were made with Z-250 or Solidex composite resin inserted in approximately 2mm-thick increments on the isolated stone die. Each increment was heat light polymerized for 2 min using the EDG-lux unit. After 24 h, the internal surface of the indirect composite resin restorations was airborne-particle abraded with 50μm aluminum oxide for 10 s, washed with an air-water spray for 60 s, air-dried and coated with a layer of the the silane agent (Ceramic Primer, 3M/ESPE) for 60 s. Next, Single Bond adhesive system was applied and light cured for 20 s. The same adhesive procedure described for direct restorations was used for these teeth. The indirect restorations were cemented with a dual-cured resin-based cement (RelyX ARC; 3M/ESPE), which was light cured for 40 s from each side of the restoration. The specimens were stored in 100% relative humidity at 37°C for 24 h. After this period, the specimens were submitted to compressive load in a Universal Testing machine (Instron 4411; Instron Corp, Canton, England) with a 6-mm-diameter steel sphere at a crosshead speed of 0.5 mm/min until fracture. The sphere came into contact with the dental structure and restorations on both buccal and lingual cusps The data were converted into N and submitted to one-way ANOVA using a 95% level of significance. The fractured specimens were analyzed under a stereomicroscope to determine the failure modes, and were assigned to 1 of 4 categories, using a modified classification system based on the one proposed by Burke et al.10: 1= fracture involving a small portion of the coronal structure; 2= fracture involving a small portion of the coronal structure, but requiring an increase in cavity preparation during the repair procedure; 3= fracture involving the tooth structure with root involvement, which can be restored in association with periodontal surgery; and 4= severe root and crown fracture, which determine tooth extraction. Results The one-way ANOVA revealed significant differences among the groups (p<0.001).The results of the Tukey’s test are described in Figure 2. The onlay preparations restored indirectly with composite resin Filtek Z250 (G6) presented the highest fracture resistance. However, the onlay preparations restored with Filtek Z-250, both directly and indirectly (G5 and G6), presented no statistical difference from each other (p>0.05). The onlay preparations restored directly with Filtek Z250 (G5) did not differ significantly from the other groups either (p>0.05), which presented similar fracture resistance values. The fracture mode data were submitted to the Kruskal-Wallis non-parametric statistical analysis. The results are shown in Table 2. The control group (G1) presented only type 1 failures. The onlay cavities restored with composite resin Z-250, both directly and indirectly (G5 and G6), presented mainly type 4 fractures, which are not repairable. Discussion The null hypothesis of this study was rejected since both the material and the cavity preparation type had an effect on fracture resistance. It would appear that the extensive cavity preparations used in this study significantly reduced the fracture resistance of the premolars11. It has been demonstrated that adhesive restorations may recover fracture resistance to values similar to those of sound non-restored teeth3. In the present study, all restorations presented similar or higher values than those of intact teeth. Moreover, in this study a bonding system and a resin agent were used for cementation of the indirect restorations. This procedure increases tooth resistance compared to the use of non-adhesive conventional cements because it allows the formation of a single body between the restorative material and the dental structure3. It may also be considered that the use of an adhesive luting cement would enhance the fracture strength of the restored unit6. Burke et al.11 reported that one could consider that teeth restored with indirect composite resin restorations would provide similar resistance to that provided by direct composite resin restorations. In the present study, the highest values fracture resistance were obtained with onlays made with Filtek Z-250. It was expected that a more extensive preparation, such as onlays, would present lower values because of the greater amount of dental structure removed compared to inlay preparations11. A possible explanation is that the lower elastic modulus of the direct composite resin promoted a greater distribution of stress than the enamel12, which also comes into contact during the test on intact teeth and inlay preparations. The enamel has high elastic modulus and friability13,14. The stress generated during the compressive load is concentrated and could initiate crack formation and propagation, resulting in lower fracture resistance4 . In addition to the elastic modulus of the material, the cohesive strength is also important in order to improve the fracture resistance of restorations15-17. The indirect composite resin Solidex presents lower filler content (53% v/v) than the direct composite resin Filtek Z-250 (60% v/ v). This difference in the filler content results in a lower elastic modulus of Solidex18, which could be beneficial. On the other hand, the lower filler content reduces the cohesive strength and may compromise the fracture resistance of the restoration19. However, the only difference between Solidex and Filtek Z-250 occurred when the two composite resins were heat light polymerized indirectly. The directly light cured Filtek Z-250 presented no difference from either Solidex or Filtek Z-250 subjected to indirect light polymerization. This probably occurred because the indirect heat light polymerization process increased the degree of conversion of the composite resins, improving their cohesive strength20-22 . In spite of the highest fracture resistance being obtained with onlay restorations made with Filtek Z-250, these restorations presented more severe failure modes when compared to inlay restorations. This observation is perhaps more important than the fracture strength values because these fractured restorations cannot be repaired. One possible explanation is the less homogeneous stress distribution3-4 . The onlay restoration used in this study involved only one cusp, and the other one remained almost intact. This non-homogeneous stress distribution added to more stress absorption by composite resin restoration resulted in a high fracture resistance and predominance of catastrophic failure. Although composite resin Solidex showed lower fracture strength values than those of the heat lightpolymerized Filtek Z-250, it presented more favorable failure modes for this type of cavity preparation. Perhaps this occurred because the lower cohesive strength of this material allowed the material to fail before fracture of the dental structure. Even with all the limitations of an experimental test, it can be observed that direct composite restorations are sufficient for reestablishing the strength of a permanent tooth. However, for more extensive preparations, such as onlays, the composition of the restorative material used was shown to have more influence on the fracture strength than the light activation method used. To restore this type of cavity preparation, the direct composite resin Filtek Z250 can be used indirectly. This technique presents the possibility of improving the degree of conversion of these materials and costs less than the use of a composite resin indicated exclusively for the indirect technique, such as Solidex. Nevertheless, the composite resins with higher filler content, resulting in better mechanical properties, presented a larger number of catastrophic failures in this study. This finding is a serious disadvantage, since it leads to indication of tooth extraction. Within the limitations of this study, it can be concluded that: 1. Adhesive inlay restorations, irrespective of the type of composite resin and light-activation technique used, restored the fracture resistance of intact teeth; 2. Onlay restorations made with composite resin Filtek Z-250 presented the highest fracture resistance, but led to a more catastrophic failure mode. References
© Copyright 2008 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os08035t2.jpg] [os08035f1.jpg] [os08035f2.jpg] [os08035t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}