 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 8, No. 1, Jan-Mar, 2009, pp. 8-14 Higher prevalence of periodontal disease among patients with predialytic renal disease Rosamma Joseph1, Rajaratnam Krishnan2, Vivek Narayan3 1 MDS, Professor and Head, Department of Periodontics, Calicut, Kerala, India
Correspondence to: Rosamma Joseph, Department of Periodontics, Government Dental College, Medical College Campus, Calicut, Kerala, India, 673008 E-mail: drrosammajoseph@gmail.com Received for publication: November 10, 2008 Code Number: os09003 Abstract
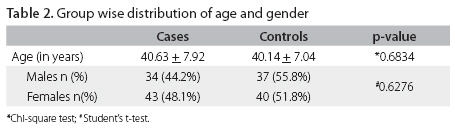
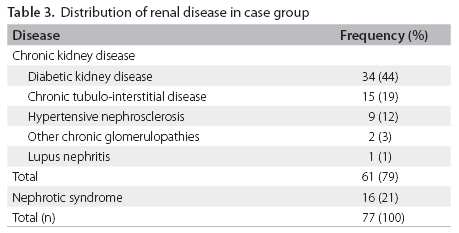
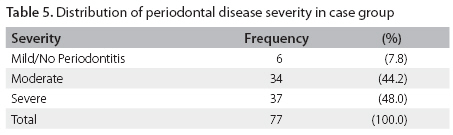
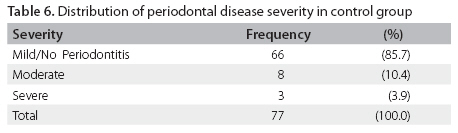
Aim: Periodontal diseases can have a significant effect on the systemic health. Chronic systemic diseases such as renal disease may also influence progression of periodontal disease. The present study assessed the prevalence of periodontal disease among a group of patients with renal disease and compared their periodontal status to that of healthy controls. Keywords: Periodontal disease, periodontitis, nephrology, renal disease Introduction Periodontal diseases comprises of a group of inflammatory diseases affecting the supporting tissues of the teeth resulting from a complex interplay between specific gram-negative microorganisms, their by products and the host-tissue response. This results in progressive destruction of the periodontal ligament and alveolar bone. Earlier, periodontitis had been considered as a disease confined to the oral cavity. However, in the past several years, substantial scientific data have emerged to indicate that the localized infections characteristic of periodontitis can have a significant effect on the systemic health. It is now recognized that the periodontopathic gram-negative bacteria and bacterial products, such as lipopolysaccharides, activate the host immune response significantly and their actions have consequences beyond periodontal tissues. Pro-inflammatory cytokines, such as α2-macroglobulin, α1-antitrypsin and C-reactive protein are significantly elevated during the destructive phase of periodontitis1-4. These inflammatory mediators may have a profound influence in the pathogenesis of many systemic diseases. During the past decade, numerous studies, mostly cross-sectional and few longitudinal, have been carried out and they provide evidence for the link between periodontal and cardiovascular diseases, like atherosclerosis and myocardial infarction5-10. Recently, several studies have been published in the literature, providing evidence for an increased prevalence of periodontal disease in patients with renal disease, especially in dialysis patients, and renal transplant recipients11-19. However, conflicting results regarding the periodontal status of these patients are also available20-24 and further studies are warranted in this regard. The aim of the present study was to know the prevalence of periodontal disease among a group of patients with predialytic renal disease from a South Indian population. Furthermore, we wanted to compare their periodontal status to that of healthy controls. Materials and methods Study population This study was designed as a matched case-control study. Cases were identified as patients attending the outpatient clinic at the Department of Nephrology, Medical College, Calicut, Kerala, India, over a period of six months, from July 2007 to December 2007. Only patients who were diagnosed with renal disease were included. These diseases include chronic kidney disease of varied etiology which includes diabetic nephropathy, lupus nephritis, glomerular disorders, and nephrotic syndrome. Systemically healthy individuals who accompanied patients to Government Dental College, Calicut, during the same period were selected as control subjects. The controls were matched for age, sex, and socioeconomic status. Subjects who had previously undergone dialysis or renal transplantation were excluded from the study. Subjects with history of smoking, those who had received periodontal therapy or systemic antibiotic therapy within a period of six months prior to the examination and subjects with any acute condition that contraindicated a periodontal examination were also excluded. To assess the periodontal status, all subjects were required to have at least six natural teeth. A written informed consent was obtained from all participants in the study. The study was conducted by the joint efforts of the Departments of Nephrology, Medical College, and the Department of Periodontics, Government Dental College. The study was approved by the Institutional Review Board for Human Ethics, Government Medical College, Calicut. Data collection All subjects were required to answer a detailed questionnaire. The information collected included demographic characteristics like name, age, address, sex, occupation etc. A detailed medical and dental history was also collected from all subjects. Oral and dental examination The dental and periodontal examination in all subjects was carried out by a single, trained examiner. The dental status was determined by visual examination under direct and indirect illumination, using a plane dental mirror and a dental explorer. Oral Hygiene Index-Simplified (OHI-S) (Greene and Vermillion)25 for assessing the oral hygiene status. The index was calculated using six index teeth: 16, 11, 26, 36, 31, 46. Modified Gingival Index (MGI) (Lobene et al.)26, for the entire dentition, was calculated as a measure of gingival inflammation. Periodontal examination The periodontal examination was carried out with calibrated periodontal probes with William’s markings. The periodontal status was determined using measurements of Probing Pocket Depth (PPD), Gingival Recession and Clinical Attachment Level measurements (CAL) from four sites on each tooth (buccal, mesial, lingual/palatal, distal). PPD was taken as the distance from the gingival margin to the base of the gingival sulcus/ periodontal pocket. Gingival recession was measured as the distance from the cemento- enamel junction to the gingival margin. These scores were then added up to indirectly obtain the values for CAL. All the subjects were categorized into three groups (Mild/No Periodontitis, Moderate Periodontitis and Severe Periodontitis) based on CAL and PPD measurements, using the criteria proposed by the joint working group of the Centre for Disease Control and Prevention in collaboration with the American Academy of Periodontology in 2003 which are depicted in Table 127. Statistical analysis Descriptive statistics including mean values for OHI-S, modified Gingival Index, PPD and CAL were calculated. For comparisons between the case and control groups, the Student’s t-test and chi- square tests were used for quantitative and qualitative variables respectively. The difference in proportions in both groups was tested using chi- square test. All statistical analyses were carried out using Statistical Package for the Social Sciences package for Windows, version 13. The 95% confidence intervals were taken (p-value < 0.05). Results A total of 154 patients were included in the study (77 in each group). The mean age of patients was 40.38 + 7.47 years. There were a total of 71 males and 83 females in the study. The group wise distribution of age and gender of the subjects is depicted in Table 2. No significant difference was found between the distribution of age and gender among the groups. Table 3 shows the distribution of different forms of renal disease among the case group. Mean values for OHI-S, MGI, PPD and CAL are given in Table 4. All these values were significantly elevated in the case group as compared to controls (p < 0.001). Table 5 indicates the severity of periodontal disease in the case group; 71 patients (92.3%) of the total 77 had moderate to severe periodontitis and the remaining patients (6, 7.7%) belonged to the category Mild/No Periodontitis. Table 6 shows the severity of periodontitis in the control group. Whereas 66 of the 77 subjects (85.7%) belonged to the category of Mild/No Periodontitis, only 11 (14.3%) subjects had moderate to severe periodontitis. When the proportion of moderate to severe periodontal disease between the groups were compared using a chi- square test, it was observed that the prevalence and severity of periodontal disease was significantly higher in the case group as compared to the controls (p < 0.001). Discussion Periodontal disease results from the interaction between specific bacteria existing in the dental plaque biofilm with components of host immune response in susceptible individuals. The inflammatory lesion in periodontitis extends from the gingiva to deeper connective tissues resulting in periodontal pockets and loss of alveolar bone. The periodontal pocket serves as a portal of entry for pathogenic bacteria and their products into the systemic circulation. The large surface area of the aggregate periodontal lesion thus serves as a significant source of inflammation in patients with moderate or severe periodontitis28. A large body of epidemiological evidence provides proof that the systemic chronic inflammatory burden of periodontal disease contributes to endothelial injury and atherosclerosis, perhaps mediated by the acute phase reactants29-34. Previous studies have shown that chronic inflammation contributes to progressive atherosclerosis in patients with end-stage renal disease (ESRD) undergoing hemodialysis35-41. Available data suggest that pro-inflammatory cytokines and the acute phase response play a central role in the genesis of both malnutrition and cardiovascular complications in these patients42. Emerging evidence also suggest that periodontal disease may provide a covert source of systemic inflammation in these patients28,36 and it may, in fact, predict the development of ESRD and the development of overt nephropathy in diabetic patients43. A recently conducted longitudinal study demonstrated that periodontal disease is a significant nontraditional risk factor for chronic kidney disease44. Our study compared the periodontal health status of patients with different forms of renal disease to that of healthy controls from a South Indian population. The results of the present study indicate that a greater prevalence and severity of periodontal disease exists in patients with renal disease. Although many previous authors have obtained similar results11-19, conflicting reports are also available and they have failed to detect any difference in the periodontal health in patients undergoing hemodialysis.20-24 In the present study, all the periodontal parameters (OHI-S, MGI, PPD and CAL) were elevated in the case group as compared to the control group and the results were statistically significant. The periodontal destruction as indicated by elevated PPD and CAL levels is significantly worse in the case group (2.4 + 0.40 and 2.76 + 0.66) as compared to the controls (1.3 + 0.49 and 1.50 + 0.72). The prevalence of moderate to severe periodontitis in the case group (92%) is very high as compared to that in controls (14.3%). While earlier authors14, 18, 22 have conducted similar studies in dialysis populations, our study population included only predialytic patients. The prevalence obtained in the present study is greater than that observed by previous studies in hemodialysis patients (58.914 and 25.9%22) and in chronic ambulatory peritoneal dialysis patients (67.3%)18. Therefore, our study result confirms our hypothesis that a greater prevalence and severity of periodontal disease exists in patients with renal disease as compared to systemically healthy controls. It might be possible that severe periodontal inflammation in these patients could have also contributed to the level of their renal disease burden. The systemic disease burden could have also influenced the progression of periodontal disease in these patients. It has been already established that the chronic renal condition could have significant effects on the prevalence and severity of periodontal disease24,45. A recent study conducted in a Japanese population suggests that the increased incidence of chronic renal failure that occurs with age might increase the probability of severe periodontal disease in community-dwelling elderly subjects45. The authors also postulate that periodontal disease is influenced by chronic renal failure because of insufficient bone metabolism. Earlier studies provide evidence that vitamin D polymorphisms may predispose to both chronic kidney disease and periodontitis46. Hence it is possible that periodontal disease and chronic kidney disease might share common risk factors. Our study, being cross-sectional in design, does not establish a cause and effect relationship. Therefore, further studies are necessary to elucidate the complex relationship between these chronic diseases. To conclude that the development of periodontal disease preceded the onset or progression of the renal condition, further studies with longitudinal study designs are necessary. Another limitation of this study is that the case group included subjects with diabetic kidney disease. This may be regarded as a confounder as diabetes mellitus is a risk factor for both, renal and periodontal disease. The studies that have assessed the effect of periodontal therapy on systemic inflammation provide promising results. Several reports have indicated that periodontal therapy, consisting of scaling and root planning and microbial plaque control, results in decreased levels of markers of systemic inflammation47,48 and may contribute to improved endothelial function49,50. However, further research with well controlled randomized clinical trials is necessary to establish whether early detection of periodontal disease followed by effective periodontal therapy will actually result in decreased in atherosclerotic complications in patients with renal disease. This study provides evidence for a greater prevalence and severity of periodontal disease among predialytic patients with renal disease. As periodontal evaluation is not performed as part of routine medical assessment in these patients, the periodontal source of inflammation may be overlooked. We hope that the results of our study provide emphasis for the fact that the periodontal health of all patients with renal disease needs to be carefully monitored. References
Copyright © 2009 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os09003t4.jpg] [os09003t1.jpg] [os09003t5.jpg] [os09003t3.jpg] [os09003t6.jpg] [os09003t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}