 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 8, No. 1, Jan-Mar, 2009, pp. 30-33 Knoop hardness of composites cured with halogen and led light-curing units in class I restorations Maria Cecília C. Giorgi1, Luís Alexandre Maffei Sartini Paulillo2 1 DDS, MS, Graduate student, Department of Restorative Dentistry, Faculdade de Odontologia de Piracicaba, Universidade Estadual de Campinas (Unicamp), Piracicaba (SP), Brazil
Correspondence to: Luís Alexandre Maffei Sartini Paulillo, Avenida Limeira, 901 – Areão, CEP 13414-903 – Piracicaba (SP), Brazil E-mail: paulillo@fop.unicamp.br Received for publication: August 29, 2008 Code Number: os09006 Abstract
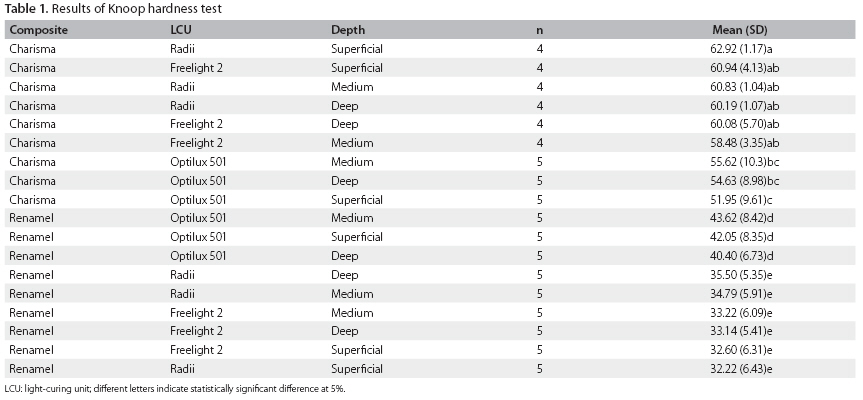
Aim: To evaluate the effect of light-curing units (LCUs) on the microhardness of class I composite restorations at different depths. Keywords: composite resins, hardness Introduction Light-activated composite materials polymerize by free radical polymerization when exposed to light at wavelengths in the 400 to 500 nm range. The photoinitiator absorbs light energy emitted from the light-curing unit (LCU), and directly or indirectly initiates polymerization1. Camphorquinone (CQ) is a commonly used photoinitiator that absorbs energy and reacts with a photo reducer to begin the polymerization process1-3. Both the light source and the resin composite play an important role in ensuring adequate polymerization. Composites can be easy, moderate or difficult to polymerize because of the differences in their photoinitiator content like shade, filler size and filler load4. While the resin composite composition and shade influence polymerization, light intensity and wavelength are also contributing factors5. If a light-activated composite does not receive sufficient total energy at the correct wavelength from the LCU, several clinical consequences6 will be observed, such as decrease in the mechanical properties7-9; increase in water sorption and solubility, reduced hardness and potential pulpal damage10,11. Quartz tungsten halogen (QTH) LCUs are the most widely sources for composite activation, but light emitting diode (LED) LCUs are gaining popularity12. The main difference between these light sources is that QTH LCUs produce a broad wavelength spectrum and need a filter to reduce output of undesired wavelengths, delivering light in the 410 to 500 nm region of the visible spectrum1. Halogen light bulbs generate light when electrical energy heats a small tungsten filament to extremely high temperatures1,3, which are responsible for QTH light bulb or filter deterioration, decreasing the power density of the curing unit and resulting in a lifetime of 30 to 50 hours. On the other hand, LED units produce a narrow band of wavelength, specifically chosen to excite the CQ, and last for thousands of hours because they convert electricity into light more efficiently, producing less heat. The use of only a radiometer to compare the curing efficacy of LED and QTH LCUs is not sufficient because these LCUs emit light in a different spectrum of the visible light13. Tests that evaluate mechanical properties of the cured material are the most indicated method to determinate the light activation potential of these light sources14. The good correlation, between the results of hardness testing and infra-red spectroscopy15,16, has allowed the microhardness to be a frequently used method to investigate the factors which influence the effectiveness of polymerization, since it is relatively easier to perform16. The aim of this study was to investigate the effect of QTH and LED LCUs on the microhardness of microfilled and microhybrid composite resin restorations placed in class I cavities at three different depths. The null hypothesis tested was that composite resin microhardness is not influenced by different LCUs. Material and methods In the present study, two LED LCUs (Freelight 2; 3M/ESPE, St. Paul, MN, USA and Radii; SDI Ltd, Victoria, Australia) and one QTH LCU (Optilux 501; Kerr-Demetron, Orange, CA, USA) were used. Since the Radii LED LCU operates only in soft-start mode, the other curing units were initially activated for five seconds with increasing intensity and, thereafter; light activation was done for 10, 20 or 40 seconds, according to the manufacturers’ recommendations, in a continuous mode. Thus, Optilux 501 QTH LCU was set in such a way that the first five seconds were in an exponential mode, and the continuous mode was activated immediately afterwards. The corresponding option was selected for Elipar Freelight 2 LED LCU. All LCUs were, thus, used for the same time. Emission spectra and power output were measured before the experiment to characterize the units. A power meter (Ophir Optronics Inc., Wilmington, MA, USA) and an integrating sphere 3A-P-SA (Ophir Optronics Inc.) were used for power measurement. The power density of each LCU was determined by measuring the output power of the entire light guide and dividing the output power by the area of the light guide or lens. Output powers of 526, 381 and 960 mW/cm² were found for Optilux 501, Radii and Freelight 2, respectively. The energy density (mJ/cm²) was determined by the product of power density and time. The spectra were measured with a spectrometer USB 2000 (Ocean Optics Inc, Dunedin, FL, USA) and are presented in Figure 1. A microhybrid (Charisma; Heraeus-Kulzer GmbH, Hanau, Germany) and a microfilled (Renamel; Cosmedent Inc., Chicago, USA), composite resins, both A3 shade, were used in association with a two-step etch-and-rinse adhesive system (Single Bond; 3M/ESPE). Thirty sound human third molars were selected for this study. The teeth were embedded in PVC molds with polystyrene resin (Piraglass, Piracicaba, SP, Brazil) in such a way that the crown and the 5 mm below the cementoenamel junction remained exposed. After inclusion, the occlusal surfaces of teeth were cut off with a water-cooled low-speed double-faced flexible diamond disc (#7020; KG Sorensen, São Paulo, SP, Brazil) and flattened in a polishing machine (South Bay Technology Inc, San Clemente, CA, USA) using 180- and 360-grit abrasive paper (Carborundum, Saint-Gobain Abrasivos Ltda, Cruz de Rebouças/Igaraçu, PE, Brazil) under water cooling. Standardized box-shaped class I cavities were prepared using a precision cavity preparation device. The cavities were outlined with a carbide bur (#FG 245; SS White, Rio de Janeiro, RJ, Brazil) operated in a high-speed handpiece (Kavo do Brasil SA Ind. & Com., Joinvile, SC, Brazil) using copious air-water spray. A new bur was used for every five preparations. The final cavities had a mesiodistal width of 4 mm, a buccolingual width of 3 mm and depth of 3 mm. The teeth were randomly divided into six groups of five teeth each and restored with either Charisma or Renamel composites and light-cured with Optilux 501, Radii or Freelight 2. The exposure time used was 20 seconds for Charisma and 40 seconds for Renamel, according to manufacturer’s recommendations. For all groups, a 37% phosphoric acid gel (Cond Ac 37; FGM Dental Products, Joinville, SC, Brazil) was applied to the entire cavity for 15 seconds. The acid was rinsed off with water spray for 15 seconds and the excess water was removed with a small damp cotton pellet. Single bond adhesive system was applied in accordance with the manufacturer’s instructions to the cavity walls and light-cured. After that, the cavity was restored incrementally in three oblique layers less than 2 mm thick. The increments were light-cured for the recommended time with the light source close to the occlusal surface without touching it. The finishing of restorations was done with flexible discs (Sof-Lex Pop on; 3M/ESPE). After seven days of storage in water at 37 ± 1° C, the teeth were decoronated at the cementoenamel junction using a water-cooled low-speed saw and the roots were discarded. The crowns were, then, bisected mesiodistally parallel to their long axis resulting providing two halves. Each half was embedded in polystyrene resin to facilitate handling and microhardness testing. The included restorations were finished with wet 400-, 600- and 1,200-grit Al2O3 abrasive paper and then polished with 3 and 1 µm diamond paste (Arotec Ind. Com., São Paulo, Brazil) using a polishing cloth. Microhardness was measured by means of a Knoop indenter under 25 g load and 20 seconds dwell time (HMV-2000, Shimadzu, Japan). Fifteen indentations were made in each specimen, five at each depth of 500, 1,500 and 2,500 µm. For depth, the values read, referring to the size of the greater diagonal, were transformed into Knoop Hardness Number (KHN) and the average of the values was calculated. Data was submitted to a three-way ANOVA (resin composite versus LCU versus depth) followed by a Tukey’s multiple comparison test (LS means) at α = 0.05 significance level. Results There were statistically significant differences (p < 0.05) between the composite resins and a composite versus LCU versus depth triple interaction (Table 1). The highest KHN (p < 0.05) was obtained for the microhybrid composite Charisma when light-cured with Radii at the superficial depth, with no difference (p > 0.05) to Radii at the other depths and Freelight 2 at all depths. However, there was statistically significant difference (p < 0.05) when Charisma was light-cured with the halogen LCU at all depths, compared to the same composite cured with Radii at the superficial depth. The microfilled Renamel presented significantly lower (p < 0.05) hardness than Charisma in spite of the curing unit and depth. The lowest KHN (p < 0.05) was obtained when Renamel was light-cured with both LED LCUs, irrespective of the depths. However, when Renamel was cured with the QTH curing unit, there was a significant increase (p < 0.05) in hardness compared to the LED LCUs at all depths. The null hypothesis was rejected. Discussion Radii showed the lowest light irradiance (381.6 mW/cm²) among the tested LCUs. Since the exposure time was the same for all devices, it also presented the lowest energy density (irradiance versus time). However, there were no significant differences between the mean KHN values of Charisma cured with Radii and the other units, which had light irradiance of 960 mW/cm² (Elipar Freelight 2) and 526 mW/cm² (Optilux 501). The hypothesis that LEDs could produce a polymerization depth similar to that of QTH LCUs, in spite of showing lower irradiance, is due to their better overlap between the emission and absorption spectra of LCUs and photoinitiators9. The absorption peak of CQ in methylmethacrylate resins is 470 nm, which is coincident with the emission peak of the LCUs evaluated in the present study (450 to 490 nm). Outside this range, however, the wavelength dependence is much stronger and the conversion rate drops rapidly17. No significant differences were observed at the superficial depth of Charisma cured by Radii and Elipar Freelight 2 compared to Optiliux 501, with LEDs resulting in higher KNH values. Considering the energy density applied, one could expect that Optilux 501 (13,150 mJ/cm²) would behave similarly to Radii (9,540 mJ/cm²). The superior performance of Radii may be justified by its emission spectrum, which is more coincident with the absorption peak of CQ. The hardness values obtained by Freelight 2 and Radii did not differ significantly from each other, although the former showed more than twice the energy density when compared to the latter (24,000 mJ/cm² and 9,540 mJ/cm², respectively). A possible explanation for this result is that Radii does not have a fiber optic tip, but an acrylic structure instead, called lens cap, which may have affected the measurement of irradiance by the radiometer. In all groups, the microfilled composite Renamel presented lower hardness values than the microhybrid composite Charisma. This is in agreement with the results of previous studies18,19, and can be explained by the fact that microfilled composites are more difficult to light-cure than microhybrid composites20, indicating that adequate polymerization is not only a function of exposure time to the light, but it is also influenced by the material’s composition18. The small filler size of microfilled composites causes light scattering, decreasing the effectiveness of polymerization6,21,22. Furthermore, resistance, hardness and other mechanical properties of the composites are influenced not only by the degree of conversion, but also by the nature of the monomer subunits of the polymer. Thus, tetraethylene glycol dimethacrylate (TEGDMA) monomer is more flexible then Bis-GMA. The flexibility of TEGDMA is related to the ether linkages of the molecule, giving rise to only slight barriers to free rotation about the bonds. The relative stiffness of Bis-GMA is related to the bulk, aromatic groups of the central part of the molecule, causing much larger barriers to rotation about the bonds23. As Renamel has a higher TEGDMA content in its composition, its lower hardness can also be credited to the nature of the resin matrix. The highest KHN values of Renamel were obtained when the material was light-cured with the QTH LCU at all depths, while the lowest KHN values of Renamel at al depths were obtained when it was light-cured with both LED LCUs, at all depths. Due to the broad wavelength spectrum emitted by QTH, the light presents a portion of emitted light with higher wavelengths and it also presents better transmittance in microfilled composites with the potential of hitting photoinitiators at deeper depths24. Arikawa et al.24 showed that there was a tendency of increase in light transmittance in the material body when an increase in wavelength from 400 nm to 700 nm occurred. The authors explained this result based on the Rayleigh equation24, which indicates that higher light scattering occurs at lower wavelengths. Consequently, the decrease in light transmittance at lower wavelengths can be caused by higher light scattering in the material. This might have occurred with the LED LCUs, which have narrower spectra. The use of LED LCUs may represent a clinical advantage because they undergo minimal degradation of the device. In addition, QTH LCUs are known to generate heat resulting, which results in degradation of their constituents over time and decrease in light irradiance. However, the findings of the present study showed that, LED LCUs do not present the same performance for different types of composites. Therefore, it is important that clinicians also know the composition of materials, especially regarding their filler particles and photoinitiator, when choosing a LCU to be used in daily practice. References
Copyright © 2009 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os09006f1.jpg] [os09006t1.jpg] |
| |||||||||

{kind=link}
{kind=link}