 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Braz J Oral Sci, Vol. 8, No. 3, July-September, 2009, pp. 128-131 Cast metal core adaptation using two impression materials and intracanal techniques Sônia Maria Lemos Brancato Camarinha1, Luiz Carlos Pardini2, Lucas da Fonseca Roberti Garcia3, Simonides Consani4, Fernanda de Carvalho Panzeri Pires-de-Souza5 1DDS, MS, Graduate student, Department of Dental
Materials and Prosthodontics, Ribeirão Preto Dental School, University
of São Paulo, Brazil
Correspondence to: Lucas da Fonseca Roberti Garcia, Rua Bernardino de Campos, 30 - Apto. 1002 - Higienópolis 14015-130 - Ribeirão Preto, SP, Brasil, Phone: +55-16-3964-6910/ +55-16-9796-0776. E-mail: drlucas.garcia@gmail.com Received for publication: May 22, 2009
Code Number: os09026 Abstract Aim: This study evaluated the adaptation of cast metal cores
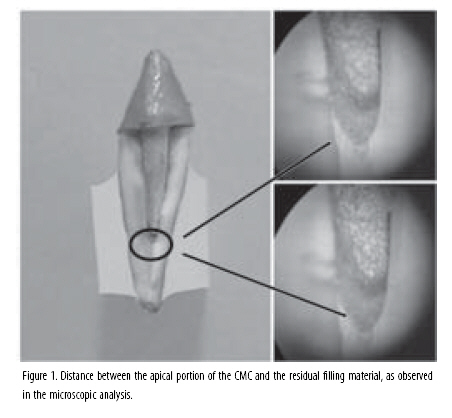
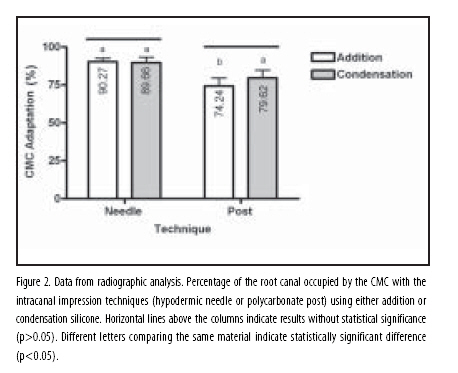
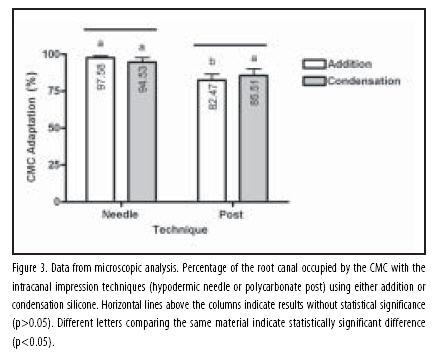
(CMCs) using two impression materials and two intracanal impression techniques. Keywords: impression technique, cast posts, silicone elastomers, intraradicular support. Introduction Endodontically treated teeth are usually weakened due to the loss of dental structure by caries, cavity preparation, root canal instrumentation and decrease of dentin moisture, becoming more susceptible to fractures1. The restoration of an endodontically treated tooth should reestablish its form and function, creating resources for anchorage of the restorative material that are capable to avoid displacement and promote an adequate distribution of the forces acting on the restoration2-3. The construction of a cast metal core (CMC) is one of the possible treatment options to increase tooth resistance to fracture and serve as a support for a subsequent prosthetic restorative treatment4. The best possible core adaptation to the root canal should always be pursued because it is a critical factor for achieving an optimal retentive and biomechanical behavior of the fixed denture5. Direct intracanal impression for CMC fabrication is a very time-consuming procedure because the dentist needs to have direct access to the root canal during all phases of preparation, adjustment and finishing/polishing of the core6. Indirect intracanal impression for CMC fabrication may thus be a viable and time-saving option. In this technique, impression of the root canal is obtained with an elastomeric impression material. A fundamental requirement for a correct CMC adaptation is the accurate reproduction of the prepared canal space shape in all of its details in order to distribute forces uniformly within the root7. The success of all subsequent operative steps depends directly on the production of a precise mould8. The use of appropriate impression materials and correct molding techniques reduces considerably the possibility of fails in the molds8. Among the elastomeric materials, silicones have as advantages their ease of handling and lack of significant alterations at room temperature8-9. However, byproducts (e.g.: ethyl alcohol) formed in the condensation silicone reaction promotes a slow and small contraction due to its evaporation8-9. Addition silicones are considered superior compared to others elastomeric materials because they do not have byproduct formation, which reduces the polymerization shrinkage of the material10, promoting higher dimensional stability and an appropriate resistance to rupture8-10. Due to the anatomic characteristics of the root canal system, the precise reproduction of the end of the prepared canal is difficult, which may result in a CMC with inadequate length and a high degree of distortion from the mould11. Therefore, the development of impression techniques that may increase the quality of reproduction and hence improve CMC adaptation to the prepared root canal is necessary12. Thus, the purpose of this study was to compare radiographically and microscopically the adaptation of CMCs fabricated from intracanal impressions obtained using an indirect double-impression procedure with two elastomeric impression materials (addition and condensation silicone) and two intraradicular supports (polycarbonate posts and hypodermic needle). The tested hypothesis was that the use of a hypodermic needle as an intraradicular support allows for the air exiting the canal during injection of the light body impression material promoting a better material flow and more accurate reproduction of the canal space. Material and methods This study was conducted after approval of the research protocol by the Research Ethics Committee of Ribeirão Preto Dental School, University of São Paulo, Brazil (Process # 2005.1.1204.58.7). Ten single-rooted human teeth were selected from a random collection and were checked for absence of root caries, cracks and structural defects. Soft debris was removed with hand curettes. Initially, the teeth were radiographed using F-speed periapical x-ray films (Insight, Eastman Kodak Company, Rochester, NY, USA) with a Heliodent 60B X-ray device (Siemens, Erlangen, Germany) operated at 60 Kvp and 10 mA, with 0.16 s exposure time, total filtration equivalent to 2 mm Al and 18 cm focus-film distance. All films were labeled with lead letters and numbers (Konex, São Paulo, SP, Brazil) and all teeth were radiographed near a 10x32mm aluminum step-wedge with variable thickness (from 2 to 16 mm, in 2 mm increments) in order to simulate the densities of the oral structures compared to that of the soft and hard tissues, and hence detect possible variations during the radiological procedures. Crowns were removed at the cementoenamel junction with a water spray-cooled double-faced diamond disc (KG Sorensen, São Paulo, SP, Brazil). The root canals were instrumented with a series of K-files (Dentsply/Tulsa Dental, Tulsa, OK, USA) according to a step-back technique, being irrigated with 0.5 mL of 2.5% sodium hypochlorite at each change of instrument. The canals were obturated by cold lateral compaction of gutta-percha and a zinc-oxide-eugenol-based sealer (Endofill, Dentsply Indústria e Comércio Ltda., Petrópolis, RJ, Brazil), and the root-filled teeth were stored in distilled water at 37oC during 48 h for complete setting of the sealer. After this period, 2/3 of the filling material was removed with Peeso burs (FKG Dentaire, La Chaux-de-Fonds, Switzerland) mounted in a low-speed handpiece (Dabi Atlante, Ribeirão Preto, SP, Brazil). In order to warrant standardization of the amount of filling material to be removed from each canal, the working length of all roots was measured with a digital caliper (Absolute, Mitutoyo, São Paulo, SP, Brazil). Next, the roots were radiographed again in the same way as described above. Using an indirect double-impression procedure, the prepared root canals were molded with either addition-cure silicone (polyvinyl siloxane - Adsil; Vigodent S/A Indústria e Comércio, Rio de Janeiro, RJ, Brazil) or condensation-cure silicone (Speedex; Vigodent S/A Indústria e Comércio) impression materials using two types of intraradicular supports: 0.70 x 30 mm hypodermic needles or prefabricated polycarbonate posts designed for root canal impression (Pin-Jet; Angelus Indústria de Produtos Odontológicos Ltda, Londrina, PR, Brazil). Four impressions were obtained from each tooth (one for each type of impression material and intraradicular support) totalizing 40 impressions that were allocated to 4 groups (n=10). An intracanal impression protocol was developed for this study using a delineator. A partial impression tray was adapted to the vertical shaft of the delineator in such a way that it could be loaded with impression material always following the same insertion and removal path. Another partial impression tray with a central hole for attachment of the teeth was loaded with autopolymerizing acrylic resin (Artigos Odontológicos Clássico, São Paulo, SP, Brazil) and fixed at the delineator's base. Two 1-cm-thick resin cylinders fixed at the delineator's base served as stoppers that limited the insertion of the tray to a standardized depth. Manufacturers mixing instructions were followed for both impression materials. A 380 g load was applied during the impression procedures and maintained until complete setting of the materials in order to standardize the force applied to the trays. The double-impression procedure can be summarized as follows. First, a layer of #7 wax (Herpo Produtos Dentários Ltda, Rio de Janeiro, RJ, Brazil) was applied on the tooth to be molded and an acrylic resin layer (Artigos Odontológicos Clássico) was applied onto the wax. After polymerization, the wax was removed and the acrylic resin was adapted on the tooth to serve as a relief for the intracanal impression with the light body material. An initial impression was obtained with the heavy body material, with care to avoid material flowing into the canal. The acrylic relief was removed together with the heavy body material and the intraradicular support was positioned loosely inside the root canal. Next, the light body material was injected into the canal with a syringe in a sufficient amount to fill it completely and reach the working length. After complete setting, the material/intraradicular support set was removed in a single movement, obtaining a final mould. All moulds were poured with type IV dental stone (Durone, Dentsply Indústria e Comércio Ltda.), copying the area corresponding to the prepared canal space. Acrylic resin cores (Duralay, Reliance Dental Mfg Company, Worth III, USA) were fabricated on the stone models according to the brush technique described by Nealon13, for further inclusion (Termocast Investment; Polidental, Cotia, SP, Brazil) and casting with Cu-Al alloy (Aje Goldent Comercial Ltda., São Paulo, SP, Brazil). The accuracy of the intracanal impression techniques was analyzed radiographically and microscopically. For the radiographic analysis, the roots were radiographed with the CMC in position using the same intraoral film, X-ray equipment and parameters described before. The radiographs were digitized and analyzed using ImageLab image-analysis software (Softium, São Paulo, SP, Brazil). For the microscopic analysis, the teeth were embedded in acrylic resin, sectioned longitudinally using a digital precision low-speed diamond saw (SYJ-150, MTI Corp., Richmond, CA, USA) and the CMC was fitted to the canal and examined with a two-coordinate microscope (Nikon Measurescope; Nippon Kogaku K.K., Chiyoda-ku, Tokyo, Japan). In both analyses, CMC adaptation to the canal was determined by calculating the percentage of the prepared canal space that was occupied by the core. In the radiographic analysis, the length of the prepared canal space (from the coronal third up to the beginning of the residual filling material was initially measured and then the coronal-apical length of the core was measured in the same image. In the microscopic analysis, canal space and core length were measured separately (Figure 1). Data were subjected to statistical analysis by 2-way ANOVA and Bonferroni correction at 5% significance level. Results The data obtained from the radiographic and microscopic analyses are graphically presented in Figures 2 and 3. Similar results were obtained in both analyses. The CMC fabricated from both addition and condensation silicone impressions using hypodermic needles as intraradicular supports presented significantly higher filling percent values, which indicate a better CMC adaptation to the prepared canal (p<0.05). Comparing the impression materials (Figure 2), there was no statistically significant difference (p>0.05) in the percentage of prepared canal space occupied by the CMC regardless of the type of intraradicular support. Comparing the techniques, the use of hypodermic needle as an intraradicular support produced significantly better (p<0.05) CMC adaptation to the canal when addition silicone was the impression material. For the condensation silicone, no statistically significant difference (p>0.05) was observed between the impression techniques. Discussion The use of adequate impression material techniques reduces significantly the likelihood of inaccuracies, such as CMC misfit, during intracanal impression procedures8. Starting from the first impression of the canal, small distortions are successively incorporated during all subsequent stages of up to the definitive installation of the prosthesis14. The challenge is to determine a minimum level of distortion and associated stress that is acceptable and that confers adequate clinical longevity to the prosthesis. Impression materials and techniques that are able to reproduce canal anatomy with a high level of reliability are expected to allow the fabrication of prosthetic pieces with the least possible misfit to the canal8. The present in vitro study was designed to analyze radiographically and microscopically the adaptation of CMCs to the root canal of extracted human teeth. Endodontically treated human teeth were used to simulate the clinical conditions as close as possible15-17. The radiographic technique is the most suitable for evaluation of CMC adaptation because, in clinical practice, a radiographic image is obtained to certify that the CMC is well adapted, occupying the whole extension of the root canal18. However, due to the limitation imposed by the x-ray diffraction, such as the superposition of structure images and distortions18, the microscopic analysis of the CMC adaptation was also performed in the present study. Periapical radiographs are the most commonly used in dental offices to ensure that the core is intimately fitted and occupies the whole extent of the prepared canal space18-19. In the present study, both radiographic and microscopic analyses showed that the intracanal impression technique combining addition silicone and hypodermic needle produced a more accurate reproduction of the canal space as demonstrated by fabrication of CMCs with better adaptation to the canals. When the condensation silicone was used, the intraradicular supports had a similar performance with no statistical significance in CMC adaptation. The difference between the intracanal impression techniques when addition silicone was used can be explained by the highest flowability of the light-body paste, in addition to its capacity of offering better reproduction of details than the condensation silicone8-10,20. Condensation silicones are more susceptible to fail, irrespective of the molding technique. According to Stackhouse Jr20, the lack of space for adequate flow of the light-body impression material induces the formation of an internal pressure during the impression procedure that leads to air entrapment into the root canal. It is assumed that this phenomenon occurred in the present study in the technique that used polycarbonate posts as intraradicular supports. During injection of the light-body material after placement of the polycarbonate post, the internal pressure formed by the air contained in the canal promoted bubble formation and the impression resulting from this procedure presented inaccuracies that interfered with CMC adaptation20. On the other hand, the use of hypodermic needle as an intraradicular support allowed the air exiting the canal during injection of the light-body impression material, which promoted a better material flow within the canal space. As a result, a more accurate impression was obtained and the CMC was more precisely adapted to the canal. In both analyses, the impression material did not produce significant differences in the results. The impression technique, on the other hand, had a significant influence on core adaptation, with better results when hypodermic needles were used regardless of the impression material. No previous study used hypodermic needles as supports for intracanal impression in the fabrication of cast metal cores. Additional in vitro and in vivo studies should be performed to confirm these findings before the clinical use of this technique can be recommended. Within the limitations of this study, both radiographic and microscopic analyses showed that: 1. the intracanal impression technique using hypodermic needle as intraradicular support provided significantly better CMC adaptation than the technique using polycarbonate post when the cores were fabricated from addition silicone impressions; 2. the type of impression material did not interfere on CMC adaptation to the canal. References
Copyright 2009 - Braz J Oral Sci The following images related to this document are available:Photo images[os09026f3.jpg] [os09026f2.jpg] [os09026f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}