 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Braz J Oral Sci, Vol. 8, No. 3, July-September, 2009, pp. 145-148 Mixture of betel leaf, areca nut and tobacco chewing is a risk factor for cytogenetic damage in construction workers from south India Sellappa Sudha1, Balakrishnan Mythili2, Vellingiri Balachandar3 1Associate Professor, Department of Biotechnology,
School of Life sciences, Karpagam University Coimbatore, Tamil Nadu, India Correspondence to: Sellappa Sudha Department of Biotechnology, School of Life sciences, Karpagam University Coimbatore-641021, Tamil Nadu, India Phone: +91-422-2611146. Fax: +91-422-2611043 E.mail: sudhasellappa@yahoo.co.in Received for publication: July 23, 2009
Code Number: os09030 Abstract Aim: To determine the cytogenetic effect of betel leaf, areca
nut and tobacco mixture usage among female construction workers in Tamilnadu,
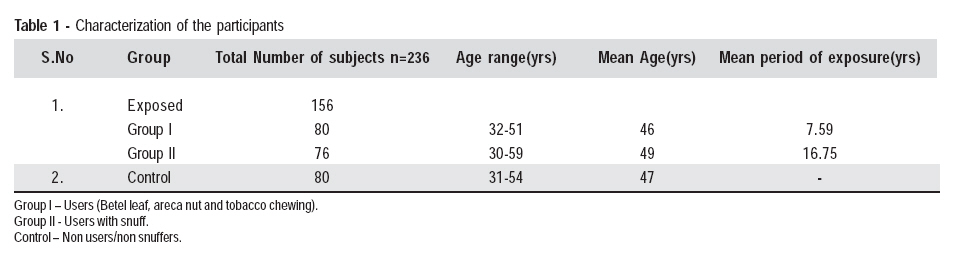
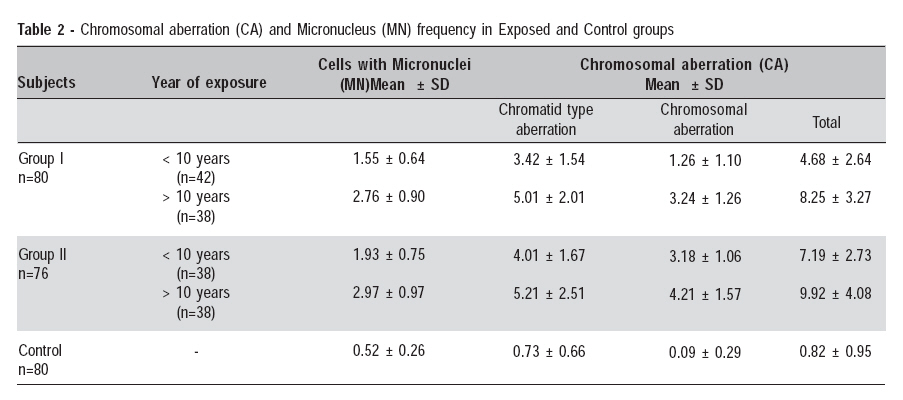
Southern India. Keywords: betel leaf, areca nut, tobacco snuff, chromosomal aberration, micronucleus. Introduction Worldwide, betel quid is among the most common addictions subsequent to tobacco, alcohol and caffeine. Its use is very popular in India. Many Indian women in rural areas regularly chew betel quid, a combination of areca nut, betel leaf (from Piper betle), lime paste, and leaf tobacco. Users are easily identified because the quid causes the teeth to turn black brown and stain the tongue and oral mucosa. The habit of betel quid chewing is quite common throughout Southeast Asia. It is estimated that between 10% and 20% of the world's population chews betel quid1-2. The International Agency for Research on Cancer (IARC) regards the chewing of betel leaf and areca nut to be a known human carcinogen3, which have role in multistage progression of oral cancer4. Smokeless tobacco contains nitrosonornicotine and 4-(methylnitrosamino)-1-(3-pyridyl) - 1-butanone; areca nut contains arecoline and 3-(methylnitrosamino) propionitrile, while lime provides reactive oxygen radicals, each of which has a role in oral carcinogenesis5. Chewing betel quid without tobacco is an independent risk factor for developing oral cancer6. When betel quid with tobacco is consumed with alcohol and smoking the relative risk increases 11-fold7. Betel leaf contains large amounts of carcinogens called safrole, which is readily metabolized and excreted in urine. Betel quid and areca nut chewing leads to oral sub-mucous fibrosis, a painful disabling and potentially precancerous condition of the oral mucosa. Betel quid chewing is a major risk factor for cancer in mouth, pharyngeal cavity and upper digestive tract8. Regular use of betel quid have several adverse effect on oral cavity and upper digestive tract, including inflammation, development of white or gray patches on the tongue and buccal mucosa and oral cancer 9. Chewing a mixture of betel leaf, areca nut and tobacco is a complex behavior and is poorly studied. Betel and areca nut chewing has been extensively studied in populations in many part of the world. However genotoxic effect of combinational use of betel quid with snuff has received less attention. The purpose of this study was to evaluate the MN and CA of individuals regularly using a mixture of betel leaf, areca nut and tobacco with snuff tobacco. Chromosomal aberrations (CA) in peripheral blood lymphocytes and micronucleus (MN) in buccal mucosa are considered as reliable biomarkers of genotoxic exposure to both physical and chemical agents10, and an increase in CA/ MN frequency indicates the risk of exposure to clastogenic and/or aneugenic agents. In addition, cytogenetic end points in peripheral blood lymphocytes have been used as biomarkers which allow a reasonable epidemiological evaluation of cancer predictability11. Material and methods The subjects were selected by random sampling. The study group consisted of 156 healthy female construction laborers and 80 healthy subjects who did not use any form of tobacco or alcohol and working in the same environment were selected as controls. Study area is Coimbatore city, South India. The exposed group includes 80 individuals (Group I) who regularly chewed a mixture of betel leaf, areca nut and tobacco (users) and 76 users with snuffing habit (Group II). For assessment of smokeless tobacco habits among construction workers, the sample was classified as users and users with snuffing. The form of smokeless tobacco use (chewing and/or snuff), the number of years of consumption (duration) and the number of units used per day were recorded by subject interview. Subjects were then classified based on duration of tobacco usage into less than 10 years and more than 10 years. Before collecting the sample, all subjects were interviewed to evaluate their habits, according to the protocol published by the International Commission for Protection against Environmental Mutagens and Carcinogens12. Venous blood samples (5 mL) were drawn in heparinized syringes from each subject for the chromosomal analysis. The work was carried out in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki13. Chromosomal Aberration Assay Blood samples were used to establish leukocyte cultures by following standard procedures6. 0.5 mL blood was added to 4.5 mL RPMI 1640 medium supplemented with 10% calf fetal serum, 2 mM l-glutamine, 1% streptomycin-penicillin, 0.2 mL reagent grade phytohemagglutinin, and was incubated at 37 ºC. After 50 h, cultures were treated with 0.1 g/mL colcemid to arrest the cells at metaphase in mitosis. Lymphocytes were harvested after 52 h by centrifuging cell suspension to remove culture medium (800-1000 rpm), addition of hypotonic solution (KCl 0.075 M) at 37 ºC for 20 min to swell the cells, and treated twice with Carnoy's fixative (3:1 ratio of methanol: acetic acid). Slides were carefully dried on a hot plate (56ºC, 2 min). Later, the slides were stained using the Giemsa technique. For the CA analysis, 100 well spread complete metaphase cells in first cell cycle were evaluated per subject under a microscope at ×100 magnification to identify numerical and structural CA. Chromatid-type CAs: (chromatid gaps; chromatid breaks) Chromosome-type CAs: (break; gap; exchange) were observed. Micronucleus Assay Buccal cells were sampled with a tooth brush from the inside of both cheeks and placed in 50ml tubes containing 25 mL of buffer solution (0.1M EDTA. 0.01M Tris HCL 0.02 M NaCl) pH 7.0, the cells were washed thrice in the buffer solution by centrifugation and slides for microscopic analysis were prepared14. Cell suspension was dropped onto clean slides and cell density was checked using a microscope. The slides were allowed to dry and then fixed in 80% cold (0°C) methanol. The samples were then applied to clean microscope slides. Smears were air dried and fixed in methanol: acetic acid (3:1). Slides were stained with May-Grunewald Giemsa method (Sigma St Louis MO). The MN analysis was done with a light microscope, at x 100 magnification, using coded slides. 1000 cells from each individual were examined. Only unfragmented cells that were not smeared, clumped or overlapped and that contained intact nuclei were included in the analysis. Criteria used for identification of micronuclei were according to the method of Countryman and Heddle15. Results Table 1 shows the total number of subjects, age range, mean age and mean duration of exposure. The study subjects were categorized into two groups based on type of exposure (users and users with snuff). Table 2 shows frequencies of chromosome aberrations and frequency distribution of micronuclei. The mean percentages of MN cells in Group I was 1.55 ± 0.64 for less than 10 years of habitual exposure and 2.76 ± 0.90 for more than 10 years of exposure. In the controls, the mean percentage of MN cells was 0.52 ± 0.26. Statistically significant differences were observed between the experimental subjects compared to controls (p < 0.01). The mean values ± SD of CA in experimental and control subjects in group I was 8.25 ± 3.27 for more than 10 years exposure group and 4.68 ± 2.64 for less 10 years exposure group respectively; in Group II it was 9.92 ± 4.08 (> 10 years exposure) and 7.19 ± 2.73 (< 10 years exposure), respectively. Statistically significant results were obtained in experimental subjects compared to control groups (p < 0.01), confirmed by chi-square test. Users with snuff habit having increased percentage of CA and MN cells when compared to users with out snuffing habit. In Group II the mean percentages of MN cells were 2.97 ± 0.97 for more than 10 years habitual users with snuffing and 1.93 ± 0.75 for less than 10 years of exposure. Discussion India has the largest betel quid consuming population in the world. A large-scale survey reported an overall 33.0% of betel quid chewing in Mumbai, India. The prevalence of oral cancer was also noted to be high in India16. Similarly, in Karachi of Pakistan, there is a high prevalence of betel quid chewing and also a high prevalence of oral cancer17. The habit of chewing tobacco is increasing because of its free availability, cheaper cost and increasing education about well established hazards of smoking. Studies have confirmed that use of tobacco leaf along with betel quid is as harmful as smoked tobacco18. Gajalakshmi et al. 19 conducted a large case-control study in Chennai and reported that tobacco is a major risk factor for mortality. A mixture of betel leaf, areca nut and tobacco chewing addiction is frequent in southern parts of India. Smokeless tobacco products including chewing and/or snuffing are believed to face less cancer risk than smokers, but are still at greater risk than people who do not use tobacco products20. In order to elicit the above issues, the present study has been carried out to determine the cytogenetic damage in betel leaf, areca nut and tobacco users in Coimbatore city. MN and CA have for many years been applied as biomarkers of genotoxic exposure and early effects of genotoxic carcinogens21-22. The MN test has received increasing attention as a simple and sensitive short-term assay for the detection of environmental genotoxicants23. The evaluation of cytogenetic damage performed in the present study helps understanding the health hazards as well as the cancer risk involved in using them. The present data shows an increased number of CA and MN in the users with snuffing compared to users and controls. Chromosomal instability has been described in many human dysplastic lesions and is considered a primary event in neoplastic transformation as well as a marker of progression to cancer24-25. A significant increase in the mortality ratio for all types of cancer in subjects with increased levels of CA in their lymphocytes has been found26-27. The present study confirmed that duration of exposure to smokeless tobacco plays an important role in genetic damage. While our previous study on micronucleus was based on the buccal cells among a mixture of betel leaf, areca nut and tobacco chewing population with smoking gave a significant increase in genetic damage28. The present control group shows a minimum number of MN and CA when compared to the smoke less tobacco exposed groups. The CA in controls might have been due to factors like their age, working environment and lifestyle. Several studies have found a significant influence of age on CA frequency, whereas others have found no association at all. Recently, age and lifestyle factors have been found to be strongly associated with the frequency of CA measured by the chromosome painting technique29. CA and MN assay is a cost-effective procedure, accurate and easy to carry out for population-based studies. Furthermore, in vivo evaluations allow for considering the influence of the individual susceptibility in screened humans. Our previous reports have established that buccal cells are useful not only for characterizing the molecular mechanisms underlying tobacco-associated oral cancers, but also as exfoliative cells that express diverse changes that appear promising as candidate biomarkers for the early detection of oral cancer30. In the present study rather than directly assessing the MN present in the buccal cells, by analyzing peripheral blood leucocytes indirectly confirm the genomic instability. In conclusion, betel quid chewing in southern parts of India is the most prevalent among construction and agricultural workers over many years. Betel quid usage is strongly associated with tobacco snuffing in most of the construction workers. Efforts to reduce habitual betel quid consumption and snuffing might be of benefit in reduction of oral cancer incidence. A strong and intriguing relation between the use of betel quid chewing and tobacco snuffing was found to be a public health hazard. Acknowledgement The authors are grateful to the Authorities of Karpagam University, Coimbatore, Tamil Nadu, South India for the use of facilities and encouragement and we also extend our thanks to all the participants of this study. References
Copyright 2009 - Braz J Oral Sci The following images related to this document are available:Photo images[os09030t2.jpg] [os09030t1.jpg] |
| |||||||||

{kind=link}
{kind=link}