 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Braz J Oral Sci, Vol. 8, No. 3, July-September, 2009, pp. 149-153 Evaluation of palatal arches made from low-nickel stainless steel wire Rogério Lacerda dos Santos1, Matheus Melo Pithon1, Margareth Maria Gomes de Souza2, Ana Maria Bolognese3, Mônica Tirre de Souza Araújo2 1 DDS, MS, PhD student in Orthodontics, Federal University
of Rio de Janeiro, Brazil
Correspondence to: Rogério Lacerda dos Santos Praça José Batista de Freitas, 78, sala 102, centro Nova Serrana- MG - Brazil CEP 35519-000 E-mail: lacerdaorto@hotmail.com or lacerdaorto@bol.com.br Received for publication: August 5, 2009 Code Number: os09031 Abstract Aim: To test the hypothesis that there is no difference between
stainless steel wires and low-nickel stainless steel ones regarding their mechanical
behavior. Force, resilience and elasticity modulus produced by Coffin, "W" arch,
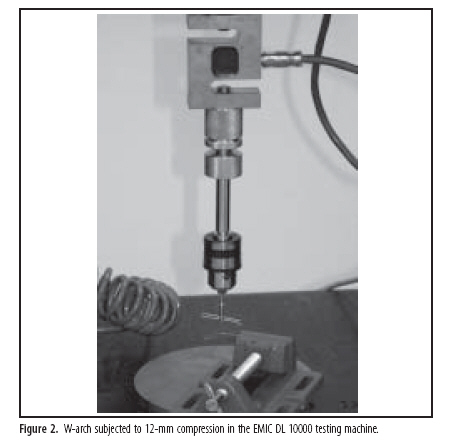
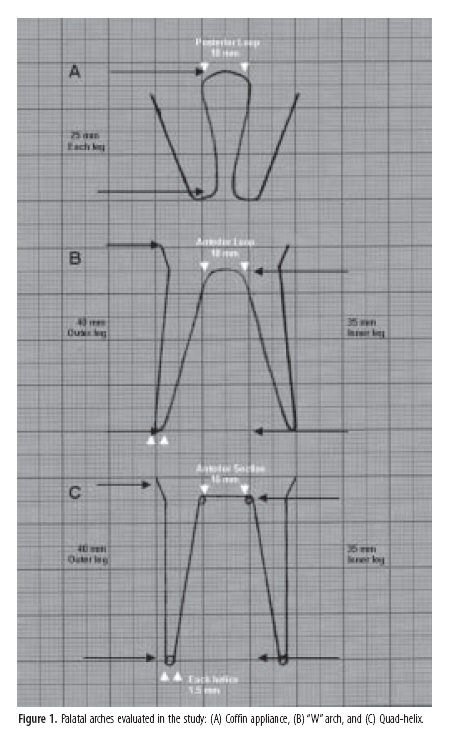
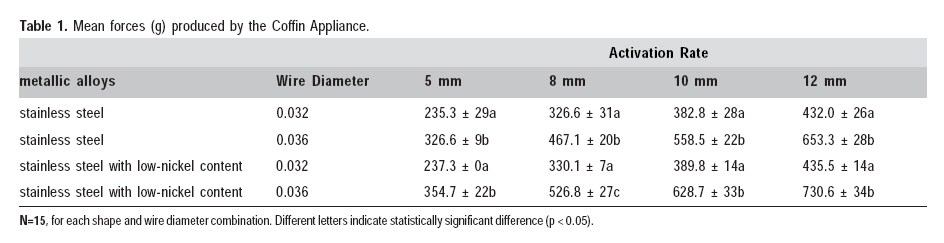
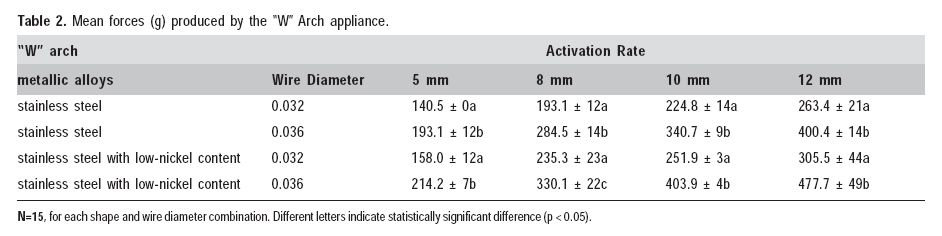
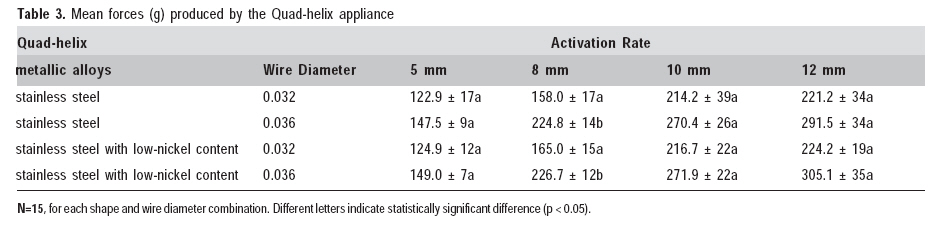
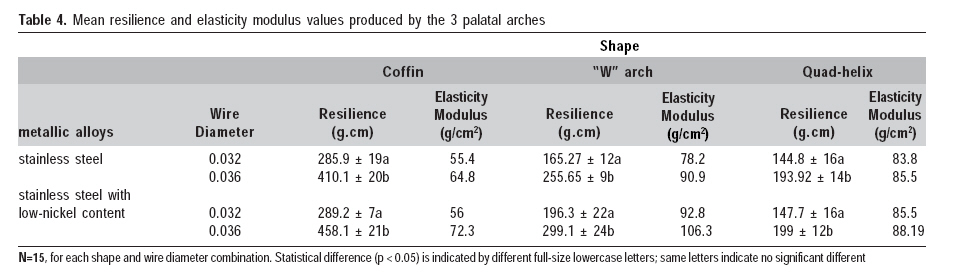
and Quad-helix appliances made of 0.032-inch and 0.036-inch wires were evaluated. Keywords: orthodontics, malocclusion, nickel, hypersensitivity. Introduction In daily orthodontic practice, a variety of metallic alloys, such as stainless steel, cobalt-chromium, nickel titanium and beta-titanium, are used, and the majority of these contain nickel1. The percentage of nickel in the appliances, auxiliaries, and accesories used in orthodontics ranges from 8% (as in stainless steel) to more than 50% (as in the nickel-titanium alloys2. The most common types of stainless steel alloys used in orthodontics are the types 302 and 304 according to the American Institute of Steel and Iron (AISI), consisting of approximately 18% of chrome and 8% of nickel, and being represented by the 18-8 stainless steel group. Leaching of these metallic components may be a potential trigger to an allergic reaction. Nickel is a strong immunologic sensitizer and may result in contact hypersensitivity3. Tissue reactions may consist of intraoral diffuse red zones, blisters and ulcerations extending to the perioral area, and eczematic and urticarial reactions of the face or more distant skin areas4. In order to solve this problem, low-nickel-content stainless steel alloys have been increasingly used for making orthodontic appliances, including the expanders usually employed to correct posterior crossbite in those cases of deciduous, mixed, and permanent dentitions as an alternative treatment for those patients who are potentially allergic to nickel. Coffin, "W" arch, and quad-helix arches are among the most common appliances used to correct the crossbite5-7 in deciduous and mixed. The Coffin appliance, designed by Walter Coffin in 1881, was originally used in removable plates aimed at expanding the constricted dental arches, and its clinical application is still often recommended7-8. The "W" arch is indeed an evolution of the Coffin appliance that resulted in changes in shape and dimension, besides being used with fixed anchorage. In order to improve the flexibility and to release the force slightly and continuously, coil springs had been initially placed at the posterior segment of the palatal arch (double-helix). Later, two more coil springs were also placed at the anterior part of the arch, thus resulting in the quad-helix appliance5,8-9. Graber10 have stated that 400 g is the lowest orthopedic force needed to achieve an effect on the maxillary arch. Conversely, the correction of posterior crossbite requires orthodontic forces, and Jarabak and Fizzel11 recommend ideal force levels for each group of teeth, that is, 250 g to move the upper molar. The aim of the present study was to test the hypothesis that there is no difference between stainless steel wires and low-nickel stainless steel wires regarding their mechanical behavior. For such purpose, force, resilience and elasticity modulus produced by three different types of expander appliances employed for crossbite correction were assessed and the ideal levels of activation regarding each appliance determined. Material and methods A total of 180 appliances were tested using two sizes of wire in 3 configurations, including two types of stainless steel alloys, one with nickel and chrome (Morelli, Sorocaba, SP, Brazil) and another with low-nickel content (less than 0.2%) (Morelli). Fifteen Coffin appliances were made of 0.032-inch stainless steel wire and 15 more were made of 0.036-inch stainless steel wire using each type of metal alloy. The Coffin appliance had two 25-mm legs and a posterior loop that measured 10 mm (Figure 1A). Fifteen Porter-W appliances were made of 0.032-inch stainless steel wire and more 15 were made of 0.036-inch stainless steel wire using each type of metal alloy. The Porter-W arch (Figure 1B) had two 40-mm outer legs, two 35-mm inner legs, and the anterior section was 10 mm. Fifteen quad-helix appliances were made of 0.032-inch stainless steel wire and 15 were made of 0.036-inch stainless steel wire using each type of metal alloy. The quad-helix had the same dimensions as the Porter-W arch, but had four 1.5-mm diameter helices that were incorporated in the arches (Figure 1C). The specimens were manufactured by the same professional, using a template with standardized intercanine and intermolar distances. A split mandrel adapted for the experiment was mounted upon the upper part of the machine in order to allow an application of force to the central part of the appliance external leg. Another device served as a base for fixing the other leg outside and keeping it in the same perpendicular position during the tests, thus avoiding momentum creation (Figure 2). Each sample was first activated at 12 mm and then submitted in sequence to compression trials in the EMIC DL 10000 testing machine (São José dos Pinhais, PR, Brazil) (Figure 2), using the Mtest program 1.0 version, at a speed of 5 mm/min12. The Mtest program provided the force and resilience means produced by 5, 8, 10, and 12 mm activation, as well as the mechanical behavior graph of each appliance in this activation index. The elasticity modulus was calculated based on the arch dimensions, the wire diameter, and the force means obtained for each appliance shape. Analysis of variance with multiple comparisons and Tukey's test were used (P < 0.05) for analyzing statistically force and resilience data. Results Force (Tables 1, 2, 3), resilience and elasticity modulus (Table 4) increased proportionally to the activation increases. In addition, the groups using the 0.036-inch wire presented statistically (P < .05) higher levels of force and resiliency when compared to the arches using the 0.032-inch wire. On average, the Coffin (Table 1) arch produced the highest levels of force, followed by the "W" arch (Table 2), and the quad-helix showed the lowest values (Table 3). Coffin appliances also showed higher resilience comparing to the others (Table 4). The "W" arches showed higher force and resilience than the quad-helix using the same diameter wire. It was observed statistically significant differences between the wire thicknesses for the same type of appliance (P < 0.05) and same metal alloys. of the mean elasticity modulus values were higher in the Coffin group, followed by the "W" arch and then the quad-helix. The larger the diameter of wire, the larger was the elasticity modulus, even in appliances with the same shape (Table 4). With respect to the wire thickness, no statistically significant difference (P >0.05) was observed between metal alloys regardless of the type of appliance. However, Porter-W and quad-helix appliances showed statistically significant differences regarding 0.032-inch and 0.036-inch wires for both types of metal alloy. Discussion One can observe statistically significant differences between Coffin and "W" arch appliances regarding the wire thickness using both types of metal alloy in all activations (5, 8, 10, and 12-mm), except for 8-mm activation in appliances made of 0.036-inch wire (Tables 1 and 2). Quad-helix appliances showed statistically significant difference regarding the wire thickness for an 8-mm activation using both types of metal alloy, but no statistically significant differences were observed for 5, 10, and 12-mm activations between stainless steel and low-nickel stainless steel alloys (Table 3). The low-nickel stainless steel alloy used for making these appliances can promote forces different from those of stainless steel alloy. Therefore, knowing the behavior of both these alloys allows us to determine the optimal activation levels for orthodontic or orthopedic movement regarding each type of appliance. The mean force values increased proportionally to the activation, corroborating that the appliances worked in the elastic phase, in which deformation is proportional to force. Resilience is the property associated with the capacity of absorbing and releasing energy; thus, the higher the resilience, the more continuous the force13. Studies have reported different shapes of palatal arches to correct posterior dental crossbites7,9,14. In the present study, different appliances provided distinct mechanical properties, indicating the need for acquiring knowledge of the performance of the appliance to be chosen. In addition, it is important to identify the etiology of such malocclusion and to determine the ideal force for each treatment15. The movement of a single molar might use 250 g11, but orthopedic effects are noted in primary and mixed dentition with forces higher than 400 g10. Orthodontic force is capable of moving teeth, whereas orthopedic forces cause bone movement. For orthodontic movement, light and continued forces are preferable because they promote direct, frontal absorption that results consequently in dental movement, whereas greater forces can stimulate indirect absorption at a given distance. As W-arch and quad-helix appliances are made of a greater amount of wire, they become more flexible and consequently are more indicated for orthodontic movement. On the other hand, the Coffin appliances incorporates fewer amount of wire compared to other ones and as a result are less flexible, being usually employed for bone movement associated with dental movement. According to Adams7, the amount of activation in the Coffin appliance depends on the length and diameter of the arch and the number of teeth to be moved. An activation range from 2 to 4 mm using a 0.050-inch wire has been proposed as being sufficient at the beginning. If new adjustments are necessary, they can be made afterwards. In the present study, 5-mm activation yielded results similar to those from Adams, who used 4-mm activations. However, the need to use a thinner wire diameter is also suggested when the etiology is a dental abnormality. Proffit6 suggested that the success of removable appliances depends on the patient's co-operation and on controlling the force of the appliance. He analyzed the use of the "W" arch and recommended 3 or 4 mm of activation as adequate levels of force when using a 0.036-inch wire. Other studies such as that by Urbaniak, et al.14 showed that the force produced by the quad-helix activation is influenced by the size and wire diameter of the appliance. This study reported that the amount of wire used in the palatal arch and the force are inversely proportional, whereas the wire diameter is directly proportional to the force. Other studies referring to the quad-helix appliance5,8-9 suggested the use of a force of approximately 400 g for an activation of 8 mm. According to the present study, the most appropriate force was the one obtained with a "W" arch using a 0.036-inch wire with 12-mm activation for stainless steel alloy and 10-mm activation for low-nickel stainless steel alloy. Such a difference might be caused by differences in the size of the appliances, wire diameter, and metal alloy used14. In face of the results obtained from this study, the crossbite of a single molar or a group of a few teeth is appropriately treated with a 0.036-inch quad-helix or a 0.032-inch "W" arch using 10 to 12-mm activation. A 0.032-ich quad-helix with 8-mm activation for both metal alloys provides a very light force and can be used to correct the crossbite of a single tooth. In this way, the results suggest that W-arch and quad-helix appliances using these activations would be appropriate to obtain forces usually indicated to induce orthodontic tooth movement. When a mild orthopedic effect is expected during the deciduous and mixed dentition, a 0.036-inch "W" arch with 12-mm activation for stainless steel alloy and 10-mm activation for low-nickel stainless steel alloy appears to be the best choice. The Coffin appliance had the highest forces released, thus suggesting that the orthopedic effects can be reached in co-operative patients or in fixed appliances using this arch shape in either 0.036-inch wires with 8-m to 10-m activation for stainless steel alloy or with 5-mm to 8-mm activation for low-nickel stainless steel alloy. Nickel is known to be a common cause of contact allergies and hypersensitivity reactions16-18. It is estimated that 4.5% to 28.5% of the population have hypersensitivity to nickel3,16. Females have been reported to have a much higher prevalence than males (10:10)16. Even though, the presence of metal ions, such as nickel, has been associated with hypersensitivity reactions in orthodontics19. The clinical manifestations of nickel hypersensitivity are easy to diagnose, any intraoral or extraoral appliances containing nickel must be removed until after the dermal or mucosal signs of adverse reactions have healed completely2. History of allergy should be considered a predictive factor of clinical manifestations of nickel hypersensitivity20. Instead of using intra- or extraoral appliances containing nickel, it is suggested that such devices be replaced by brackets and wires made of stainless steel alloys with no or low-nickel content. The wires made of stainless steel alloys with low-nickel content are an option the orthodontist can consider for patients with history of nickel hypersensitivity, however attention should be paid to the activation to be used for appliances made from this wire. In the present study the appliances made of low-nickel stainless steel wire showed high force released and resilience, and this can influence significantly the treatment as a greater dental response can be obtained. In conclusion, appliances made of low-nickel stainless steel alloy had higher release of force, resilience and elasticity modulus compared to those made of stainless steel alloy. The three types of appliances evaluated can produce adequate forces for orthodontic treatment as long as their clinical application is correctly planned. References:
Copyright 2009 - Braz J Oral Sci The following images related to this document are available:Photo images[os09031t4.jpg] [os09031t3.jpg] [os09031f2.jpg] [os09031t1.jpg] [os09031t2.jpg] [os09031f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}