 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Braz J Oral Sci, Vol. 8, No. 3, July-September, 2009, pp. 154-158 Clinical performance of indirect esthetic inlays and onlays for posterior teeth after 40 months Regina Helena Barbosa Tavares Silva1, Ana Paula Dias Ribeiro2, Alma Blacida Conception Elisaur Catirze 3, Lígia Antunes Pereira Pinelli2, Laisa Maria Grassi Fais2 1 DDS, MS, PhD, Professor, Department of Dental Materials
and Prosthodontics, São Paulo State University, Araraquara School
of Dentistry, Araraquara, SP, Brazil.
Correspondence to: Regina Helena Barbosa Tavares da Silva, Rua Humaitá, 1680 Araraquara-SP Brazil, Phone: +55-16- 3301-6409. Fax: +55-16- 3301-6406 E-mail: reginats@foar.unesp.br Received for publication: June 22, 2009 Code Number: os09032 Abstract Aim: Searches for biocompatible restorative materials with
better clinical properties, longevity and esthetics have resulted in the development
of several ceramic types. The aim of this study was to evaluate the performance
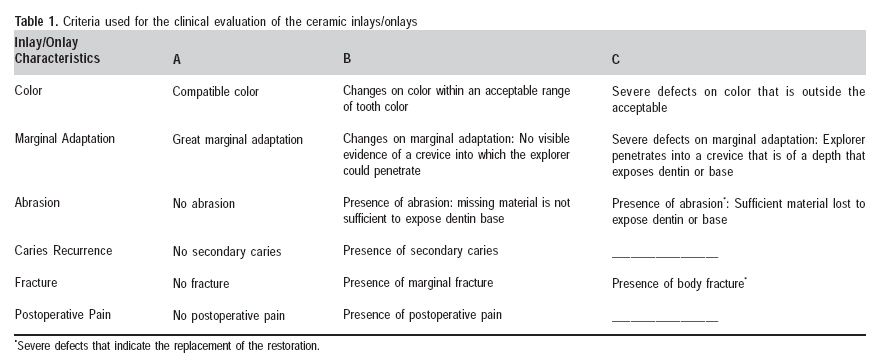
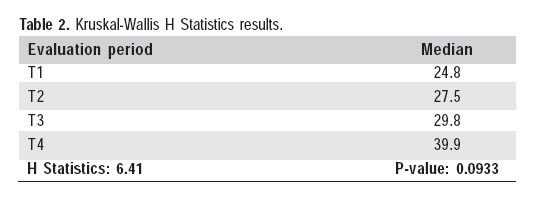
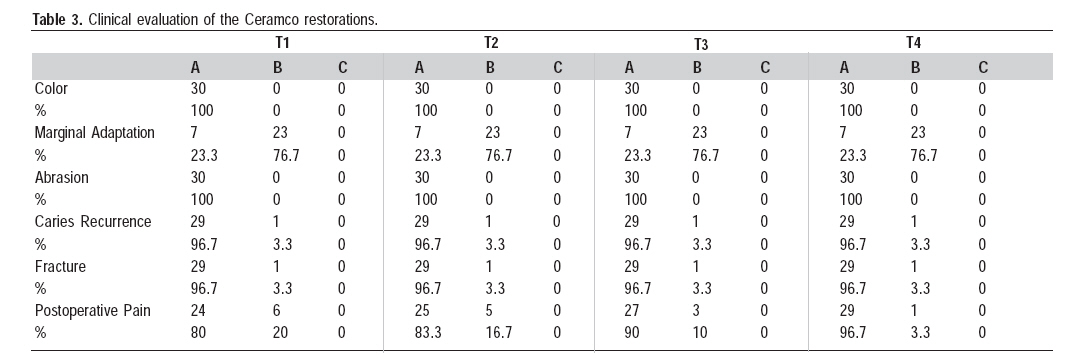
of Ceramco inlays and onlays over 40 months. Keywords: dental materials, inlays, onlays, clinical trial Introduction The search for an ideal restoration has led to the development of several restorative techniques and materials. Although metallic alloys were used due to their favorable physicomechanical properties1-2, much effort has been made to develop materials with better performance to fulfill clinical requirements3-5 and meet the patients' esthetic expectations5. Restorations with similar characteristics to those of the dental structures, such as color, brightness, and superficial texture, associated to low cost and high durability, are often the patients' desire. The most recent results of this evolution are the composite materials and the non metallic ceramic restorations4,6-7. Ceramic materials are brittle, with relatively high compressive strength, but present low flexural strength and fracture toughness8-9. Nevertheless, the main disadvantage of this material is the high potential of wearing the enamel or resin restoration of the antagonist teeth. The new ceramic compositions have demonstrated an abrading potential of dental enamel similar to that of natural teeth, which means that they have less aggressive behavior. Moreover, they are biocompatible with the pulp and periodontal tissues, present less biofilm accumulation than the enamel, and transfer less heat and electric current when compared to metallic alloy restorations3. The restorative technique with dental ceramics has also been enhanced significantly and had its acceptance increased due to the advancement of adhesive systems. The advent of dual cure resin cements associated with recent dental adhesives represent a significant improvement in cement adhesion, thus optimizing the retention and stability of ceramic restorations3,5,8,10-11. Despite of all this advantages, the longevity and success of this type of restoration depend on the correct indication, clinical experience of the operator and an accurate work of the laboratory technician12-14. Since only few long-term clinical studies exist under controlled conditions15-17, it seemed interesting to assess the longitudinal performance of ceramic inlays/onlays restorations over 40 months using a direct evaluation. This study is expected to contribute to a better indication of dental ceramics aiming to contribute to return teeth to a normal condition and promote their reintegration in the stomatognathic system. Material and methods Ten undergraduate dental students from the Araraquara School of Dentistry, São Paulo State University aged 18 to 21 years were select for this study. The volunteers should have almost similar buccal and dental conditions, habits, diet, age and indication for an adhesive restoration. Patients with parafunctional habits, poor hygiene and periodontal conditions were excluded from the selected group. The patients were informed of the research protocol and agreed to attend a recall program of 40 months. Thirty ceramic restorations (12 onlays and 18 inlays) (Dentsply Ceramco, York, PA, USA) were placed in 6 maxillary premolars, 8 maxillary molars, 4 mandibular premolars and 12 mandibular molars. The cavities included O (12), MO (4), OD (3), MOD (6), MOL (1), MODV (2) and MODL (2) preparations. A calibrated professional prepared the posterior teeth for indirect ceramic inlay/onlay restorations using tapered and round diamond burs (KG Sorensen Indústria e Comércio Ltda., Barueri, SP, Brazil). The carious tissue was removed with excavator and the dentin-pulp complex was protected with calcium hydroxide (Hydro C; Dentsply, RJ, Brazil) and glass ionomer cements (Vitrebond; 3M ESPE, Sumaré, SP, Brazil) in deep cavities. All cavities were prepared according to the established principles for adhesive inlays/onlays, which included an occlusal reduction of 1.5 to 2.0 mm, with a wide isthmus rounded internal angles and the axial wall with 1.5 mm of thickness. Gingival margins were prepared entirely in enamel whenever possible at the cementoenamel junction18. Custom trays were used for the 1-step full-arch impressions using vinyl polysiloxane (Reprosil Dentsply, Petrópolis, RJ, Brazil) and the antagonist impression was made with alginate compound (Jeltrate; Indústria e Comércio Ltda.). The casts were placed on an adjustable articulator and all the inlays and onlays fabricated by a dental technician according to the manufacturer's instructions. The restorations were evaluated and, when necessary, adjustments were made with diamonds burs (KG Sorensen Indústria e Comércio Ltda.) and fine-grain diamond discs. The adjusted restorations were polished with aluminum oxide discs (Sof-Lex, 3M, Sumaré, SP, Brazil), Enhance abrasive rubbers (Denstply Indústria e Comércio Ltda.) and pumice slurry. Under rubber dam, the enamel was etched with 37% phosphoric acid gel (Scotchbond; 3M ESPE) for 30 s and the remaining dentin was etched for 10 s. Afterwards, Syntac Primer (Ivoclar Vivadent, São Paulo, SP, Brazil) was a applied for 15 s on the dentin and the excess was gently removed with air syringe. Then, Syntac Adhesive was applied for 10 s on the cavity and dried thoroughly with blown air. The restorations were cemented with Dual Cement according to the manufacturer's instructions (Ivoclar Vivadent). Polymerization was performed by the application of a halogen light (Heliomat-Vivadent, São Paulo, SP, Brazil) for 20 s in each tooth face with a fluence rate of 500 mW/cm2. The occlusal contacts were checked and, when necessary, teeth were adjusted using diamond rotary cutting instruments. Final polishing was conducted using F and FF diamond finishing rotary cutting instruments (KG Sorensen Indústria e Comércio Ltda.), and rubbers and felt discs with polishing diamond slurry. All restorations were clinically evaluated on four recalls during 40 months. The periods were: T1 (10 months), T2 (20 months), T3 (30 months) and T4 (40 months). All the restorations of T0 (baseline) were considered satisfactory and received high scores for each variable. The photographs were made with a Dental Eye II camera (Yashica, Sorocaba, SP, Brazil) with the maximum approach only to illustrate the general condition of each restoration. Clinical evaluations were made by a calibrated professional using an explorer and plain clinical mirror, with the tooth and the restoration previously dried. The variables studied were: color, marginal adaptation, abrasion, caries recurrence, fracture and postoperative pain. All restorations received an adapted score following the description of Cvar and Ryge criteria19 (Table 1). Results The 40-month recall rate was 100% on clinical re-evaluations. In order to evaluate the clinical performance of Ceramco inlays/onlays during the 40 months, Kruskal-Wallis H statistics were applied (p=0.05). No statistically significant difference was observed between the periods (T1, T2, T3, T4) (Table 2). The outcomes observed in clinical evaluations for the Ceramco inlays/onlays during T1, T2, T3 and T4 periods are presented in Table 3. During the 40-month evaluation period, no color alteration or abrasion occurred. Fracture and secondary caries occurred in only 1 restoration, corresponding to 3.3%, which maintain in 96.7% the success index. Postoperative pain was present in 20% of the cases, in T1 period of evaluation. However, postoperative pain was not present on T4, which represents a success index of 100% on that period. The same success level was not achieved for the marginal adaptation. Twenty-three restorations (76.7%) presented alterations in the restoration/tooth interface. These alterations occurred in the first months of use, and the same level was maintained after the first time of evaluation (T1) until the T4 analysis. Figures 1 and 2 show the general condition of restorations in T0 and T4. Discussion The evaluation of the clinical performance of the Ceramco restorative ceramic system within a 40-month period showed a high success rate for most analyzed variables (color, marginal adaptation, abrasion, secondary caries, fracture and postoperative pain), which is in accordance with the literature20-21. Although this system has a relatively complex technique and high cost, it has excellent esthetic results and mechanical resistance, in addition to presenting biocompatibility when compared to other restorative materials14,22. In recent years, these features have contributed to the high-quality performance of ceramic restoration, which leads to good acceptance by the professionals. In addition to these successful rates, the longevity of ceramic restorations is subjected to many factors that can act in a positive or negative form and should be carefully controlled. On these concerns, factors that have the major occurrence were fracture of the restorations, hypersensitivity, loss of retention and fracture of the restored tooth15. Molin and Karlson21 reported that these factors can be originated from misfits, occlusal forces, incorrect cavity designs and imperfections in the cementation technique. Among the 30 (33%) restorations evaluated in this clinical study, fracture occurred in only one during the analyzed period. Friability is an inherent characteristic of dental ceramics and it has direct influence on their durability21,23. Ceramic fractures have been related to inadequate tooth preparation, occlusal adjustments disrupting the surface and faulty material. Tagtekin et al.24 (2009) found that fractures in ceramic restorations usually occur during the first 6 or 8 months, and the results of the present study agree with this evidence. The fracture observed in our study could possibly be due to the occlusal adjustments done after cementation, although the other restorations were also adjusted. These adjustments might have caused disruption of the superficial glazed layer, generating micro-fractures that became points of crack propagation9,15-16,25. Some special care should be necessary to deal with this problem as an occlusal adjustment of the restoration integrated with a balanced occlusion, an adequate preparation and adhesion technique for cementation. The use of resin cement provided a better integration between tooth and restoration, transferring the external forces to the dentin. Therefore, an increase in ceramic resistance occurred, probably resulting in enhanced clinical durability of these restorations5. The results of this study clearly demonstrate that the major problem is situated at the margin between the restoration and dental structure. Kramer and Frankenberger12 reported that every clinical trial assessing ceramic inlays revealed a certain deterioration of marginal quality. This might be caused by insufficient bonding to enamel or degradation of the luting agent caused by fatigue. Therefore, it is necessary an adaptation with the dental structure as good as possible for these restorations, including edges and external cavosurface margins5. The negative results observed for marginal adaptation occurred in the first months, and showed a tendency to keep the same level (76.7%) until the final analysis (40 months). This fact clearly demonstrates that the main concern with this type of restoration must be the initial adaptation and the friability of ceramic material at the cementation moment and the first months of use, as well as for the material and technique used to cement these restorations26. These results were also observed in other clinical studies21,27 where the marginal adaptation was the factor that presented more alteration for indirect ceramic restoration. However, Lange and Pfeiffer28 showed that 93% of the ceramic inlays received score "A" for marginal adaptation after 57 months of evaluation, and the other 7% did not need replacement. The union imperfection can be explained by the incomplete polymerization of the resinous cement, by the low resistance of some cements, lack of acid and silane treatment on the internal surface of the restoration, absence of an adhesive agent, and/or by the possible fatigue that occurs in the adhesive agent after long periods of clinical use and action of occlusal loads, mainly in patients with bruxism3. Postoperative pain was the second more incident alteration. Ceramic postoperative hypersensitivity has been initially reported to be problematic due to incomplete sealed of dentin or detachment between material and dentin12. This was a common occurrence in the majority of the cases, is a transitory characteristic and it is directly related to the wet technique of dentin hybridization, which was used in this study. The need of restoration replacement is rare, similar to what occurred in this study29. One limitation of the present study may be the fact that probably the period of 40 months was not sufficient for the appearance of significant clinical alterations. However, in recent studies18,24,28 a great clinical performance of ceramic inlays/onlays was observed at longer periods of evaluation. Finally, it might be considered that the good results were positively influenced by the selected patients. Nevertheless, it can be noticed that, although there were not statistically significant results, there was a small tendency of deterioration of the restorations with time. This shows that long-term analyses could probably indicate critical alterations that require the restoration substitution15,27. In spite of the positive results obtained in the present study, long-term clinical investigations are needed to obtain in situ information on the performance of the ceramic materials22,30-31. It is also necessary to have studies and improvements on the tooth/restoration interface, as the clinical success with ceramic inlays/onlays depends on the ability to develop a reliable bond of the composite to dental tissues. This study evaluated 30 Ceramco ceramic inlays and onlays and none of them showed any alteration that could indicate their replacement, although there was a moderated failure of marginal adaptation. Within the limitations of the design and the evaluation time of this investigation, this restoration technique seems clinically acceptable as an esthetic and conservative treatment method for molar and premolar restorations. References
Copyright 2009 - Braz J Oral Sci The following images related to this document are available:Photo images[os09032f2.jpg] [os09032f1.jpg] [os09032t1.jpg] [os09032t3.jpg] [os09032t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}