 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Braz J Oral Sci, Vol. 8, No. 3, July-September, 2009, pp. 159-162 Complication of local dental anesthesia - a broken needle in the pterygomandibular space Bruno Ramos Chrcanovic1, Djalma Cordeiro Menezes Junior1, Antônio Luis Neto Custódio2 1 DDS, Department of Oral and Maxillofacial Surgery,
Pontifical Catholic University of Minas Gerais, Brazil
Correspondence to: Bruno Ramos Chrcanovic Av. Raja Gabaglia, 1000/1209 Gutierrez Belo Horizonte, MG CEP 30441-070 Brazil. Phone: +55 31 91625090 , +55 31 32920997. E-mail: brunochrcanovic@hotmail.com Received for publication: August 19, 2009
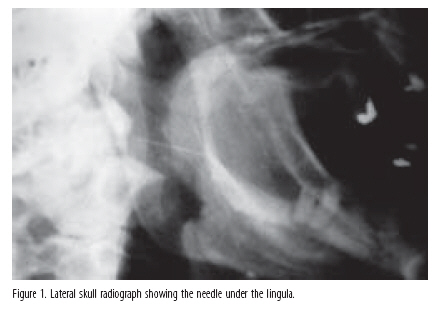
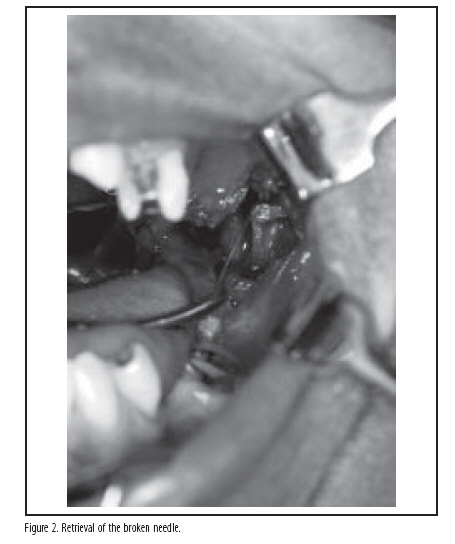
Code Number: os09033 Abstract Broken dental needles are a rare event. They are difficult to find and remove. This paper reports a case of broken needle in the pterygomandibular space. The needle was localized using plain radiograph and removed under local anesthesia and venous sedation. Preventing needle breakage is important, as it can be a traumatic experience for the patient. Practitioners should routinely inspect dental needles before administering injections and minimize the number of repeated injections using the same needle. A meticulous injection technique is imperative. If breakage occurs, immediate referral to an oral and maxillofacial surgeon is necessary. It is strongly recommended that only an oral and maxillofacial surgeon may indicate and/or perform surgery to remove the broken needle. Keywords: local anesthesia, complications, broken dental needle, pterygomandibular space. Introduction Metal instruments used in clinical practice may be subjected to considerable wear and may subsequently fracture. The removal of the broken instrument may be simple if the fractured part remains accessible, but this is not always the case. Before the advent of the disposable spiral-constructed dental needle, breakage of needles during the administration of local anesthetics was not an uncommon event. Since the introduction of disposable dental needles in the early 1960s, the frequency of needle breakage has been minimal, compared with the first quarter of this century during which time rigid, inflexible, nondisposable needles were used. Blum1 reported 100 cases of broken needles over a 14 year period from 1914 to 1928. The occurrence of needle breakage has decreased as a result of the development of stainless, flexible alloys used in modern, disposable dental needles2. Scientific advances in metallurgy and manufacturing, as well as better training of dental practitioners in how to administer anesthetic also have reduced breakage frequency3. This article reports a case of broken needle in the pterygomandibular space and discusses the modalities of localization and preventive measures. Clinical Case An 18-year-old male patient was referred by his general dentist to the Department of Oral and Maxillofacial Surgery of the Pontifical Catholic University of Minas Gerais for evaluation and removal of a fragment of 30-gauge long needle that broke during an inferior alveolar nerve block. The patient had moved his head quickly because of the sensation of shock when receiving the injection. The fragment disappeared into the tissues and the dental practitioner was unable to retrieve it. The patient was healthy with no significant medical history. Physical examination showed a moderate trismus. The patient complained of localized pain in the left pterygomandibular region and the ability to feel the broken needle during mandibular movements. Clinical intraoral examination revealed bruising in the right pterygomandibular region, but no bleeding or visible punctures wounds. A lateral skull radiograph was made (Figure 1). The lateral skull view helped us determine the needle's anterior-posterior location and also showed us its vertical relation to the teeth. It also showed that the needle was located just below the mandibular lingula. Under local anesthesia and venous sedation, a vertical incision parallel and medial to the anterior border of the ramus was made and a periosteal elevator was used to reflect the masseter and medial pterygoid musculature. During blunt dissection of the medial pterygoid muscle, the broken needle was removed (Figure 2 and 3). The postoperative period was uneventful with no evidence of trismus. Discussion Needle breakage during administration of a nerve block was a complication more frequent prior to the 1960s. This was thought to be at least partly due to the use of more rigid, non disposable needles which were subjected to repeated sterilization cycles, with attendant alterations to their physical properties during this time4. Needle fracture is now a rare complication. This is probably due to the use of modern flexible alloys in their fabrication. When fracture occurs it is usually due to the inappropriate use of short, narrow gauge needles inserted to the hub or bending before use as well as poor operator technique. Any sudden or unexpected movement by the patient and redirection of the needle against tissue resistance during administration of the injection are considered to be contributing factors to needle breakage3. The most common site for loss of a fractured needle is the pterygomandibular space during an inferior dental nerve block5-6. There is a degree of controversy over management of broken dental needles. Different authors7-9have mentioned that that removal is not necessary unless the patient developed symptoms such as pain, infection, numbness and swelling. No author has cited the possibility of formation of fibrosis in the tissues around the needle over time. Retrieval of the needle in itself can lead to neurological and tissue damage during removal9. On the other hand, many other authors6,10-14 suggested removal, fearing that the needle might migrate toward large blood vessels in the head and neck. We agree with these authors, which state that because of the fear of needle migration and also because of the medico-legal considerations, removal of the broken needle is important. It is obvious that presence of active symptoms such as pain, trismus and infection that are not alleviated by standard treatments necessitate needle removal15. There are in the literature no contraindications to perform the surgical removal under local anesthesia. A further argument in favor of removal is the possible psychological trauma to the patient that may result from the knowledge that a needle has been retained "somewhere in the throat"16. Every effort should be made to retrieve the needle immediately, if the tip is visible, using fine haemostatic tool4. Prompt retrieval is advocated to minimize symptoms of pain, dysphagia, trismus and to prevent migration of the needle and potential damage to vital structure6,9. If its tip is not visible, attempts by the general practitioner in order to recover it should be discouraged, because the needle could be pushed deeper into the tissue. It is strongly recommended that only an oral and maxillofacial surgeon may indicate and/or perform surgery to remove the broken needle. The most important aspect of the surgical technique is accurate localization of the needle. Determining the position of a broken needle in the pterygomandibular space in an anaesthetized patient is a difficult task. Several different techniques have been described including the use of metal detectors. These have been used for localization of metallic foreign bodies in the floor of the mouth17 and have been successfully used to find a broken needle in the pterygomandibular space18, although Crouse3 had a long time ago employed a metal detector but found no response on both ferrous and non-ferrous settings of the instrument and thus found it of no value. Metal detectors though are not readily available and the probe must be small enough to use in the mouth17,19. The more common method is the use of intraoperative radiographs with localizing needles20-21. Intraoperative radiographs though are difficult to obtain and prolong the procedure14. Plain radiographs are useful in confirming the presence, dimensions and approximate position of the needle. They are, however, unable to provide the accurate position of the needle and its relationship to adjacent structures. The incision and site of exploration can be determined from the information available on the CT scan. The use of 3D reformatting is especially useful. If dental restorations are present, beam-hardening artifacts can interfere with the quality of the image obtained4. The lateral skull view, used in this case, helps to determine the needle's anterior-posterior location and also shows us its vertical relation to the teeth22, although not precise in providing accurate position of the needle. Despite the availability and ease of preoperative radiograph exams, they are not sufficiently accurate because of the time period between obtaining the images and performing the surgery15. Thompson et al.14 used a simple stereotactic technique using an image intensifier and two 19-gauge venepuncture needles under general anesthesia. They stated that image intensifiers are usually readily available in theatres as they required for orthopedic and urological surgery. Nezafati and Shahi15 used C-arm digital fluoroscopy. The rapid taking and immediate reviewing of images at various angles without disturbing the reference needle, reducing radiation dose by using intensifiers and excellent image quality are the advantages of this technique, according to Nezafati and Shahi15. However, as plain radiographs, intensifiers only shows two-dimensional images, and are unable to provide the accurate position of the needle. The radiation dose increases, as one must review the image in three directions (antero-posterior, latero-lateral, cranio-caudal) in order to locate the needle precisely in the space. The use of stents has been described. Intra-operative X-rays with positioning stents are often time consuming and the discrimination between small changes in position between the two (three) localizing needles can often be poor21. Magnets are no longer used, because the manufacturing process has eliminated ferrous compounds4. Most reports have suggested the use of a vertical mucosal incision often on the medial aspect of the mandible in the area penetrated by the needle, followed by blunt supra-periosteal dissection to identify the needle6,9,13,23-24. But an initial subperiosteal dissection can help identify bony landmarks (lingula), which can be used as reference during exploration and also provides greater protection to the inferior alveolar and lingual nerves4. The inferior alveolar and lingual nerves can be injured in case of extensive dissection in a surgical retrieval of broken needles in the pterygomandibular space. The extensive dissection can also cause local pain and trismus for a considerable period. Kennett et al.16 described postoperatively considerable swelling and trismus but the patient was fit for discharge on the third postoperative day. The swelling subsided over the next week, but normal jaw opening was not present until three weeks postoperatively. Other authors reported uneventful postoperative recovery4,6,13-15,17, as also occurred in the present case. Examination of the needle before administering the injection should be standard practice among dental practitioners. If a practitioner notes any needle defects, he or she should discard the needle6. Repeated injections with the same needle should be minimized, as needle fragility and susceptibility to breakage with repeated injections has been documented12,15,21. Needles should not be bent. Using fine and short needles for inferior alveolar nerve block demands the insertion of the needle up to the hub. Long needles should be used. It is recommended to not penetrate the needle to its hub, as this is where the needle is the weakest and sight of the needle can be lost when it is buried to the hub6,16. Pietruszka et al.20 suggested that a 30-gauge needle should not be used for nerve blocking injections because it is the most narrow, least rigid needle available and also the most susceptible to breakage. Though most dentists use a 27 gauge (35 mm long) needle for administration of an inferior alveolar nerve block in an adult, there is occasionally a perception that the use of a thinner needle (30 gauge) is associated with less discomfort4. It has however, been shown that there is little difference in the pain perception between the use of 27 and 30 gauge needles25. Flanagan et al.26 also showed that there is no statistically significant difference in perceived injection pain based on needle gauge when analyzed for injection location (mandibular, maxillary posterior, maxillary anterior, and palatal), injection side, patient gender, treating dentist, or overall. These results indicate that when it comes to injection pain and needle gauge, size does not matter. Safer et al.27 assessed and compared the chemical composition, microstructure and compositional homogeneity in the alloy used by different manufacturers to make dental anesthesia needles. They found that aluminum and niobium were present in the alloy from which the needles least likely to break had been manufactured, but not in the alloy from which the most brittle needles were made. The concentrations of chromium and nickel were higher in the better quality needles. Greater needle deflection may contribute to needle breakage. Previous studies of dental needle penetration in vitro have demonstrated that the amount of deflection was inversely proportional to needle gauge; that is, thicker needles deflect less than thinner ones28. The study of Jeske and Boshart29, however, has demonstrated that a 28-gauge needle with a specially modified, nondeflecting tip produces less needle deflection than a 25-gauge needle with a conventional tip. This would suggest that a thicker needle per se will not minimize deflection (at least in the range of needle gauges used in dentistry), and that tip design is perhaps more important than gauge in reducing deflection. In this connection, another study30 demonstrated significantly less force required to insert a smaller gauge needle. This improved penetrability may contribute to decreased deflection if it allows the needle to penetrate through, rather than deflect around, various tissues encountered during a dental injection. The use of a bidirectional rotation insertion technique minimized needle deflection, resulting in a straighter tracking path for 30-, 27-, and 25-gauge dental needles, in 3 different tissue-like substances tested in the study of Hochman and Friedman31. Comparing the resistance to penetration of two types of disposable injection needles, Lehtinen30 showed that the 30-gauge needle required significantly less force (69 mN) than the 27-gauge needle (139 mN). Being required significantly less force to penetrate the tissue, the 30-gauge needle is less prone to breakage. A further consideration is the use of adequate preoperative sedation in the nervous patient, thereby minimizing the possibility of his sudden movement during the injection16. Despite the rarity of this complication and the improvement in needles, there is no room for complacency and a meticulous injection technique is imperative16. Surgeons performing the removal must not only be skilled and well-trained, but be familiar with the anatomy involved. Immediate referral to an oral and maxillofacial surgeon is necessary, as is thorough and complete documentation of the events that led to the breakage. In conclusion, preventing needle breakage is important, as it can be a traumatic experience for the patient. Practitioners should routinely inspect dental needles before administering injections and minimize the number of repeated injections using the same needle. A bidirectional rotation insertion technique should be used in order to minimize the needle deflection. It is recommended to not penetrate the needle to its hub, as this is where the needle is the weakest and sight of the needle can be lost when it is buried to the hub. A meticulous injection technique is imperative. The use of adequate preoperative sedation in the nervous patient may be considered, thereby minimizing the possibility of his sudden movement during the injection. Needle breakage rarely occurs nowadays, but when it occurs, the situation must be managed appropriately. Every effort should be made to retrieve the needle immediately, if the tip is visible. If it is not visible, the required steps include immediate referral to a maxillofacial unit, imaging to identify the position of the fragment, and surgery to remove the needle. The imaging exam should be the one available at the clinical facility, but a combination of two or more could be of great help in locating the broken needle. Surgeons performing the removal must not only be skilled and well-trained, but be familiar with the anatomy involved. It is strongly recommended that only an oral and maxillofacial surgeon may indicate and/or perform surgery to remove the broken needle. Although there is a degree of controversy over management of broken dental needles, it is the authors' opinion that every broken needle should be withdrawn. Acknowledgements We like to thank Mr. M. Ethunandan for providing us his article. References
Copyright 2009 - Braz J Oral Sci The following images related to this document are available:Photo images[os09033f3.jpg] [os09033f2.jpg] [os09033f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}