 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Braz J Oral Sci, Vol. 9, No. 3, July-September, 2010, pp. 345-350 Dental caries experience in children attending an infant oral health program Leila Maria Cesário Pereira Pinto1 , Luiz Reynaldo de Figueiredo Walter2 , Celio Percinoto3 , Cássia Cilene Dezan4 , Murilo Baena Lopes5 1DDS, MS, PhD, Professor, Department of Dentistry, University of North Parana (UNOPAR), Londrina; and Assistant Professor, Department of Oral Medicine Correspondence to: Leila Maria Cesário Pereira Pinto Av. Rio de Janeiro, 1630 - apto 502 - Centro 86.010-150 - Londrina, PR, Brazil E-mail: jolugui@sercomtel.com.br Received for publication: October 07, 2009 Accepted: July 06, 2010 Code Number: os10033 Abstract Aim: To investigate: a) caries experience in 5 year-old
children and its relationship to the caries
risk evaluation made before 1 year of age; b) compliance of parents to an
infant oral health
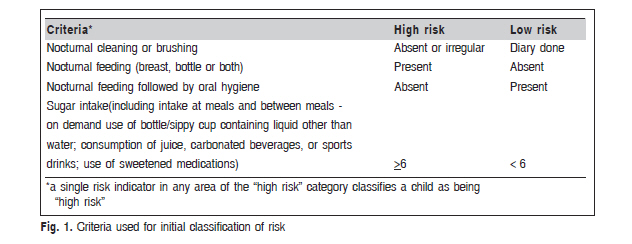
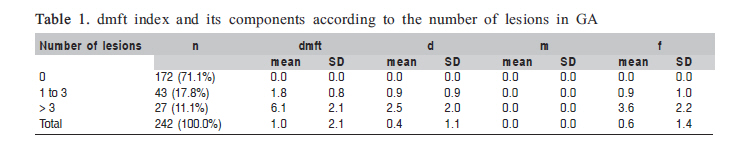
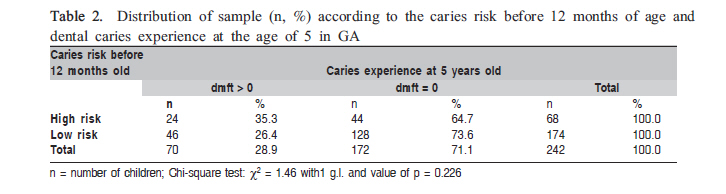
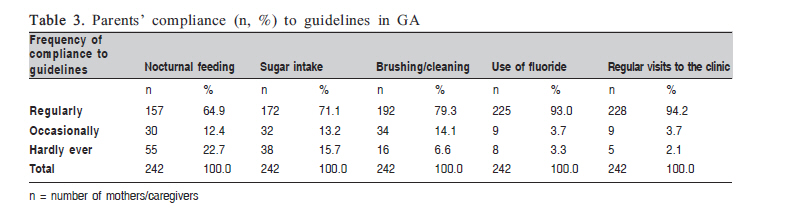
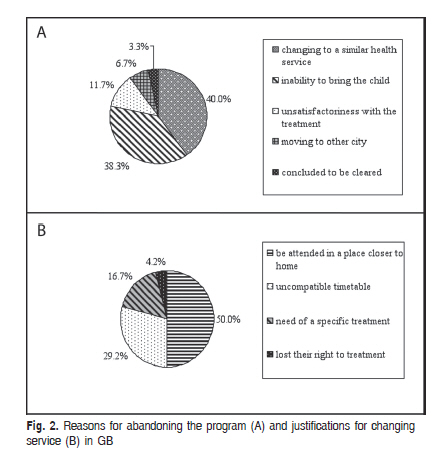
program as well as the abandonment reasons. Keywords: dental education, prevention, behavior. Introduction Prevalence, severity and level of dental caries progression have declined in the younger segment of the population of well developed countries over the last few decades1 . In Latin America and the Caribbean, the decline in the severity of the disease has been less conspicuous in preschool age children (5-6 years old) than in schoolchildren (11-13 years)2 . In the United States, the prevalence of caries has declined in 3 to 4-year-old children, but the severity of the disease has increased3 . The role of fluoride in reducing caries is well documented, but little emphasis has been given to the educational practices in dental caries prevention and control. However, since dental caries is a disease than can develop as early as the first year of life4 , parents and pediatricians should be made aware of this condition through education5 . In breast-fed infants, the guidance and motivation of parents to participate in caries prevention leads to their greater compliance in controlling the risk factors6. Moreover, as a preventive strategy, caries risk evaluations involving the identification of children with a potential for developing the disease enables dental health services to target those most in need of such services, providing greater efficiency of the procedures, appropriate levels of assistance, and economic effectiveness7. According to Twetman et al.8, the assessment of risk factors for the disease in the first year of life enhances the effectiveness of preventive procedures. The aim of this study was to investigate: a) caries experience in 5 year-old children and its relationship to the caries risk evaluation made before 1 year of age; b) compliance of parents to an infant oral health program as well as the abandonment reasons. Material and methods This transversal study included retrospective data collection. The sample comprised all children (n = 484) between 60 to 71 months old enrolled in their first year of life at a Public Infant Oral Health Program in a Brazilian city with fluoride supplied water. The project was approved by the local Ethics in Research Committee. The study began with an analysis of the patients' file to classify the children participation in the program as follow: a) those whose time interval between the last appointment and the research clinical examination did not exceed 10 months, classified as Group A (GA) "those that stayed in the program" b) those whose time interval between the last appointment and the research clinical examination exceed 10 months, classified as Group B (GB) "those that dropped out the program". The exclusion criteria were: a) refusal to participate in the survey; b) children with special needs9. Among those that stayed in the program (GA), a caries risk classification based on the patient's case history recorded on his/her file at the first appointment in the first year of life was made. Patients classified as high risk were the ones presenting one or more caries risk indicatives, while those classified as low risk were infants presenting no indicative of caries risk or those who had no teeth, even when caries risk behaviors were encountered - i.e. nocturnal feeding. Figure 1 describes the criteria adopted for caries risk classification in the first year of life. An oral examination was then carried out to diagnose dental caries in GA. All exams were carried out by a trained and qualified examiner (Kappa intra-rater index = 0.92). Ten percent of the total sample was reexamined during the data collection (Kappa = 0.98). Caries diagnostic criteria were based on the methods recommended by the World Health Organization10. The teeth were dried with a gentle air stream and illuminated with artificial light. The examination was visual, aided by a flat-surfaced dental mirror. The dmft index was used to verify the caries experience of the participants in the study10. The parents/caregivers were interviewed to ascertain their compliance to the program, evaluating their difficulty to follow the guidelines of the program. The evaluated aspects were: nocturnal feeding, sugar intake, teeth brushing, use of fluoride and regular visits to the clinic. The data were recorded according to the frequency that the parents followed the guidelines of the program - regularly (regular frequency), occasionally (irregular frequency), and hardly ever (rarely). The parents/caregivers enrolled in GB were interviewed by phone call, using a structured questionnaire to evaluate the possible cause for abandoning the program, as well as the continuity of their dental care in other locations. The data were analyzed using the statistical non-parametric chi-square test with 5% level of significance. Results The evaluation of the patient's files indicated that the total sample comprised 484 children of both genders aged 60 to 71 months, who were divided into: GA - 300 (62.0%) who stayed in the program and had been enrolled since their first year of life; GB - 184 (38.0%) children who had left the program before the case histories were evaluated for this survey. Among children belonging to GA there were 58 losses. The reasons for losses were: 2 parents/caregivers refused to participate, 39 dropped out the program without explanation while the research was being conducted, 8 were transferred to similar health services and 9 could not be encountered. The final sample of those that stayed at the program was composed by 242 children. Data about the age and number of erupted teeth registered on the patients records showed that at the first appointment: 23.8% were 6 months old or less and 76.2% were older than 6 months, 58.9% presented one or more erupted teeth and 41.1% did not. It was also observed that 85.3% had regular returns to the appointments, considered as children up to the age of 3, which time elapsed from one appointment to other did not exceeded 1 month of the scheduled appointment, and after this age, not exceeding 2 months. About children who had dropped out of the program (GB), 60 parents/caregivers could be contacted. a) Children attended the infant oral health program (GA) - Dental caries prevalence in 5 years old At the time of the clinical examination, most of the children were free of caries (71.1%). The encountered dmft was 1.0 (SD = 2.1). No dental loss due to caries was recorded, and the number of filled teeth exceeded that of decayed (Table 1). The dmft for the group of children presenting caries (n = 70) was 3.5 (SD = 2.5). - Relationship between the caries experience and the caries risk evaluation To evaluate if the caries risk indicators adopted in the program were efficient in predicting future caries lesions the sensibility and specificity of the method was calculated. The indicators adopted to determine the caries risk in the first year of life revealed low sensibility to caries experience at 5 years of age, once 34.3% (95% CI: 22.4 46.1) of the children with caries were identified as high risk at the beginning of the program. However, the specificity was high, pointing out that among the children without caries at age 5, 74.4% (95% CI: 67.6 81.2) were identified as low risk in first year. The positive predictive value of the method was low, since 35.29% (95% CI: 23.2 47.4) of the children who entered the program with high risk developed the disease, while its negative predictive value is high, because it showed that 73.6% (95% CI: 66.7 80.4) of the children who entered the program with low risk did not develop the disease. No significant associations (p>0.05) was encountered between the risk evaluation at the beginning of the program and caries experience at age of 5 (Table 2) - Compliance of parents/caregivers Sixty-two mothers (25.6%) reported having encountered some difficulty to follow the guidelines of the program, while 180 (74.4%) did not have problem. The topics of the guidelines with more frequency of "occasionally" and "hardly ever" answers involved the control of nocturnal feeding (35.1%) followed by sugar intake (28.9%) (Table 3). On the other hand, greater compliance ("regularly") was recorded for the regular visits to the clinic (94.2%) followed by the use of fluoride (93.0%). b) children that dropped out the program (GB) - Abandonment reasons to the program The most frequent reason for abandoning the program was changing to a similar health service (40.0%) in Londrina or in another city (Figure 2-A). According to the mothers' report, 50.0% of the cases were due to the need of being attended in a place closer to their homes (Figure 2-B). The current situation of dental care of those who dropped out of the program showed that 65.0% (n = 39) were still receiving dental care. Among these, 79.9% (n = 30) were in preventive treatments, 15.4% (n = 6) in restorative treatment because of dental caries and 7.7% (n = 3) in orthodontic treatment. Only 35.0% (n = 21) affirmed not to be under any kind of dental care. Discussion The program described in this paper has been operating to promote oral health for children since 1985. Inclusion criteria of the program are the age (the child must be underage of 12 months) and to be free of caries. The children are assisted from the first year of life up to the age of 71 months. The service is focused on parents' education and preventive measures for the children, which are planned according to a periodic evaluation of caries risk. Parents' education is based on a collective educational approach and an individual follow-up in order to evaluate and guide parents about their children's needs. The preventive measures applied to infants involve the removal of dental plaque and fluoride application. For the children enrolled in the program before dental eruption, the mothers behaviors and the children habits related to oral health are evaluated previously to the educative measures be performed. The parents' education and preventive measures performed at every visit to the clinic generate feedback for their children oral health improvement11. The appointments were scheduled tri-monthly to the child up to 3 years old, and at a 6-month interval thereafter. There is some flexibility in the schedule of the dental appointments to assure parental compliance to the program. The Nucleus of Dentistry for Babies is funded by the SUS (Brazilian Public Health System) and integrated to the Municipal Health System of Londrina, state of Parana, Brazil. It provides health services to all socioeconomic levels of the local and regional community, with more than 17,000 infants enrolled in the program. The dmft found in 5-year-old children participating in the program (1.0, SD = 2.1) was lower than that reported for Brazil (2.8, SD = 3.5), according to an epidemiological survey conducted by the SB Brazil 2003 project12. The results of the dmft index by macro-region in Brazil were also higher than those of the program (North 3.2, SD = 3.6; Northeast 3.2, SD = 3.7; Southeast 2.5, SD = 3.3; South 2.6, SD = 3.4; Mid-West 2.7, SD = 3.3)12. Although the living conditions are different, the number of caries-free children (71.1%) was similar to that found in oral health programs in well-developed countries such as Finland13, Denmark14 and France15. These findings are also in agreement with those of Ismail et al.16, who reported a significant correlation between regular visits to the dentist and low caries indices. In addition, the results confirm the importance of oral health promotion programs as an effective mean to facilitate the adoption of healthy behaviors and, hence, better health for children6,17-21. The successful promotion of health is associated with the development of different parental skills allied to the guidelines offered by the health services and the child's regular visits to the clinic17. The method employed in the caries risk evaluation in the first year of life revealed a low positive predictive and a high negative predictive value for dental caries experience at the age of 5. In this way, the findings of this survey confirm the need for establishing specific protocols for risk evaluation in different age groups, since children's habits are being formed and, if inappropriately established, they become resistant to changes. Additionally, the importance of determining caries risk in preventive treatment planning are pointed and are in agreement with data reported in the literature, which identify risk evaluation as the key to a successful prediction of disease in all age groups13,22-23. The specificity of the method used in this study was good. The test demonstrated that among the children that were classified as low risk at the beginning of the program, 74.4% were free of caries. On the other hand, the sensibility was low, once from those children that were diagnosed as high risk at the beginning of the program only 34.3% developed caries lesions. The low sensibility may be related to the interposal of educative and preventive measures to reverse the caries risk from high to low since the first patients' appointment to the clinical examination at 5 years old. Legal and ethical aspects must be considered in this situation because the dentist is supposed to promptly advise the parents/caregivers when a patient is diagnosed as high caries risk. Another element to be considered is the major dietary changes occurring at the period of transition from breast or bottle-feeding to familiarly diet in childhood. An obstacle to the clinical implementation of caries risk evaluation is the lack of studies investigating how the application of the risk evaluation methodology affects future oral health24. Moreover, there is no single risk factor or combination of factors that has reached high positive and negative predictive values25, although previous caries experience is still the best indicator of the future development of caries. However, the caries experience is not commonly used with children because it is important to determine the risk of caries before the disease manifest24, especially in infants (1-23 months). The parents' motivation through personalized guidelines shows a stronger effect in caries prevention compared to traditional health education6. However, this survey revealed that even with the personalized educational practices provided by the program, 25.6% of the parents reported finding some difficulty to follow the guidelines, especially those involving control of nocturnal feeding and sugar intake. Thus, a more specific approach is required for individual assessment of each child. In addition to this, personalized alternatives could be indicated to control these factors, such as: a) feeding throughout the first year of life, but before eruption of the first teeth; b) establishing a maximum limit of 12 to 14 months for breast and bottle feeding26. These measures established in the first year of life could control the free demand for sugar intake from juices, soft drinks and other cariogenic liquids via bottles or cups. Parents abandon oral health promotion programs for several reasons, e.g., choose to take their children to be treated by the family dentist, change their address, mothers may begin or go back to work when their children are old enough, lack encouragement or the may be even financial reason17. In this study, the most frequent reason for abandoning the program was changing for similar health service (40.0%), which demonstrates the program's ability in become parents conscious of their role in promoting their children oral health. The change from one clinic to another rather than giving up of oral health promotion means that the program has being reaching some of its goals. Although the program offers daily services from Mondays through Fridays, morning and afternoon, difficulties were reported to appointment times, resulting in the child's loosing the place in the program due to consecutive absences. The continuity of dental care by those who dropped out of the program can be considered an indicative of the education importance to a parents/caregivers preventive conscious. Despite of the parents' compliance difficulties, the educative-preventive measures lead to good oral health when adopted since the first year of life, independently of the caries risk in this age. The findings of this survey showed that caries risk in the first year of life was not efficient to predict dental caries experience at 5 years of age. The caries risks must be systematically checked between 1 and 5 years when hygiene and diet undergo drastic changes. The importance of oral health promotion should also be highlighted since the first year of the children's life. Although dental health promotion through educational and preventive practices since the child first year of life leads to a good oral health, educational practices should be improved to increase the compliance of the parents to the guidelines of the oral health program. The change from one clinic to another rather than giving up of oral health promotion program means that the program has reached some of its goals, showing that the parents become conscious of the importance of dental health promotion for their children. References
The following images related to this document are available:Photo images[os10033t2.jpg] [os10033t1.jpg] [os10033f1.jpg] [os10033f2.jpg] [os10033t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}