 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Braz J Oral Sci, Vol. 9, No. 3, July-September, 2010, pp. 371-375 Effect of post length on endodontically treated teeth: fracture resistance Jefferson Ricardo Pereira1, Accácio Lins do Valle2, Talita Magro Juvêncio3, Thais Maria Freire Fernandes3, Janaina Salomon Ghizoni4, Marcus Vinícius de Reis Só5 1DDS, MSc, PhD, Department of Prosthodontics, Dental
School, University of South of Santa Catarina, Brazil Correspondence to: Jefferson Ricardo Pereira Rua Rio Grande do Sul, 1901 - apto 303 Mar Grosso Laguna SC CEP: 88790-000 Brazil Phone: +55 (48) 36471571 Fax: +55 (14) 36264088 E-mail: jeffripe@rocketmail.com Received for publication: April 09, 2010 Abstract Code Number: os10038 Aim: This study compared the fracture resistance of
endodontically treated teeth restored with posts and cores systems with different
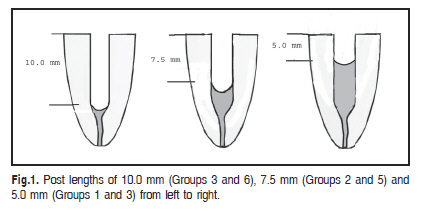
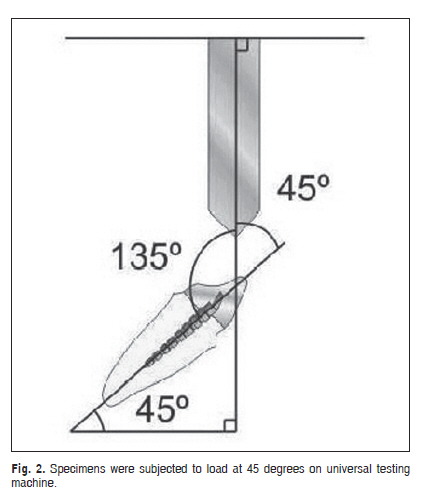
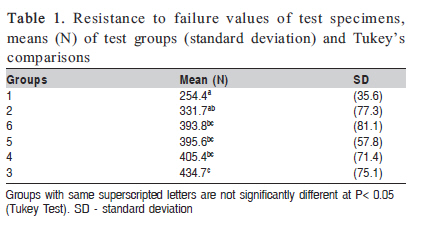
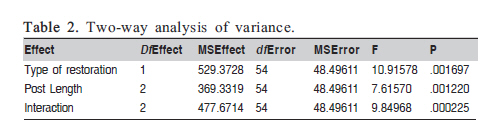
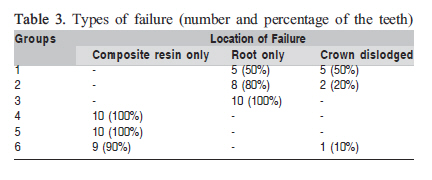
post lengths. Keywords: post and core technique, composite resin, fracture strength. Introduction Numerous techniques to restore endodontically treated teeth have been advocated with criteria for success depending on variations in length1, shape and surface configuration2, amount of dentin structure3-5, materials and techniques used in construction6. In prosthodontic practice, the task of restoring endodontically treated teeth is encountered almost daily. The pulpless tooth is known to present a higher risk of biomechanical failure than vital teeth7. The generally accepted explanation for the increased failure rate is the substantially loss of tooth structure during endodontic access, dowel space preparation, and cavity preparation8. The posts are necessary to allow the clinician to rebuild enough tooth structure to retain restorations9. The price for added retention, however, may be an increased risk to damage tooth structure. The custom cast post and core system has been regarded as the restoration of choice for endodontically treated teeth when there is no coronal dentin. However, the use of prefabricated post systems are increasing because all steps can be completed chairside, and fair clinical success can be expected, simplifying the restorative procedures3. Some authors3,10 advocated that roots restored with cast posts exhibited significantly higher internal stresses than prefabricated posts. The length of a post relative to root length is an unresolved problem in post design11. With recent improvements in the bonding of composite resin to dentin, true internal retention may assist with treatment success12-14. Laboratory studies have shown that increasing the length of the post in teeth with post and core results in a more favorable stress distribution along the post 2,15-16 and an increased post length improves the resistance of the restored tooth to fracture17. A previous clinical study showed an increased survival rate has been correlated with increase of post length7. On the other hand, another study showed a minimal difference in stress distribution between varying post lengths18, while other authors observed that an increase in post length as such will not necessarily increase the fracture resistance of the tooth19. It is important to notice that it may not always be possible to use a long post, especially when the remaining root is short or curved. Several studies have suggested that it is important to preserve 3 to 5 mm of apical gutta-percha to maintain the apical seal20. The purpose of this study was to evaluate the relative effect of post length (length of the vertical dentinal overlap of the crown) and type of post and core (custom cast post and core or prefabricated post and composite resin core) on the resistance of endodontically treated teeth. The research hypotheses were that there is a significant difference in the effect of post length on the fracture resistance, and that there is a significant difference between the types of posts. Material and methods Sixty human maxillary canines freshly extracted for periodontal reasons were selected and stored in distilled water at 37ºC during the course of the study. Teeth with cracks, caries, restoration, and/or roots shorter than 15 mm (measured with a millimeter ruler from the apex until the cementoenamel junction - CEJ) were discarded. The roots were scaled with periodontal curettes and water and were sectioned with double-faced diamonds discs (KG Sorensen, Barueri, SP, Brazil) to a standardized length of 15 mm. The endodontic treatment was done using a standard master apical file #20 (Dentsply Maillefer, Ballaigues, Switzerland) that extended 1 mm beyond the apex and the preparation took place with a conventional step-back technique to an International Standardization Organization (ISO) file #35 (Dentsply Maillefer) at the apical constriction. The teeth were obturated by lateral condensation using gutta-percha points (Tamari, Tamariman Industrial LTDA, Macaçaruru, AM, Brazil) and an ISO 35 primary gutta-percha master cone (Tamari, Tamariman Industrial LTDA). Root canal sealer (Endomethasone Ivory; Septodont Brasil, Barueri, SP, Brazil) was used as the sealer. After this, the teeth were randomly divided into 6 groups of 10 teeth each. The randomization was accomplished by drawling lots. Different post preparations were standardized using a #5 reamer (Largo; Dentsply Maillefer). Five millimeters of gutta-percha (apical to CEJ) from each filled canal in groups 1 and 4, 7.5 mm in groups 2 and 5, and 10 mm in groups 3 and 6, as showed in Figure 1. In groups 1, 2 and 3 the tooth was restored with a custom cast post and core. Impression of the root canals was made with acrylic resin (Duralay, Reliance Dental Mfg. Co. Chicago, Ill). The cores were standardized using a core-forming matrix (TDV Dental, Pomerode-SC, Brazil). The patterns were invested (Cristobalite, Whip-Mix Corporation, Louisville, Ky,) and cast in Cu-Al alloy (NPG, AalbaDent, Cordelio, CA). After casting, small nodules were removed if present. The post-cores were sectioned and seated to their corresponding teeth and Rely X luting cement (3M Dental Products Division, St. Paul, MN, USA) was used to cement them. The material was prepared according to the manufacturer's instructions and taken to the canals with a spiral file (Lentulo, Dentsply Maillefer, Ballaigus, Switzerland) at low speed. Cement was placed on the post and seated under 9 kg of pressure during 10 min. After this time, the pressure was released and the post was held in place until final setting of the cement. Excess cement was removed and each specimen was returned to storage in distilled water. In groups 4, 5 and 6 the canals were restored with prefabricated stainless steel, parallel-sided, serrated posts with a tapered end (number 5317, Screw-Post, Euro-Post Anthogyr S.A., Sallanches, France). In these groups, the teeth were cemented with the same material and the same technique as used in the other groups. The coronal portion was made with composite resin material (Z250; 3M Dental Products Division).The root surfaces and cervical dentin was etched with 37% phosphoric acid for 30 s, rinsed, and air dried. Two coats of bonding agent (Prime & Bond 2., Dentsply Ind. e Com Ltda., Petropolis, RJ, Brazil) was applied to the cervical dentin and the coronal portion of the post and were light-cured for 20 s (Ultraled, Dabi Atlante, Ribeirão Preto, SP, Brazil; 110 W). Cores were fabricated in a standardized form, using the same core-forming matrix as used in the other groups. Five increments of the composite resin were applied to complete the coronal core, each requiring 40 s of light curing (Ultraled, Dabi Atlante, Ribeirão Preto-SP, Brazil) to complete the coronal core. The tip of the light guide of the curing unit was positioned 2 cm from the specimens on top of the core. All teeth were prepared with a #3216 diamond bur (KG Sorensen, Barueri, SP, Brazil) coupled to a high-speed handpiece (Super Torque 625 Autofix, Kavo do Brasil Ind. Com. Ltda., Joinville, SC, Brazil) with water spray coolant to simulate a crown preparation with 1.5 mm of facial reduction with a chamfer finish line and 0.5 mm of chamfered lingual reduction, and receive a PFM crown. All the finish lines, for all specimens and groups, were placed at the CEJ level. Crown wax (Kerr Corporation, CA, USA) patterns were then made for the specimens using vinyl polysiloxane (Aquasil, Dentsply, Konstanz, Germany) impressions obtained from the teeth prior to preparation. A lingual ledge was added to create a standard loading point. The wax patterns were sprued, invested (Cristobalite, Whip-Mix Corporation, Louisville-Ky, USA) and cast in a Ni-Cr alloy (Durabond, São Paulo, Brazil). Crowns were cemented using the same material used with the posts. Root surfaces were covered with a 0.6-mm-thick foil (Adapta foil; Bego, Bremen, Germany) to a depth 2 mm below the CEJ to produce a layer approximately equal to the average thickness of the periodontal ligament. Teeth were embedded in acrylic resin (Clássico, Artigos Odontológicos S/A, São Paulo, SP, Brazil) poured into molds made of same material (30 mm in height, and diameter of 22 mm and a internal space, located in the center of the mold, with diameter of 10 mm and 20 mm in height) along their long axes using a surveyor (Bio Art Equipamentos Odontológicos Ltda, São Carlos, SP, Brazil). Each tooth was removed from the resin block, by moving rods in an upward direction, when the first signs of polymerization were observed. The Adapta spacers were removed from the root surfaces. Aquasil was injected into the acrylic resin blocks, and the teeth were reinserted into them. A standardized silicone layer that simulated periodontal ligament thus was created3. The specimens were tested in a universal testing machine (Kratus K2000 MP, Dinamometros KRATOS Ltda, São Paulo, SP, Brazil (Figure 2). Each specimen was affixed in a custom-made apparatus (fabricated by the authors) that allowed it to be positioned at 45 degrees to the buccal/lingual long axis (Figure 2). The testing machine was set at a crosshead speed of 0.5 mm/min. The load was measured in Newtons (N). Failure threshold was defined as the point at which a specimen could no longer withstand increasing load and fracture of the post-core complex or root occurred. The mode of failure was recorder after the test using x4 binocular magnifier (Bio Art Equipamentos Odontológicos Ltda, São Carlos, SP, Brazil). Data were analyzed statistically by 2-way ANOVA to determine the overall differences among the means of the test groups and the overall variability within the test groups. Tukey's multiple-comparison test was conducted to determine which test groups were statistically different from the others. All testing was done with alpha equal to 0.05. Results Table 1 presents the mean fracture resistance values (in N) standard deviations obtained for each studied group. Significant differences were detected by ANOVA (Table 2) (p<0.001). The Tukey's test confirmed that the mean fracture resistance for group 3 was significantly greater than groups 1 and 2 and fracture resistance for the group 6 was not significantly greater than groups 5 and 6 (Table 1). The fracture patterns of all groups are presented in Table 3. The majority of the failures in the groups restored with custom cast and post occurred due to root fracture. However in the groups restored with prefabricated posts the failure occurred due to core fracture. Discussion The present study accepted the hypotheses that there is a significant difference in the effect of post length on the fracture resistance and the hypotheses that there is a significant difference between the types of posts. Group 3 presented higher fracture resistance (p<0.05) than groups 1 and 2. These findings are believed to be related to the higher strength of the nickel-chromium alloy, and the higher modulus of elasticity of this material10. This is in agreement with Standlee et al.2 and Holmes et al.16, who showed that increasing the post length in the tooth results in a more favorable stress distribution along the post. On the other hand, the results of the present study showed that the increase of post length in teeth restored with prefabricated posts and composite resin core did not increase significantly the fracture resistance of endodontically treated teeth. Studies have shown that post preparation weakens the root considerably15. Furthermore cementation of a post can regain some of the root's original strength15. In other words, the use of a post may weaken the root more than it reinforces it. This may explain why increasing post length in these groups did not consistently increase the fracture resistance of these roots in the present study. Our results are in agreement with those of Isidor et al.19, who showed that increasing post length in teeth restored with prefabricated posts did not increase the fracture resistance of endodontically treated teeth. We found no significant difference on fracture resistance was found when the group restored with custom cast post and core was compared to the group restored with prefabricated post and composite resin core with 5 mm of post length each one. This could be explained because the size and shape of the composite resin matrix particles account for 66% of its volume13, and this higher amount of inorganic particles corresponds to the maximum resistance of compressive load, surface hardness and wear resistance13. Furthermore, it has been demonstrated by some authors that roots restored with custom cast post and core presented significantly higher internal stress than prefabricated posts10. Core construction using prefabricated posts and composite resin is a viable technique for endodontically treated teeth3-6. Composite resin core fracture occurring when occlusal force is applied may be a positive occurrence because it could be protective of the supporting root12. The most common cause of failure when the choice is the direct technique (prefabricated post and composite resin) is fracture of the restorative material12. The results of this study are in agreement with another study that concluded that composite resin fracture can occur at a lower force than that required to yield root fracture14. When the cast post-and-core was used the most common failure is the fracture of the root12 as was observed in this study (Table 3). This investigation demonstrated that roots restored by individual cast posts with 10 mm of post length exhibited higher fracture resistance than those restored by prefabricated post and composite resin core. Despite its lower resistance, the technique using prefabricated posts and composite resin may be appropriate because there were no root fractures. Hence, the direct method appeared to protect the tooth structure12. The limitations of this study include that this was an "in vitro" experiment, which did not replicate oral conditions, and a single load to fracture test was used to test the fracture resistance of endodontically treated teeth. For more meaningful results, future studies should incorporate thermal cycling of the specimens and fatigue loading. Acknowledgements This study was supported by FAPESP. References
Copyright 2010 - Braz J Oral Sci The following images related to this document are available:Photo images[os10038f1.jpg] [os10038t2.jpg] [os10038t1.jpg] [os10038f2.jpg] [os10038t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}