 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Braz J Oral Sci, Vol. 9, No. 3, July-September, 2010, pp. 388-392 Self-perception of generalized aggressive periodontitis symptoms and its influence on the compliance with the oral hygiene instructions - a pilot study Renato Corrêa Viana Casarin1, Erica Del Peloso Ribeiro2, Francisco Humberto Nociti-Jr3, Enilson Antônio Sallum3, Antonio Wilson Sallum3, Márcio Zaffalon Casati3 1DDS, MS, PhD, Assistant Professor, University São
Francisco, Brazil
Correspondence to: Márcio Zaffalon Casati Departamento de Prótese e Periodontia FOP/UNICAMP Av. Limeira 901 - 13414-018 Piracicaba - SP Phone/Fax: 55 19 34125301 E-mail: casati@fop.unicamp.br Received for publication: December 07, 2009 Code Number: os10042 Abstract Aim: Patient's adherence to the periodontal treatment is fundamental
to the success of the therapy. Lack of response to the clinician's instructions
is influenced by various factors, including gender, age and psychosocial profile.
The aim of the present study was to evaluate the relationship between self-perceived
symptoms of generalized aggressive periodontitis and compliance with the oral
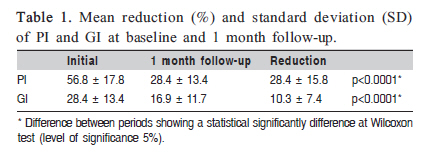
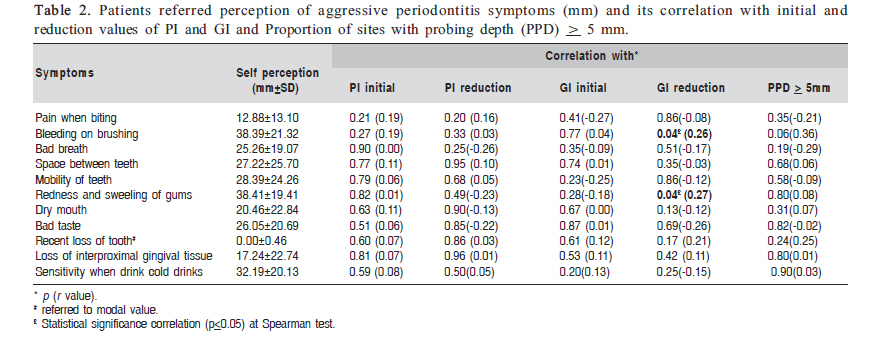
hygiene instructions. Keywords: compliance, generalized aggressive periodontitis, periodontal disease symptoms, self perception, oral hygiene instructions. Introduction A major aspect of the effective treatment of periodontal disease is adequate oral hygiene1, which consists of a combination of daily tooth brushing, inter-dental cleaning, and when necessary, use of chemotherapeutic agents (e.g. mouthwash)2. Therefore, the success of the treatment ultimately relies on patients' compliance with daily dental care, in which satisfactory plaque and inflammation control is fundamental. Unfortunately, evidence shows that only a portion of the patients actually comply with the treatment and the level of adherence decreases as the time of treatment is extended over the years3-6. Ciancio2 suggested that this lack of compliance would lead to serious consequences for chronic periodontitis, and there is an urgent need to develop and validate effective strategies to improve the performance of patients with periodontitis in applying daily prophylactic dental care and identifying the reasons for their non-compliance. Patient adherence depends on believing in the necessity of following preventive and/or treatment recommendations7 and this has been addressed in numerous studies that have investigated patients' behavioral practices with regard to adherence to the treatment of periodontal disease, especially oral hygiene. Some reasons given for non response with respect to oral hygiene include unwillingness to perform oral self-care8, lack of motivation9 and poor dental health beliefs10. An important consideration is that adherence also depends on social and psychological factors11. Background factors that influence periodontal disease and beliefs regarding oral health could have a negative influence on the adhesion to Supportive Periodontal Treatment12. Age and gender can also negatively modify adherence to the treatment13-14. Some theories of human cognitive behavior have also been used to explain non-compliance. The four main theories include the health belief model (HBM); transtheoretical model (TM); theory of reasoned action/theory of planned behavior (TRA); and the social-cognitive theory (SC)15. The HBM focuses on an individual's perception of the threat posed by a health problem. The TM is concerned with an individual's readiness to change. The TRA focuses on an individual's intention to perform a behavior. The SC incorporates intra-personal and inter-personal factors and suggests that the benefits of behavior must outweigh the costs. In this context, self perception of the symptoms could have an influence on adherence to periodontal treatment, since the determining factor is that the patient must seek treatment, and this could represent the real importance the patient attaches to oral conditions. This idea increases in importance when considering severe periodontal disease, such as aggressive periodontitis, recognized as a rare condition affecting young subjects, and presents rapid periodontal destruction, also induced and aggravated by biofilm accumulation. Thus, the recognized approaches known to contribute to patient adhesion to oral hygiene could be useful tools in therapy to control the disease. The aim of the present study was to evaluate the relationship between self-perception of generalized aggressive periodontitis symptoms and adherence to the oral hygiene instructions. Material and methods Subjects The patients enrolled in the present study were selected from those initially referred to the Periodontal Clinic of the Piracicaba Dental School, State University of Campinas, Brazil for oral examination and periodontal treatment. Patients who presented generalized aggressive periodontitis were selected in accordance with the following inclusion criteria: 1) under 35 years of age; 2) clinical and radiograph attachment loss on incisors and first molars, and in three other teeth; 3) at least 8 sites with pocket probing depth (PPD) ≥ 5 mm, of which 3 of them with PPD ≥ 6 mm; and 4) at least 20 teeth in the mouth. The exclusion criteria were: 1) smoking and pregnancy/nursing mothers; 2) use of mouthrinse or antibiotics 6 months before the study; 3) history of relevant medical condition; and 4) periodontal treatment, including professional prophylaxis, 6 months before the study. Ethics The study protocol was previously approved by the Institutional Clinical Research Ethics Committee of the State University of Campinas (UNICAMP) Protocol No. 24/2006. All the selected patients received and signed an informed consent form and thereby agreed to participate in the study. Questionnaire Initially, the patients received a questionnaire to assess their periodontal status. The patients were questioned about their perception of: pain in the gums, bleeding while brushing, bad breath, spaces between the teeth, mobility of teeth, redness and swelling of gums, dry mouth, bad taste, recent loss of teeth, loss of interproximal gingival tissue and sensitivity when drinking cold or hot drinks. Each affirmative was followed by a VAS (Visual Analogue Scale) ranging from NO FEELING to STRONG FEELING. To indicate a recent tooth loss, the patient checked YES or NO. The self- evaluation of recent loss was considered without determining the length of time since the loss. Each subject was instructed to check on the chart their self-assessment of each symptom listed above. After this, the distance from the origin on the scale to the mark made by the patient, was measured with a caliper. Clinical parameters and compliance assessment The measurements were made by a single calibrated examiner (kappa index = 0.91) using a periodontal probe (PCPUNC 15-Hu-Friedy/Chicago, IL, USA), at the beginning of the study. A dichotomous analysis of the presence of plaque (Plaque Index PI16) was made on six surfaces of each tooth, excluding the third molars. The presence of dental plaque accumulation on the buccal, lingual and proximal surfaces of all teeth was assessed using a periodontal probe. To determine the gingivitis status of each patient, a dichotomous index was also used (Gingival Index GI16). Bleeding of the gingival margin within 10 s after probe stimulation was considered positive. PI and GI were evaluated at the beginning and thirty days after the patient received prophylaxis and oral hygiene instructions. Reduction in PI and GI was considered to assess each patient's level of compliance with the oral hygiene instructions. Correlation between self-perception and severity of the disease was also studied. Initially, the total number of sites with probing depth ≥ 5 mm presenting bleeding on probing was determined in a baseline examination using a periodontal probe. After that, a percentage of these sites per patient was calculated (PPD). Prophylaxis and Oral Hygiene Instructions Immediately after the first evaluation, professional prophylaxis was performed in each patient, consisting of calculus and plaque removal with an ultrasonic device (Profi III Bios, Dabi-Atlante, Ribeirão Preto, SP, Brazil) and brushes. After this, patients were given instructions on toothbrushing and interproximal cleaning with dental floss. All the patients received the same protocol of prophylaxis and instructions. The importance of plaque control and instructions on oral care were reinforced within 15 days after the first session17-18. Data Analysis The Biostat® program (Version 3.0) was used to determine the relationship between the parameters. Spearman's correlation test was used to test the relationship between the values of self-perception and initial PI and GI values, as well the PPD values. To determine the influence of self-perception of symptoms on adherence to the oral hygiene instructions, the percent reduction in PI and GI was also correlated with these values. Wilcoxon's test was used to evaluate the difference in PI and GI before and after initial treatment. The level of significance was set at 5%. Results Twenty-six patients were enrolled in this study. The mean age was 27.1±4.9 years. Gender distribution revealed a predominance of females (73.1%). The PI and GI values and the results of treatment are shown in Table 1. The initial PI was 56.8% and 30 days after the prophylaxis and oral hygiene instructions this value declined to 28.4% (p<0.0001). There was also a statistically significant reduction in GI after the treatment (28.4% to 16.9%) (p<0.0001). The self-perception values attributed by each patient are shown in Table 2. None of the perception values showed a correlation with the initial PI and GI values (Table 2), and no correlation was observed between the self-perceived symptoms and the reduction in PI. There was however, a positive correlation between the perception of some of the symptoms and reduction in GI. The greater the perception of bleeding on tooth brushing (p=0.04, r=0.27) and redness and swelling of gums (p=0.04, r=0.26), the greater the reduction in bleeding (statistical significance shown by Spearman's correlation) (Table 2). The mean percentage of sites with probing depth ≥ 5mm with bleeding on probing was 63±20%. The Spearman's correlation test also showed no correlation between this percentage and the self-perceived symptom scores (Table 2). Discussion The efficient inflammation control obtained by means of supragingival plaque control is fundamental to periodontal treatment success, and many psychosocial and psychological characteristics influence the patient's adherence to the oral hygiene instructions19. The proper perception of oral health could influence adherence by showing the real importance the patient attaches to the treatment20, determining a high or low acceptance of the oral hygiene instructions. This is especially important in young patients, who normally present a low adherence to treatment5. Thus, the present study was designed to evaluate the relationship between the self-perception of generalized aggressive periodontitis symptoms and patient compliance with instructions. The results showed that the patients with a greater perception of some of the aggressive periodontitis symptoms adhered to the treatment more firmly, with greater reductions in the GI within 1 month. A positive correlation was found between the perception of bleeding on tooth brushing and redness and swelling of the gums and reductions in the GI. Moreover, these symptoms, which recent studies have shown to be normally associated with periodontal disease, were those most perceived by the patients18. This correlation could be involved in a personal definition of disease by patients. Patient's definition of disease differs from that of the professionals' definition20-21. Professionals usually consider the presence or absence of illness whereas patients consider the social and functional problems caused by the disease, such as the capacity to smile, speak and chew22. Hence, the social influence of the disease appears to interfere more significantly in the perception than the presence of the actual disease, and to the patients, bleeding and swelling of gums could represent a social impact. This difference regarding the influence based on the definition of the disease was ratified by another result found in the present study. None of the self-perceived symptoms of the disease showed a correlation with the percentage of sites presenting bleeding, and with PPD ≥5mm. Patients appear to perceive the disease differently from the professional; this perception involving the psychosocial influence of disease to a greater extent than does its presence or severity. Certain psychological models can be applied to explain levels of compliance with dental and medical treatment. The HBM proposes the following requirements for behavior change: (1) a perception of susceptibility to disease; (2) a belief that the impact of this disease will affect him/her biologically and/or psychosocially; (3) a belief that the potential benefits of the treatment outweigh the risks of the disease and its treatment; (4) an ability to surmount barriers to treatment23. The TM suggests that six stages of changes are involved in health behavior: pre-contemplation, contemplation, preparation, action, maintenance and termination24. In both models, the perception of the disease is an important variable that could determine the level of compliance with the treatment. Thus, the analysis of self perception, as shown in the present study, could represent a key to achieving and improving patient compliance. Moreover, the influence of the perception of symptoms could also be related to the Leventhal's theory. Leventhal et al.25 postulated that people's behavior in response to a disease is determined by their representation of that disease. Disease representation has a cognitive and an emotional aspect and they are constructed through direct or vicarious experiences as well as information received from the social environment and health professionals. They propose that patients will only adhere to a treatment if they believe that this treatment will have a positive effect on their health and that they have the capacity to effectively act as required. The application of this model in periodontal treatment was tested by Phillipot et al18. Their results showed that the application of Leventhal's method produced a higher rate of compliance with oral hygiene instructions, producing a lower level of plaque accumulation within a month, than in patients who received traditional oral hygiene instructions. In this context, the self-perception of symptoms, and particularly the recognition of the changes after adherence to the oral hygiene instructions, could help patients believing their own capacity of acting on the instructions and adhere to the treatment. This could be seen in the results of present study, in which those patients who perceived their own symptoms of the disease showed better adherence to oral hygiene. The GI has been used as an indicator of compliance in previous studies12,17-18,26. This index is an important tool to evaluate significant adherence to the daily oral hygiene regime, since the reduction in bleeding represents efficient and continued plaque control. Moreover, the use of the PI may represent efficient hygiene but it does not affirm that control is continuous or was only implemented near the revaluation day. Therefore, the reduction in the GI observed in the present study represents an adherence to the oral hygiene instructions. The reduction in bleeding observed in the present study could be explained by improvement in the daily oral conditions after patients received prophylaxis and oral hygiene instruction (reinforced during the study) and represents a reduction in gingival inflammation, as seen in previous studies17-18. The role of the reduction of these aspects (bleeding and PI) during periodontal therapy, especially during the initial phase of the treatment, is well demonstrated in the literature. The supragingival plaque control due to the compliance with the oral hygiene instructions, sessions of prophylaxis and calculus/plaque retenders removal shown in recent studies be capable of produce favorable clinical and microbiological changes in periodontal disease27,28. However, in this pilot study, posttreatment follow up was done for only 1 month. Long-term implication of initial adherence to the treatment is unknown, and has yet to be determined in future studies. Therefore, a larger population of patients with aggressive periodontitis, specifically generalized periodontitis, should be evaluated to ratify the results of this study. In spite of study limits, the obtained results can be easily transported to daily practice, in which recognition by patients with greater levels of perception could be an indication of enhanced adherence to the initial treatment. Nevertheless, the key idea of this study was to recognize patients with a lower perception, which provided an opportunity to plan a patient-specific approach to improve their knowledge and self-perception of symptoms and ultimately their compliance with the treatment. In conclusion, within the limitations of this study, patient adherence to oral hygiene instructions could be related to the self-perception of generalized aggressive periodontitis symptoms. References
Copyright 2010 - Braz J Oral Sci The following images related to this document are available:Photo images[os10042t2.jpg] [os10042t1.jpg] |
| |||||||||

{kind=link}
{kind=link}