 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Braz J Oral Sci, Vol. 9, No. 3, July-September, 2010, pp. 402-409 Antimicrobial activity of chlorhexidine in root canals instrumented with the ProTaper Universal™ System Andréa Cruz Câmara1, Miracy Muniz de Albuquerque2, Carlos Menezes Aguiar3, Ana Cristina Regis de Barros Correia4 1PhD Student in Pharmaceutical Sciences, Department
of Pharmaceutical Sciences, School of Pharmaceutical Sciences, Federal University
of Pernambuco, Brazil
Correspondence to: Andréa Cruz Câmara Rua Nadir de Medeiros, 51, Piedade, Jaboatão dos Guararapes PE 54410-110 Brasil. Phone: (+55) 81 3361 5269.E-mail: andreaccam@yahoo.com.br Received for publication: May 26, 2010 Code Number: os10045 Abstract Aim: The purpose of the present study was to evaluate the
antimicrobial activity of 0.2%, 1%, and 2% chlorhexidine in root canals instrumented
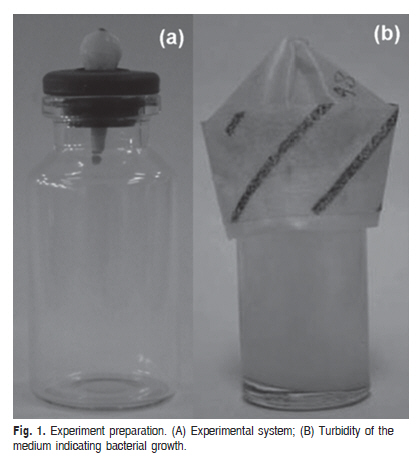
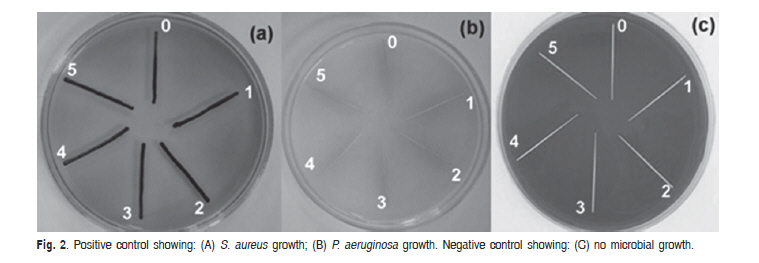
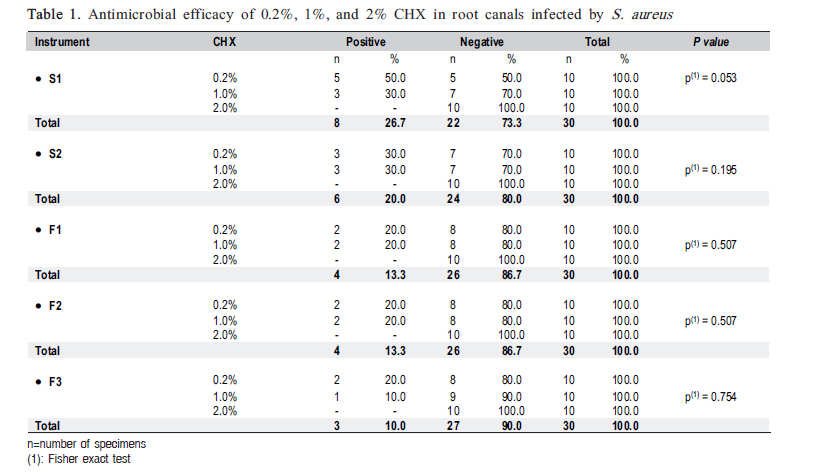
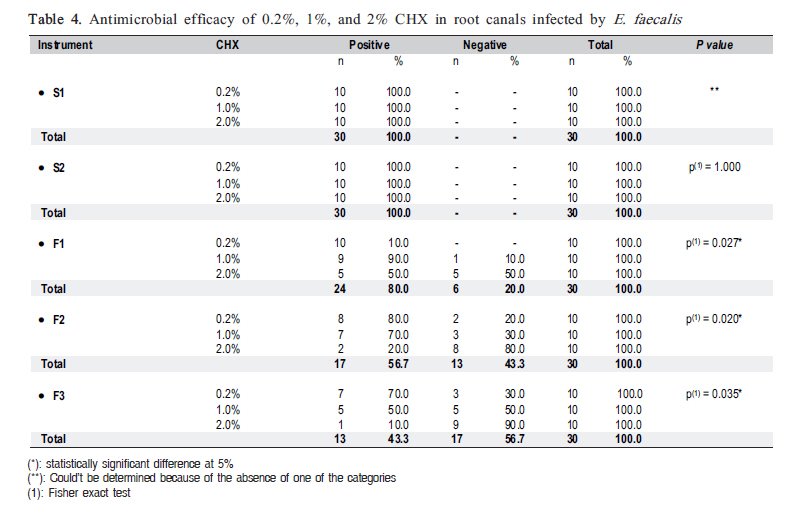
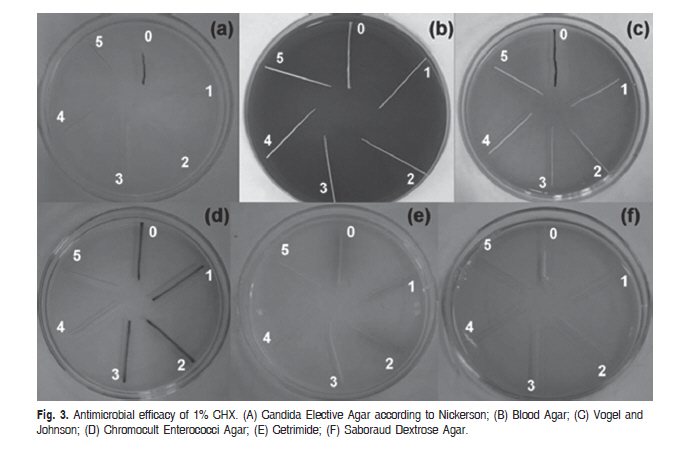
with the ProTaper Universal™ system. Keywords: antimicrobial activity, chlorhexidine, ProTaper Universal™, root canal irrigant, rotary instrumentation. Introduction The contribution of microorganisms to the development of pulpal and periapical disease has been well documented. Enterococcus faecalis, Candida albicans, Pseudomonas aeruginosa, and Staphylococcus aureus are considered by many to be the most resistant species in infected root canals and they are often associated with endodontic treatment failures1-3. Root canal system disinfection may be accomplished by using irrigating solutions during mechanical instrumentation. Antibacterial irrigating solutions may reach canal ramifications and inaccessible areas and permeate completely through the dentinal tubules. Therefore, several irrigating solutions in different concentrations with antibacterial activity have been recommended for use to irrigate and disinfect root canals in combination with root canal preparation3. A large number of substances have been used as root canal irrigants. Although several irrigants have been proposed over the years, sodium hypochlorite (NaOCl) remains the most widely used1. It is an effective antimicrobial agent and an excellent organic solvent for vital, necrotic and fixed tissues. However, it is highly irritating to periapical tissues, especially at high concentrations4. The biocompatibility problems associated with the use of concentrated NaOCl have led to the use of substances with known antimicrobial properties and less toxicity, such as chlorhexidine (CHX). This substance has been used in Endodontics as an irrigating solution and intracanal medicament on account of its broad antimicrobial-spectrum2, substantive properties5, relatively low cytotoxicity6, and ability to inhibit adherence of certain bacteria7. However, it does not dissolve organic tissue. In the last decade, several rotary nickel-titanium (NiTi) instruments with different configurations and designs have been developed with the aim to reduce the preparation time and to simplify the preparation procedure8. The ProTaper Universal™ rotary system is one of the most popular endodontic NiTi systems currently on the market9-11. As the advent of rotary techniques for root canal preparation shortened the working time in comparison to manual instrumentation, the irrigant should be one that exerts its antimicrobial activity quickly against the microorganisms found in the root canal and dentinal tubules. Therefore, the purpose of this in vitro study was to evaluate the antimicrobial activity of 0.2%, 1%, and 2% CHX against some endodontic pathogens in root canals instrumented with the ProTaper Universal™ system. Material and methods Sample selection and preparation Fifty freshly intact human mandibular premolar teeth (length 20-21 mm), straight, with radiographically confirmed single root canal and fully formed apices, were obtained from the Human Tooth Bank of the Prosthodontics and Oral and Maxillofacial Surgery, Dental School, Federal University of Pernambuco, Brazil, for this study after approval by the Research Ethics Committee of the University's Center of Health Sciences. The teeth were stored in 10% formalin until use. The coronal access was performed. To determine the working length (WL), a #10 K-file (Dentsply-Maillefer, Ballaigues, Switzerland) was inserted into the root canal until it was visible at the apical foramen. The WL was calculated to be 1 mm less than the length obtained with this initial file. The specimens were stored in glass test tubes and were individually sterilized in an autoclave at 121 °C for 30 min. Ten samples were randomly chosen and immersed totally in bottles containing 10mL of autoclaved Brain Heart Infusion (BHI, Acumedia, Lansing, Michigan, USA). They were kept in an incubator at 37°C for 96 h to check the sterilization's efficacy. Experiment preparation The methodology used was described previously by Câmara et al.12. Glass vials with rubber stoppers were adjusted for use in this experiment (Figure 1, A). The experimental systems were sterilized in an autoclave at 121°C for 30 min, and inside a laminar flux chamber (Veco, Piracicaba, Brazil), they were filled with BHI (Acumedia). The experimental systems were kept in an incubator at 37ºC for 96 h and no turbidity of the medium was observed. Bacterial strains The microorganisms strains used in this experiment were obtained from the American Type Culture Collection™ (ATCC, Rockville, MD, USA): Candida albicans (ATCC 10231), Pseudomonas aeruginosa (ATCC 9027), Enterococcus faecalis (ATCC 19433) and Staphylococcus aureus (ATCC 6538). Bacterial cultures and root canal infection The following procedures were performed inside a laminar flux chamber (Veco, Piracicaba, Brazil) using sterilized instruments and materials. Isolated 24 h colonies of pure cultures of C. albicans, P. aeruginosa, E. faecalis and S. aureus grown on 10% sheep blood plus BHI (Newprov, Paraná, Brazil) agar plates were suspended in a sterile 0.85% NaCl solution. The suspensions of the microorganisms had the optical density adjusted spectrophotometrically to approximately 3.0 x 108 colony-forming units (CFU) mL-1 (equivalent to 1.0 McFarland scale). From each experimental suspension, 1 mL was removed and a mixture of the four selected microorganisms was prepared. The sterilized experimental systems were then opened. The root canals were infected, except for the negative control, with 10mL of the suspension containing the microorganisms using an automatic micropipette (Gilson, Villiera-le-Bel, France) placed into the access cavity of each tooth. After introduction of the suspension, sterile #10 K-files (Dentsply-Maillefer) were used to carry the bacterial suspension to the WL. The infected teeth were incubated at 37 ºC for 48 h. The turbidity of the medium during the incubation period indicated bacterial growth (Figure 1, B). The purity and the identification of the cultures were confirmed by Gram staining, the colony morphology and the growth on Petri dishes with the media: Cetrimide Agar (Acumedia) to verify the presence of P. aeruginosa, Vogel and Johnson Agar (Acumedia) to verify the presence of S. aureus, Saboraud Dextrose Agar (Acumedia) and Candida Elective Agar according to Nickerson (Merck, Darmstadt, Germany) to verify the presence of C. albicans, Blood Agar (Newprov, Pinhais, PR, Brazil) to verify the hemolytic activity, and Chromocult Enterococci Agar (Merck) to verify the presence of E. faecalis. If the 4 microorganisms were not identified, the experimental system would be discarded. The efficiency of the method for the infection of the root canal was observed in a pilot study. All assays were conducted in triplicate under aseptic conditions. Root canal biomechanical preparation Freshly prepared 0.2%, 1%, and 2% CHX solutions (Farmácia Escola Carlos Dumont de Andrade, Recife, PE, Brazil) were used for root canal irrigation. The infected teeth were removed from the experimental systems with the contamined medium and transferred to glass vials without the medium, in order for the teeth to remain fixed at the beginning of the instrumentation. The specimens were randomly divided into 3 experimental groups and 2 control groups with 10 root canals each according to the irrigant used during root canal preparation as follows: Group 1: 0.2% CHX; Group 2: 1% CHX; Group 3: 2% CHX; Group 4 (positive control): 0.85% sterile saline; Group 5 (negative control- without microorganisms): 0.85% sterile saline. For irrigation of the root canal, the 3-mL FCF syringe system (FCF, São Paulo, SP, Brazil) with a 30-gauge needle (Injecta, Diadema, SP, Brazil) was used. Irrigation was performed at the beginning of instrumentation, between changes of instruments, and at the end of biomechanical preparation. All root canals were instrumented with the ProTaper Universal™ using an electric motor (Driller Endo-Pro Torque, Sao Paulo, Brazil) at a speed of 300 rpm as follows: (1) SX file was used to one half of the WL; (2) S1 file was used up to 4 mm short of the apex; (3) S1 and S2 files were used to the full WL; and (4) F1, F2 and F3 files were used to the full WL. A single operator instrumented all root canals. After the instrumentation with each instrument and before drying the root canal, in groups 1, 2, and 3, irrigation with 0.5% Tween 80 + 0.07% lecithin was used to neutralize CHX. The shaping time was recorded, excluding the assessment of the antimicrobial action of the irrigants. Assessment of antimicrobial action the irrigants: To assess the antimicrobial action of the irrigants, sterile paper points were consecutively placed in the root canal. Each paper point was left in the root canal for 1 min, as follows: 0-initial (before biomechanical preparation), 1-after instrumentation with S1 file to the full WL, 2-after instrumentation with S2 file, 3-after instrumentation with F1 file, 4-after instrumentation with F2 file, and 5-after instrumentation with F3 file. The paper points were transferred to Petri dishes containing the media: Cetrimide Agar, Vogel and Johnson Agar, Saboraud Dextrose Agar, Candida Elective Agar according to Nickerson, Chromocult Enterococci Agar, and Blood Agar. The plates were then incubated at 37ºC for 48 h. After incubation, bacterial growth was assessed with light microscopy at 400×. All assays were conducted in triplicate under aseptic conditions to ensure the reliability of this study. Statistical analysis The categorical data were summarized by means of absolute frequency and relative percentage and the numeric data by means of the usual descriptive statistics of location and dispersion. The results were statistically analyzed using the Chi-squared test and the Fisher exact test were used when the conditions for the use of the Chi-squared test were not verified (statistical inference). A level of significance of 0.05 was adopted. The SPSS software (Statistical Package for the Social Sciences, version 13, Chicago, USA) was used. Results Irrigant antimicrobial efficacy Microbial growth was found in all initial samples (0-before biomechanical preparation), except for the negative control group, demonstrating that the contamination was effective in all root canals of all groups. All positive controls showed microbial growth before the biomechanical preparation and after the instrumentation with S1 (1), S2 (2), F1 (3), F2 (4), and F3 (5) files (Figures 2A and B), while negative controls showed no microbial growth (Figure 2C) before the biomechanical preparation and after the instrumentation with S1, S2, F1, F2, and F3 files. The irrigants' antimicrobial efficacy against S. aureus, P. aeruginosa, C. albicans and E. faecalis is shown in Tables 1, 2, 3, and 4, respectively. Table 1 presents the antimicrobial efficacy of 0.2%, 1%, and 2% CHX in root canals infected with S. aureus. In the 0.2% concentration, the frequency of positive samples was higher in S1 (with 5 specimens), equal to 3 in S2 and equal to 2 specimens in F1, F2 and F3. In the 1% concentration, the frequency of positive samples was higher in S1 and S2 (with 3 specimens), equal to 2 in F1 and F2 and equal to 1 specimen in F3. In the 2% concentration all the samples were negative for S. aureus. There was no statistically significant difference between the concentrations of CHX for any of the instruments used (p>0.05). Table 2 presents the antimicrobial efficacy of 0.2%, 1%, and 2% CHX in root canals infected with P. aeruginosa. In the 0.2% concentration, the frequency of positive samples was higher in S1, S2 and F1 (with 6 specimens), equal to 4 in F2 and equal to 1 specimen in F3. In the 1% concentration, the frequency of positive samples was equal to 6 in S1, equal to 3 in S2 and there was no bacterial growth in F1, F2 and F3. In the 2% concentration, all the samples were negative for P. aeruginosa. With the exception of the F3 instrument, there were statistically significant differences between the concentrations of CHX and the instruments used (p <0.05). The antimicrobial efficacy of 0.2%, 1%, and 2% CHX in root canals infected with C. albicans is shown in Table 3. In the 0.2% concentration, the frequencies of positive samples were 6, 5, 3, 2 and 1 respectively for S1, S2, F1, F2 and F3. In the 1% concentration, the frequency of positive samples was equal to 7 in S1, equal to 3 in S2, equal to 1 in F1 and there was no microbial growth in F2 and F3. In the 2% concentration, all samples were negative for C. albicans. Statistically significant difference was found only between the concentrations of CHX and the instruments used was observed in S1 (p <0.05). The antimicrobial efficacy of 0.2%, 1%, and 2% CHX in root canals infected with E. faecalis is shown in Table 4. All samples were positive in S1 and S2 in all test irrigants. In the 0.2% concentration, all the samples were positive in F1, equal to 8 in F2 and equal to 7 in F3. In the 1% concentration, the frequencies of positive samples were 9, 7 and 5 respectively for F1, F2 and F3. In the 2% concentration, the frequency of positive samples was equal to 5 in F1, equal to 2 in F2 and equal to 1 in F3. There were statistically significant differences between the concentrations of CHX and the instruments F1, F2 and F3 (p <0.05). Figure 3 shows the antimicrobial efficacy of 1% CHX against (A) C. albicans, (B) E. faecalis, (C) S. aureus, (D) E. faecalis, (E) P. aeruginosa, and (F) C. albicans, respectively. Root canal preparation time The mean preparation time for the ProTaper Universal™ system was 4.0 ± 1.0 min. Discussion The methodology used to assess the antimicrobial activity of endodontic irrigants in this study was the artificial infection of extracted teeth with the selected microorganism and in situ irrigation with the test antimicrobial agents, which according with some authors is an effective method to evaluate anti-fungal as well as antibacterial properties of any solution12-13. After 48 h of incubation, all initial samples were recovered with pure cultures of viable microorganisms confirming the efficiency of the infection methodology adopted for the present research. Microbial sampling is another important step that varies among the different methodologies. In this research, the microbial samples collected within the root canals with sterile paper points were obtained before, during and after the biomechanical preparation with the ProTaper Universal™ system in order to evaluate the antimicrobial activity of 0.2%, 1%, and 2% CHX. The role of bacteria and their by-products in the initiation and perpetuation of pulpal and periapical disease has been well established. The pathogens used in this study were selected because of their clinical importance and association with the endodontic infection. Microorganisms such E. faecalis, C. albicans, P. aeruginosa, and S. aureus have been associated in cases of persistent periradicular lesions1-3,14. Several irrigating solutions might be used during the treatment of infected root canals. These require, among other properties, antimicrobial activity15-17. CHX was developed in the late 1940s in the research laboratories of Imperial Chemical Industries Ltd. (Macclesfield, England). It is widely used as a root canal irrigant or intracanal medication5,18. This cationic bisbiguanide is highly efficacious against several gram-positive and gram-negative oral bacterial species as well as yeasts19. CHX was chosen as the irrigating solution to be used in this study because it has been recommended as an alternative or potentially preferred irrigant for endodontic treatment when there are reports of hypersensitivity to NaOCl by the patient, in cases of open apex where there is great risk of apical leakage of the chemical solution and in cases of microorganisms considered to be resistant to endodontic therapy20. When the antimicrobial activity of CHX was compared with NaOCl, Siqueira Júnior et al.19 reported that 0.12% CHX and 2.5% NaOCl presented comparable results relative to bacterial elimination from infected root canals in vivo. The present study was unable to confirm the in vitro findings of Ohara et al.21 and D'Arcangelo et al.22, in which 0.2% CHX eliminated all microorganisms, including E. faecalis, because 0.2% CHX did not eliminate the microorganisms evaluated. In the present research it was noted that 1% CHX was effective in eliminating P. aeruginosa and C. albicans, but ineffective against S. aureus and E. faecalis, disagreeing with Sassone et al.23 where the 1% CHX showed antimicrobial activity against S. aureus and E. faecalis. There has been increasing concern regarding the insufficient antimicrobial efficacy of CHX against E. faecalis even after prolonged contact of the medication in the root canal5,16. These findings were observed in this study where the antimicrobial activity of 0.2%, 1%, and 2% CHX solutions in combination with the NiTi rotary instrumentation were not effective in eliminating E. faecalis. However, other studies have reported contradictory results regarding the efficacy of 2% CHX in eliminating E. faecalis2,6,20,22. Ruff et al. 24 found 2% CHX to be effective against C. albicans. Additionally, Huth et al.25 observed that 2% CHX was able to eliminate C. albicans and P. aeruginosa, which is consistent with the results of this study, where the 2% CHX was effective against C. albicans and P. aeruginosa. Because chemomechanical preparation is a short procedure, it would appear that the antibacterial effectiveness of the irrigant inside the root canal might be highly dependent on both, the concentration and type of irrigant used as well as the microbial susceptibility. Gomes et al.26 and Vianna et al.20 demonstrated that 0.2%, 1% and 2% CHX showed antimicrobial activity, and the time required by the 0.2% CHX to produce a negative culture was 30 s and less than 30 s for the 1% CHX and 2% CHX. However, Athanassiadis et al.7 reported that when CHX is used as an irrigating solution it has relatively short effective exposure time in the root canal and this does not allow the medication to exert its full antibacterial action. As a result, a large number of bacteria may persist within the dentinal tubules and remain viable. This occurred in the present research, since the mean instrumentation time for the ProTaper Universal™ system was 4.0 ± 1.0 min and the CHX did not exhibit its full antibacterial action when applied for a short exposure time in the root canal during irrigation. The present study did not investigate the residual effect of the CHX as it was neutralized by the addition of Tween 80 plus 0.07% lecithin. This study reinforces the importance of using irrigants with antimicrobial activity during the biomechanical preparation because in the positive control group, a 0.85% saline was used and showed no antibacterial activity, in accordance with previous works12,18. However, Berber et al.27 found that saline was able to remove microorganisms from the main root canal. In recent years, NiTi rotary root canal preparation systems, such as the ProTaper Universal™, along with several others, have altered the techniques of canal instrumentation10. The use of rotary NiTi files for root canal preparation helped shortening significantly the time required to instrument canals with minimal deviation from the original canal path compared with hand instrumentation8,9. Rollison et al.28 reported that only instrumentation with rotary systems without irrigating solutions was unable to remove all the bacteria from the root canal. In the same way as observe din the present study, Chuste-Guillot et al.29 evaluated the bacterial reduction of in vitro infected root canals after instrumentation by NiTi rotary files and showed that despite extensive instrumentation and antiseptic irrigation, bacteria could remain in the root canal, maintaining the endodontic infection. In this research, the 0.2% CHX solution in combination with the ProTaper Universal™ system was ineffective against all test microorganisms. The 1% CHX solution was effective in eliminating P. aeruginosa and C. albicans at the end of instrumentation after the use of the F1 and F3 instruments, respectively, but was ineffective against S. aureus and E. faecalis. The 2% CHX solution was effective at killing S. aureus, P. aeruginosa and C. albicans at the beginning of the instrumentation after the use of the S1 instrument, but was not sufficient to inactivate E. faecalis. In this study, due to anatomic variations and with the purpose of standardizing the final apical instrument, the root canals were instrumented up to instrument F3 to achieve size #30 for the apical preparation, which, according to Khademi et al.30, is the minimum instrumentation size needed for penetration of irrigants into the apical canal third. Further research should be carried out to evaluate if by increasing the final apical instrument diameter, microorganisms considered to be resistant to endodontic therapy would completely eliminated. This study investigated in vitro the antimicrobial activity of different CHX concentrations against some endodontic pathogens in root canals instrumented with the ProTaper Universal™ system. The 0.2% CHX solution in combination with rotary instrumentation was ineffective against all test microorganisms. The 1% CHX solution was ineffective against S. aureus and E. faecalis. The 2% CHX solution was not sufficient to inactivate E. faecalis. The conclusions of the present work are limited to the in vitro conditions of the study and should be confirmed by further in vivo investigations. Acknowledgments This study was supported by grants from Coordenação de Aperfeiçoamento de Pessoal de Nível Superior CAPES - Brazil. References
Copyright 2010 - Braz J Oral Sci The following images related to this document are available:Photo images[os10045t4.jpg] [os10045f2.jpg] [os10045t2.jpg] [os10045f3.jpg] [os10045t3.jpg] [os10045t1.jpg] [os10045f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}