 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Braz J Oral Sci, Vol. 9, No. 3, July-September, 2010, pp. 410-414 Trends in dental caries in 12- and 13-year-old schoolchildren from Florianópolis between 1971 and 2009 Helena Mendes Constante1, João Luiz Bastos2, Marco Aurélio Peres2 1 Undergraduate dental student, Federal University of
Santa Catarina, Brazil
Received for publication: May 19, 2010 Correspondence to: Marco Aurélio Peres Departamento de Saúde Pública, Centro de Ciências da Saúde Universidade Federal de Santa Catarina Campus Universitário Trindade - 88010-970 Florianópolis - SC Phone: +55-48-37219046 Fax: +55-48-37219542 E-mail: mperes@ccs.ufsc.br Code Number: os10046 Abstract Aim: To estimate the prevalence and severity of dental caries
in schoolchildren from the city of Florianópolis, SC, Brazil, in 2009
and to compare these results with data from previous studies carried out in
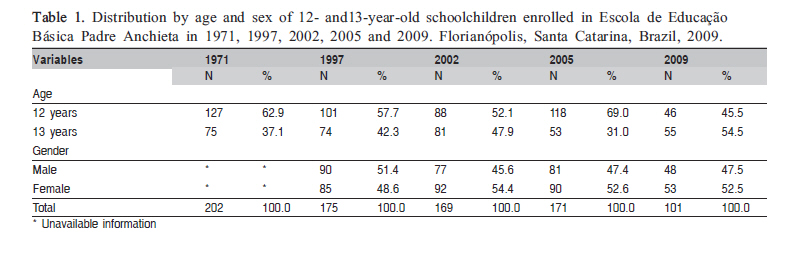
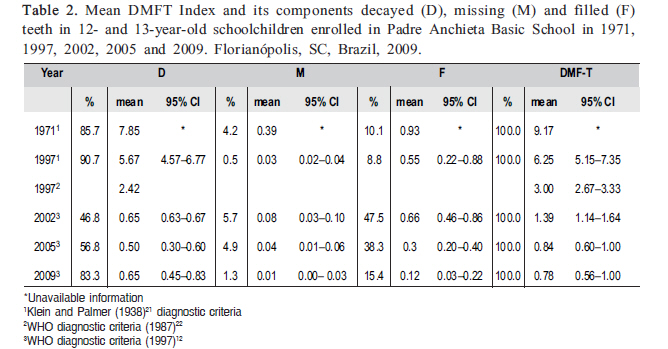
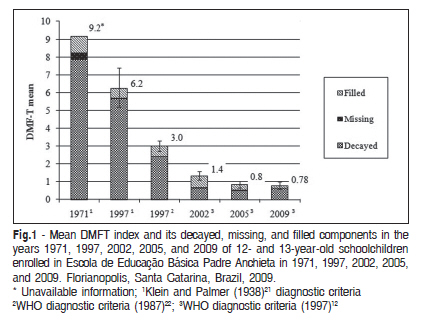
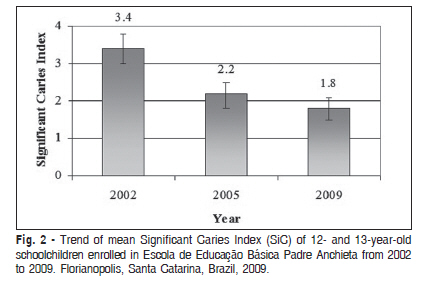
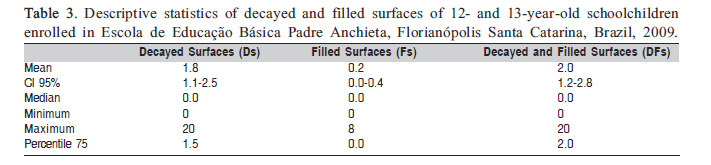
the same institution since 1971. Keywords: dental caries, DMF index, oral health, trends. Introduction The World Health Organization (WHO) holds epidemiological data showing a decline in the levels of caries experience in 12-year-old children in several countries in recent decades, including some from South America, such as Argentina, Chile, Uruguay, Paraguay, and Brazil. According to the WHO1, in 2004, the global mean DMFT (an index measuring counts of decayed, missing, and filled permanent teeth) was 1.61. In Brazil, the mean DMFT was 2.8 in 2002-2003, although almost 70% of the Brazilian children aged 12 years and nearly 90% of adolescents aged between 15-19 years presented at least one permanent tooth with dental caries experience, according to the Brazilian Ministry of Health2 and the WHO1. A bibliographic search carried out in PubMed and Scielo using "dental caries" and "trends" as descriptors, limited to the period between 2004 and 2009, showed that several studies in Brazil documented declining trends in the mean DMFT in 12-year-old adolescents. In the city of Bauru, SP, Bastos et al.3 observed that the dental caries decline was of 84.5% between 1976 and 2001. Gushi et al.4, using data from oral health surveys carried out with adolescents between 12 and 18 years of age in the state of São Paulo, observed a reduction of 32.3% in the mean DMFT between 1998 and 2002. In the city of Palhoça, SC, Traebert et al.5 observed a reduction of 41.9% in the mean DMFT index for adolescents in the same age group between 1997 and 2003. In the city of Goiânia, GO, the decline in dental caries was even greater, reaching 70.6% between 1988 and 2003, as Reis et al.6 reported. Studies carried out in the same school in 1971-19977, 20028, and 20059 in Florianópolis, SC, also demonstrated an expressive reduction in the severity (91.3%) and in the prevalence (58.2%) of dental caries. Worldwide, very few studies have monitored dental caries prevalence and severity in the same population group for a long period. In Australia, Armfield et al.10 conducted a study with schoolchildren enrolled in public and private schools from 1977 to 2002 and observed a reduction of 79% in the experience of dental caries throughout 25 years. In Somerset, United Kingdom, Anderson11 reported that the mean DMFT declined by 80% in 12-year-old adolescents from two schools, between 1963 and 1988. The monitoring of dental caries over time is a part of oral health surveillance system; it is important to subsidize health planners to implement and evaluate preventive programs and dental care. The aim of this study was to evaluate the prevalence and severity of dental caries in 12- and 13-year-old schoolchildren from Florianópolis, SC, Brazil, in 2009 and to compare these data to the results obtained in previous studies conducted in the same school in 1971, 1997, 2002, and 2005. Material and methods The sample comprised all 145 students 12 and 13 years of age, enrolled in a public school (Escola de Educação Básica Padre Anchieta) in the city of Florianópolis, state of Santa Catarina, Southern Brazil, in 2009. The same methodological procedures used in previous studies7-9 were adopted in the present investigation, including the collection of clinical data under natural light and using plane dental mirrors and periodontal probes (ball-end probes), following the diagnostic criteria recommended by the WHO12. The fieldwork team was composed of two undergraduate dental students; the first performed all dental examinations, whereas the second transferred clinical records to appropriate forms. Both were supervised and trained by an experienced dental epidemiologist (MAP) to ensure standardization of dental caries diagnosis, as well as to avoid discrepancies in interpretation of dental examinations. This calibration training consisted of repeated dental examinations on 15 subjects, followed by discussion on the dental caries diagnostics. This process was ended when the discrepancies were eliminated, and consistency in dental caries diagnosis was achieved among dental examiners. For this phase of the fieldwork, intra- and interexaminer reliabilities were not estimated. Because a remarkable decline in dental caries prevalence over the past decades has been observed, the DMFS index (number of decayed, missing, or filled permanent dental surfaces) was used as a diagnostic criterion, in addition to the DMFT index. A tooth surface was considered as "decayed" when a lesion in a pit or fissure or a smooth tooth surface presented an unmistakable cavity, undermined enamel, or a detectable softened floor or walls. A filled but still decayed surface was also included in this category. This index, recommended by the WHO12, also considered further areas with past experience of dental caries, recording those that received restorative dental treatment and those that have been extracted because of caries. According to the methodology proposed by Pinto13, the 28 permanent teeth were divided into 128 surfaces, as follows: molars and premolars with five surfaces (occlusal, mesial, distal, buccal, and lingual) and incisors and canines with four surfaces (mesial, distal, vestibular, and lingual). To record clinical data, the following sequence was respected: upper right (2nd molar to the central incisor), upper left (central incisor to 2nd molar), lower left (2nd molar to central incisor), and lower right (central incisor to 2nd molar). To analyze tooth surfaces, the examination started in the occlusal surface (O), followed by mesial (M), buccal (B), distal (D), and lingual (L) surfaces. Data were typed into a Microsoft® Excel spreadsheet. Statistical analysis was performed with Stata, v.9. The prevalence of dental caries, the mean DMFS index, the mean DMFT index, and their components were also estimated with 95% confidence intervals. The chi-square test was used to compare caries prevalence according to sex, and the Mann-Whitney U test was used to compare the distributions of DMFS according to sex and age. The significant caries index (SiC) was calculated based on the mean DMFT index of the highest DMFT tertile in the studied population14. A letter was sent to parents explaining the aims and importance of the study and asking permission for their children's participation. When the survey was completed, another letter was sent to acknowledge the participation of adolescents, to report any dental treatment needs, and to provide advices on oral health. The project was approved by the Ethics Committee for Human Research of the Federal University of Santa Catarina (protocol number 126249/2008-3). Results From a total of 148 eligible schoolchildren, 101 took part in the study (response rate of 68.2%). Losses were due to refusals (18.2%) and transferences to other schools, during data collection period. The distribution of the studied adolescents by age and sex in the present and previous studies is shown in Table 1. In 1971, 1997, 2002, and 2005, most of the schoolchildren were aged 12 years; this proportion ranged from 62.9% in 1971 to 45.5% in 2009. However, in 2009, 13-year-old children were more frequent (54.5%), when taking the 1971 study as a reference. The differences in caries prevalence by sex and age were not statistically significant (p = 0.4 and p = 0.1, respectively). Consequently, the results are shown for the sample as a whole. Table 2 displays the mean DMFT and its components, as well as 95% confidence intervals. In the present study, the mean D component was 0.65 (CI 95% 0.45-0.83), followed by the F component with 0.12 (CI 95% 0.03-0.22) and by the M component with 0.01 (CI 95% 0.00- 0.03). The mean DMFT index was 0.78 (CI 95% 0.56-1.00). In the later period of the present study (2009), the D component contributed most to the mean DMFT value, corresponding to 83.3% of the index. When compared to the percent composition of the DMFT index in the first study year (1971), there was a greater reduction of the M component (97.43%), followed by the D (91.71%) and F (87.09%) components in the present study. Caries prevalence, i.e. the number of participants with DMFTe"1 divided by all examined schoolchildren, declined from 98.0% (CI 95% 96.0-100.0) in 1971 to 93.7% (CI 95% 90.0-98.0) in 1997, when the Klein and Palmer (1938) diagnostic criteria were adopted. Between 1997 and 2002, and taking into account the WHO 1987 and the WHO 1997 diagnostic criteria, respectively, the caries prevalence decreased from 80.0% (CI 95% 74.0-86.0) to 57.4% (CI 95% 50.0-65.0). In the penultimate period of observation (2002-2005), caries prevalence declined from 57.4% (CI 95% 50.0-65.0) to 40.9% (CI 95% 33.5-48.4), according to the criteria set forth by the WHO12 in 1997. In the later period of the present study (2009), the dental caries prevalence reached 43.5% (CI 95% 33.7- 53.4). The average of DMFT index was 9.2 (CI 95% not available) in 1971, declining to 6.2 (CI 95% 5.2-7.4) in 1997, according to the Klein and Palmer (1938) diagnostic criteria. The mean reached 3.0 (CI 95% 2.7-3.3) and 1.4 (CI 95% 1.1-1.6) in 2002, when the WHO 1987 and the WHO 1997 diagnostic criteria were adopted, respectively. In 2005, the mean DMFT index was 0.8 (CI 95% 0.6-1.0), a value also observed in the present study (Figure 1). In 2002, the SiC index was 3.4 (CI 95% 3.0-3.8), decreasing to 2.2 (CI 95% 1.8- 2.5) in 2005 and to 1.8 (CI 95% 1.5-2.1) in the present study. This corresponds to a reduction of 47% (Figure 2). Table 3 shows that the mean decayed and filled surfaces in 2009 was 1.8 (CI 95% 1.1-2.5) and 0.2 (CI 95% 0.0-0.4), respectively. Seventy-five percent (75th percentile) of the adolescents showed a mean of decayed and filled surfaces (D and F) below 2. In 2009, the mean DMFS index was found to be 2.0, with an average of decayed surfaces of 2.3 in males and 1.7 in females, a nonsignificant difference. At the age of 13 years, an average of 2.7 decayed and filled surfaces was observed; at the age of 12 years, this average was 1.2. However, this difference was not statistically significant. Discussion Since 1971, when the first of this series of studies was conducted, until 2009, an effective decline in dental caries prevalence and severity was observed in the studied population Even though different diagnostic criteria were used along the studied period, a reduction of 91.4% in the caries severity was found in the 2009 study, when compared with the 1971 study. Compared to the 2002 study, which adopted the same diagnostic criteria, a reduction of 43.4% in the caries severity was observed in 2009. Despite the fact that the mean DMFT did not change between 2005 and 2009, its components presented contradictory proportions when compared with those observed in previous studies. The D component showed a reduction of 93.6% between 1971 and 2005, represented 83.3%of the DMFT in 2009, and showed a relative increase of 30% over the last studied period (2005-2009). These data may hypothetically indicate a decrease in dental care utilization in the region, a paradox considering that, for this period, the number of dentists in the city increased, achieving a ratio of 1 dentist for every 250 inhabitants in the city of Florianópolis in June 2009. A less invasive approach by dentists in the city may be another explanation for such a decline in the proportion of D component. The 2009 F component showed a reduction of 60% as compared with the previous study (2005) and comprised 15.4% of the DMFT index in 2009. The M component showed an even greater reduction (75%) since the last year of study, although it represents only 1.3% of the mean DMFT index in the current study. The mean DMFT was 0.78, reaching one of the WHO goals for the year 2010, that is, a mean DMFT below 1.0 for the age of 12 years, according to Gomes et al.15. It is noteworthy that there are few studies conducted in the same place for such a long period and under the supervision of the same research team. Marcenes et al.16 and Souza et al.9, suggested that the reduction observed in dental caries experience may be partially attributed to changes in diagnostic criteria for dental caries over time. In Brazil, similar decline in dental caries was demonstrated by other researchers. As stated by Martins et al.17 the city of in Bilac, SP, a similar reduction in the mean DMFT index was achieved, despite the lack of water fluoridation supply during the study period. According to Bastos et al.3 (2005), fluoridated water supplies contributed to the remarkable reduction in the mean DMFT in Bauru, SP. In fact, the results from the "SB Brazil: Oral Health in the Brazilian Population" held in 2003, produced by Ministry of Health2, revealed that in the South region - an area with high water fluoridated coverage - presented 37.7% of caries-free adolescents aged 12 years, in contrast to only 12.9% of caries-free adolescents in non-fluoridated regions. Worldwide, similar reductions in caries experience have been documented. Armfield and Spencer10 (2008) analyzed data from dental caries in adolescents enrolled in public and private schools between 1977 and 2002 in Australia and found a reduction of 79% for the age of 12 years. In this same study, an annual reduction of 2.6% the SiC index between 1977 and 2002 for the same age was observed. These values were lower than the ones found in the present study (annual reduction of 6.7%). In Lithuania (1993-2001), Aleksejûnienë et al.18 (2004) reported that the decline in dental caries rates may be explained by an improvement in oral hygiene because products for this purpose began to be sold in 1991 and had an increase of 95% in their use in 2001 in that country. The US Centers for Diseases Control and Prevention19 declared that the fluoridation of water supplies is a the most effective mass intervention to prevent dental caries, and it was considered one of the most important public health achievements in the last century. In addition to water fluoridation, the major decline in dental caries prevalence and severity has been attributed to the access to other fluoride sources, especially to the widespread use of fluoridated toothpaste. Moreover, an improvement in socioeconomic indicators and the boost of initiatives in dental public health also have been listed, by Bastos et al.3, Ministry of Health20, Martins et al.17, as important to dental caries reduction over time. As stated by Bastos et al.3 and Martins et al.17, the use of fluoridated toothpaste in Brazil was intensified from 1989, when the Ministry of Health regulated the addition of fluoride in these products and mouthrinses. Possibly, according to Freysleben et al.7, Bastos et al.8 and Souza et al.9, these factors contributed to a higher rate of annual reduction in the dental caries severity over the periods that followed the studies through the 1990s in Florianópolis. However, the design of this study does not allow an assessment of the possible reasons for the decline in dental caries prevalence. In the first period (1971 to 1997), in which the lowest annual reduction rate was observed compared with other years, this could be explained, as noted by Freysleben et al.7, by the shorter period of public exposure to fluoridated water, implemented in Florianópolis in 1982, and the availability of use of fluoride toothpaste from the late 1980's. In 1971, the school was located in a suburban area of the city, which became, in 1997, a middle class region with a residential profile and close to the city's downtown with better living conditions. In the second studied period (1997 to 2002), the caries decline can be attributed to the increased availability of fluoridated toothpaste and to the implemen-tation of fluoridated water supply. Additionally, Florianópolis in 2003 occupied the third position among the capitals with the lowest level of social exclusion in Brazil. In 2008, Bastos et al.8 reported that Florianópolis appeared as the city with the highest human development index (HDI of 0.86) among 33 other Brazilian metropolitan areas and cities and presented the highest average income among Brazilian cities. Despite the observed declining trend in dental caries over the studied period, different authors10-11,18 found that the disease rate is likely to stabilize because of the low value already reached. Some limitations of this study must be mentioned. The 2009 study had a relatively low response rate, lower than those observed in the previous phases. We can hypothesize that the mean DMFT could be higher, assuming that individuals who were not examined presented higher dental caries attack than those who effectively took part in the study. In conclusion, despite the fact that different dental caries diagnostic criteria were used, there was an actual decrease in the mean DMFT over the 38-year study period. It should be noted that these results cannot be readily generalized to the entire population of 12 and 13 years of age from Florianópolis, SC. Acknowledgments Helena Mendes Constante was supported by a scholarship granted from the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) of Brazil from November 2008 to July 2009 (number 126249/2008 3). References
Copyright 2010 - Braz J Oral Sci The following images related to this document are available:Photo images[os10046t1.jpg] [os10046t3.jpg] [os10046t2.jpg] [os10046f1.jpg] [os10046f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}