 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
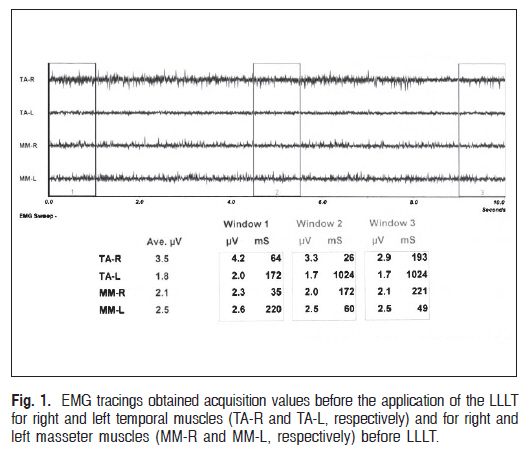
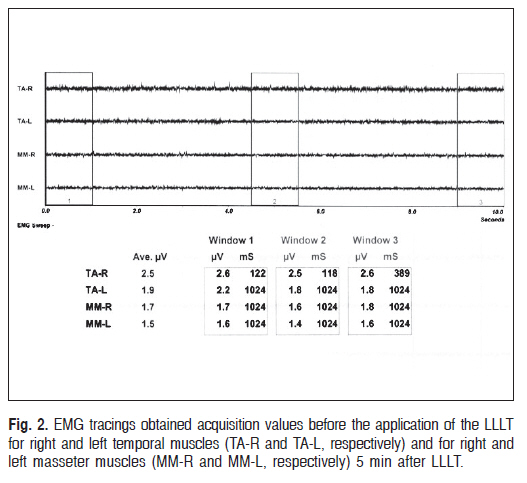
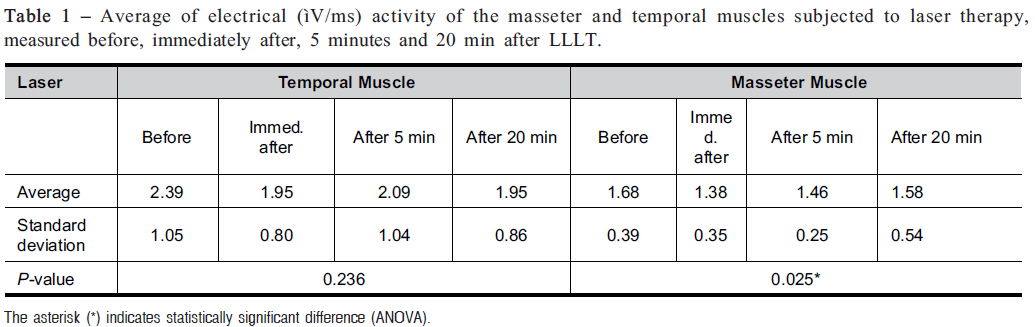
Braz J Oral Sci, Vol. 9, No. 4, October-December, 2010, pp. 434-438 Clinical assessment of the efficacy of low-level laser therapy on muscle pain in women with temporomandibular dysfunction, by surface electromyography Ewerson Bertolini Shinozaki1,2 , Mateus Bertolini Fernandes dos Santos 3, Luiz Kioaki Okazaki 2 Leonardo Marchini 2,4,5, Aldo Brugnera Junior1 1 DDS, MSD, PhD, Dental Laser Center, Institute for Research and Development, Universidade do Vale do Paraíba, São José dos Campos, SP, Brazil. Recieved for publication: March 17, 2010 Accepted: September 10, 2010 Code Number: os10050 Abstract The use of low-level laser (LLL) may be an useful tool to promote reduction of muscular pain caused by TMD. Keywords: temporomandibular dysfunction, low-level laser, electromyography. Received for publication: March 17, 2010 Correspondence to: Mateus Bertolini Fernandes dos Santos Rua Engº João Fonseca dos Santos, 123/34, São José dos Campos 12243-620, SP, Brazil Phone +55-19-8830-9867 Fax +55-12-39221555 E-mail: mateusbertolini@yahoo.com.br General clinicians and even specialists in orthodontics, prosthetics and oral and maxillofacial surgery have been treating a growing number of patients complaining of pain in the region of the temporomandibular joint (TMJ), which may be diagnosed as temporomandibular dysfunction (TMD). Very often, these patients have already consulted doctors of other specialties in an attempt to solve painful symptoms in the muscles of the head, face, neck, and shoulders. Orofacial pain is particularly stressful because this area is powerfully represented in the cerebral cortex1 . TMD is a term used to define the clinical joint and muscle disorders affecting the maxillofacial region. These dysfunctions are characterized firstly by pain, articular noise and irregular or limited mandibular functions. They are the main cause of nondental-related pain in the orofacial region2 . The correct diagnosis is crucial in planning TMD treatment, since its etiology is multifactorial and the treatment of these dysfunctions covers a wide range of interdependent variables that are often interdisciplinary2-4 . The treatment of TMD basically consists of occlusal corrections involving teeth drilling (occlusal adjustments), use of occlusal splints, physiotherapy, psychological advisory, orthodontic or prosthetic rehabilitation2,5-6. Low-level laser therapy (LLLT) acts as an adjuvant in the treatment of the dysfunction, promoting the reduction of muscular pain caused by muscle hyperactivity and/or mandibular displacement2 . The markedly analgesic, anti-inflammatory and stimulating effects of LLLT are characterized by increased production of â-endorphins and control of the production of prostaglandins7-8. The application of laser beams diminishes pain while simultaneously reducing muscle contraction. When a local effect is desired, laser is effective by stimulating microcirculation and local cell tropism or, when a general therapeutic effect is needed, by promoting pain relief for a variety of etiologies, including irradiation of trigger points in microfacial pain, acting on tissue repair, reduction of edema and hyperemia9-10 . This work involved a clinical assessment of the immediate efficacy of low-level laser therapy on women displaying signs and symptoms of TMD, using surface electromyography. We hypothesized that LLLT promotes muscle relaxation. Material and methods Subjects The sample consisted of thirteen 18 to 36-year-old women presenting spontaneous facial pain at rest, exacerbated during the function; limited mandibular opening (<45 mm) and alterations in the trajectory of movements evidenced by lateral deviations; moderate to severe sensitivity to manual palpation of the masseter (superficial) and temporal (anterior bundle) muscles; muscular weakness and fatigue. All patients answered a questionnaire regarding about TMD and only the subjects diagnosed with TMD were assigned to this study. The pain was also assessed by the same questionnaire, which was applied before and after LLLT. During the experiment, each patient remained in the same room and was attended by the same operator. This study was evaluated and approved by the Ethical Committee of the University of Vale do Paraíba for the use of human subjects (Protocol number L170/2004/CEP). All subjects signed an informed consent form before participating in this study. Electromyographic (EMG) measurementsEMG measurements were taken with a surface electromyograph (Model MP100, BioPAC system, Bio-Research Assoc. Inc., Milwaukee, USA) with 8-channel amplifier (model 800); this equipment present a Common Mode Rejection Ratio (CMMR) of 110 dB (50/60 Hz), low (500Hz) and high (20Hz) pass filters and 16 bits of resolution. Surface silver/silver chloride electrodes of 10 mm diameter (Duotrodes; Myotronics Co.) were used to measure the electrical activity of the right and left temporal (anterior bundle) muscles and the right and left masseter (superficial) muscles, it was used a low pass filter in order to retain signals in the range of 10 to 350 Hz for surface electrodes11 . The protocol proposed by Macaluso and deLaat in 1995 was followed for the electrodes location12. Before their placement, the skin of the patients was cleaned with liquid soap suitable for skin cleansing and soon after with ethyl alcohol 70ºGL. The electrodes were placed on the muscles in the region of highest volume and parallels to the long axis with a distance of 21mm between them. A single monopolar electrode with a neutral point function (grounding cable) was also used in the neck region. The data were carefully recorded simultaneously and bilaterally. Before starting the measurements the equipment was always calibrated with a trial test, which is necessary to verify the correct state of the electrodes and connections. The first recording was performed during 10-ms. The electrical activity of the four muscles simultaneously appears reflected. Thus, we obtain a reference value of the state of the muscles at rest which can be achieved by the patient by one’s own means by simply responding when being asked to relax13. For this, we calibrated the screen reticule to a range of 30 ìV/div and a speed of 1 ms/div. Each patient underwent EMG tests at resting position of the superficial masseter and anterior temporal muscles. The record of the EMG activity at rest was measured for a period of 10-ms with five-fold amplification. After recording the EMG activity of the right and left masseter (superficial) and temporal (anterior bundle) muscles, the electrodes were removed and their exact location marked so that they could be put back on exactly the same spot after LLLT. Immediately after application of the laser (as described below), the electrodes that had been removed were placed back on the marked locations and the entire above described procedure was repeated to record the electrical activity of the aforementioned muscles after the laser therapy, thus obtaining the second EMG record. The third and fourth records were obtained after 5 and 20 min, respectively. The patient was allowed to rest, seated comfortably but keeping the electrodes in place, and the muscles were then monitored following the above described protocol. All data of the electrical activity of the muscles in rest, prior to the low-level laser therapy, immediately after, 5 and 20 min after the therapy were recorded automatically by the computer. The EMG tests were performed on the side that the patient reported increased pain on muscles, the other side of the patients were used as a placebo treatment. LLLTThe LLLT was applied using a Bio-wave device (Kondortech) with 40 mW power, gallium aluminum arsenide (GaAlAs) diode laser, 790 nm wavelength, beam delivery system by direct contact with the skin, and a beam area of 0.2 cm2. The low-level laser irradiations were applied pointwise on standardized TMJ points: head, anterior, posterior, superior and inferior portions of the mandible, each of which received an application of 1.5 J/cm2, and posterior to the TMJ at the height of the outer ear, the region through which the auriculotemporal nerve and bilaminar zone pass, where 2.5 J/cm2 was applied. The masseter muscle (superficial and anterior bundle) received 3 J/cm2 of laser energy pointwise on three predetermined points of the muscle, superior, median and inferior in case of superficial and anterior, and median and posterior in the anterior bundle. Data analysisThe data, average of rectified signals, were processed with the software BioPak for Windows, and then examined by one-way ANOVA to check possible correlations between EMG results and the LLLT. Whenever ANOVA indicated a difference, Scheffe’s multiple-comparison method was used to identify the existing correlations. Student’s paired t-test was also applied to analyze each muscle. All the tests were performed at a P<0.05 level of significance. ResultsEMG tracings obtained acquisition values before and five minutes after the LLLT is presented in figures 1 and 2. The mean and standard deviation of the results obtained by electromyography at the abovementioned times are shown in Table 1. A statistical difference was found among the times in masseter muscle (P=0.025). Therefore, Scheffe’s multiple-comparison method was applied, indicating a statistically significant difference between the EMG activity before and immediately after LLLT application (P=0.013). Discussion EMG as well as clinical examinations and application of questionnaires are efficient methods for evaluating and diagnosing TMD3,14. The severity of pain cannot be reflected in EMG activity, but since limited mandibular movement heightens muscle tonus activity, TMD patients present a slight increase in basal muscle tonus which is detected electromyographically, confirming that EMG is an effective tool for evaluation and diagnosis in the treatment of these dysfunctions3,7. In a comparison of normal and TMD patients, Gervais et al.14 demonstrated that individuals presenting TMD have increased EMG activity in the painful muscles and, hence, a shortening of the fibers of these muscles. The results of the present study demonstrated the effectiveness of LLLT in promoting relaxation of the masseter muscles, resulting in the relief of pain produced by muscle contraction in women suffering from TMD. Nunez et al.8 also found an improvement in the mandibular motion of patients with TMD immediately after LLLT. However, we should consider some of the limitations of the present study, such as the limited sample size. Other important limitations for clinical application are the TMD diagnostic criteria, instrumentation, electrodes and equipment used in this study, and the fact of only women were evaluated. According to Simunovic et al.15, the muscle relaxation and the analgesic effects of LLLT are due to factors such as the increase of endorphin production and elevation of pain threshold through an electrolytic blocking mechanism of the nerve fibers. On the other hand, Bertolucci and Gray16-17 believe that these effects are due to increased cell metabolism accompanied by a gain in energy due to the transformation of ADP into ATP in the cells exposed to the laser beam, reducing the painful symptoms. We agree with the latter authors insofar as it concerns the mechanism of laser action in producing muscle relaxation and analgesia. LLLT can help removing metabolites and increase blood flow to muscles in painful conditions through local vasodilatation18-19 . Hunter et al.20 stated that there is a cell response to the application of LLLT through increased intracellular calcium. LLLT promoted immediate relaxation of the masseter muscles in a single session. Conti21, in turn, stated that laser therapy increased mandibular mobility, reducing and stabilizing pain after the third day of application. The rapid reduction of intra-articular and muscle inflammation achieved with infrared laser contributes toward stabilization of the occlusion and to symmetry of the muscle functions, which influence reparative processes22 . Similarly, Bertolucci and Grey16-17 reported significant improvement in articular noise, in limitation of oral opening, and in the masticatory function through reduction of muscle contraction and of intra-articular inflammation by LLLT4 . Conti21, on the other hand, reported relief of painful symptoms only in cases of myogenic dysfunction, while patients with arthrogenic pain showed improvement only of their mandibular functions. Kulekcioglu et al.23 stated that the effects of the therapy on cases of myogenic and arthrogenic dysfunction were similar. In view of the noninvasive action of LLLT, it can be considered a useful tool in the treatment of TMD, although further studies are required to define reliable clinical parameters21. The correct diagnosis and an appropriate application protocol are key factors to enable LLLT to produce positive effects24 . This study also proposes the use of an GaAlAs laser emitted at a wavelength of 790 nm and power of 40 mW. The sessions should vary according to the severity of the pathology and the painful symptoms. The laser beam should be applied to the TMJ at four points around the joint, using an ED of 1.5 J/cm2 on each point, and at a fifth point in the region of the outer ear, through which the auriculotemporal nerve passes, with an ED of 2.5 J/cm2. Muscles with painful symptoms should be treated with the laser beam applied pointwise with an ED of 3 J/cm2 at three predetermined points on the masseter and temporal muscles. Within the limitations of this study, it is possible to conclude that women with TMD subjected to laser therapy present a reduction of the EMG activity in both the masseter and temporal muscles. The proposed LLLT promoted significant immediate relaxation of the masseter muscles, measured electromyographically. References
Copyright 2010 - Braz J Oral Sci The following images related to this document are available:Photo images[os10050t1.jpg] [os10050f2.jpg] [os10050f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}