 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Braz J Oral Sci, Vol. 9, No. 4, October-December, 2010, pp. 443-448 Medical and dental absenteeism in workers from a furniture industry in Itatiba, SP, Brazil Cristina Gomes de Macedo1, Dagmar de Paula Queluz2 1DDS, Master student, Piracicaba Dental School, State University of Campinas (Unicamp), Piracicaba (SP), Brazil Received for publication: June 16, 2010 Correspondence to:Dagmar de Paula Queluz Departamento de Odontologia Social Faculdade de Odontologia de Piracicaba –UNICAMP Avenida Limeira, 901 CEP 13414-900 Piracicaba SP Brazil Phone: +55 -19-2106 5277 E-mail: dagmar@fop.unicamp.br Code Number: os10052 Abstract Introduction: Absenteeism is a matter of growing interest due to the current
economic competitiveness and leads companies to seek means to minimize its
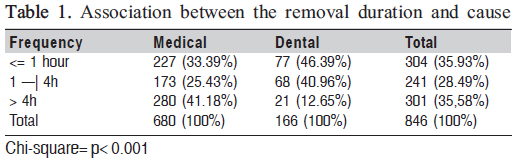
occurrence in order to increase the profitability and productivity. Keywords: absenteeism, workers, sick leave. IntroductionThe term absenteeism is used to designate the absences of workers at work process, either by lack or delay, due to some intervening reason. Absenteeism has become a crucial problem for both private and public organizations and their administrators, which causes a quantitative impact on human resources and reflects on the quality of service provided1-3 . The individual workers (and their dependents) many times see their income reduced due to absenteeism, especially in long-lasting cases. Absenteeism at work also has a negative effect on the national economy as a result of potential loss production due to reduction of the available labor force and the increased costs of medical treatment and social security4 . Work should be considered by the worker not as an obligation, but as a form of growth, interpersonal development, enhancement of skills, abilities, sharing of experiences. Worker should feel happy with his/her activity, the working environment and with his/her co-workers. Presenteeism is an even worse organizational problem because the worker is physically present at work, but he/she is not producing due to multiple variables and factors such as: dissatisfaction, pessimism, discouragement and high stress level, making it harder to identify the problem, and causing harm to the industry and to other workers who are often contaminated by this apathy and lack of productivity. Gaidzinski5 (1994) developed a study to grade the staff services, and classified absences as foreseen and unforeseen. The first class of absences if formed by those that are granted by law and that may be planned in advance, such as vacation, retreats and holidays. Unforeseen absences effectively characterize absenteeism due to their unpredictable nature, such as unjustified absences, medical licenses, accidents, maternity and paternity licenses, mourning, specialization courses and other situations that prevent a worker of staying at the work place. In any case, this phenomenon causes not only direct, but also indirect costs, caused by decrease in productivity because fewer workers are active. This will reduce the quality of service since another worker has to cover for the missing one, certainly decreasing the efficiency and effectiveness of the expected results. Another classification of absenteeism presented by Midorikawa6 (2000) discusses the aspect of lack at work and absenteeism where the worker is only physically present. The first can be measured and has its cost calculated by the absence of the individual. The second, which cannot be measured, is when the worker cannot perform his usual tasks because of any kind of pain. The World Health Organization (WHO) recognizes that pain, suffering, psychological and social constraints may result from oral diseases, leading to losses at the individual and collective levels7 . Oral problems are directly related to lost working days. Workers with lower wages and minorities are disproportionately affected. Oral health is undeniably important for appropriate standards of quality of life. Brazilian dental health indicators of the adult population, indicate a high caries incidence, a significant number of teeth loss in young adults, great need for use of prostheses and severe periodontal problems8 . Dental absenteeism in Brazil is very difficult to evaluate because the relevant documents are not duly stored. There are few statistically processed data to measure the absenteeism for dental reasons1-3. Data are scarce about both the economic burden that such losses may entail and the worker’s dissatisfaction by breaking the health-work binomial9 . According to Nardi10 (2005), although dentists have been empowered to certify dental facts and their consequences since 1966, they were allowed to issue certificates to justify sick leaves only 9 years later. The Federal Council of Medicine Resolution nº 1.851/ 2008 regulates the issuing of medical certificates11. According to the Law 5.081, art. 6- I, dated August 24 1966, it is within the dentist’s scope to attest, in their professional activity and other unwholesome states, including justification of absence to employment. The Dental Ethics Code classifies as infringement of professional ethics to issue a certificate that does not correspond to the facts or in which the dentist did not participate12. Thus, from the ethical point of view, it is unacceptable to issue a certificate that is incompatible with the truth, for which only a professional who was involved in patient care can testify and, after the due examination of the real condition, determine whether a certificate is required. A dental certificate may not be refused for any reason, if it obviously meets all the required conditions to ensure that the referenced document can be accepted: who is the dentist that actually treated the patient, if the dentist is legally empowered for dental practice, understood as having professional qualification, possession of a legal document certified by records at the competent offices; not to have his/her practice suspended by judicial decision; not be the dentist suspended the profession by virtue of penalty imposed by the Regional Council of Dentistry12 . The dentist can have a printed form especially for the issuance of certificates, or, as commonly practiced use plain paper, which must contain the dentist’s professional qualification, the registration number in Regional Council of Dentistry and address. Never should the professional issue a certificate in advance, since the document can be use for purposes other than those mentioned by the requester. The purpose of the certificate must be specific, whether for school, sports activity or to justify absence at work. The term of absence shall be entered in full stating clearly the number of days stipulated by the professional12 . In the current context of economic competitiveness, sick leave, mainly if related to oral health, is a cause of growing concern for businesses, since only with a strict control and care of these factors they can reach a significant increase in profitability. Studies have shown that caries and other oral diseases are responsible for 20% of work day loss, and decreased productivity and directly affect the worker’s selfesteem and quality of life. The aim of this study was to identify the main factors involved with medical and dental absenteeism between 2005 and 2008 in a furniture industry in the city of Itatiba, SP, Brazil. Material and methodsThe sample of this study was composed of dental and medical certificates and duly approved presence declarations, issued between January 2005 and 2008, and delivered to the Human Resources Department of a furniture industry, whose purpose was to vouch for sick leave up to 15 days. The research protocol was reviewed and approved by the Research Ethics Committee of the University of Campinas (UNICAMP); protocol number 009/2009. This was a descriptive cross-sectional study in which all medical and dental certificates issued in the proposed time span were reviewed. The data collection was carried out in the industry and the variables in the dental and medical certificates were: activity, date of the certificate (year and month), International Classification of Diseases (ICD) code, absence duration (hours), certificate type (medical or dental), declaration variations, and completeness. Questionnaires were applied to all employees without exclusion criteria to study the demographic profile with variables focusing on: gender, age and education level. The collected data were automatically tabulated using Excel software13 and analyzed statistically by SAS14 . ResultsIn the evaluated period, the industry had 170 workers with a variation of 10 to 15 workers per year spread across sectors such as polishing, glaziers, maintenance, carpentry, sorting, warehouse management, human resources, budget, purchases, projects, gatehouse and expedition. One hundred and eleven workers replied to the questionnaire (65.2%), being 84.6% men (n=94) and 15.3% women (n=17) with mean age of 31.4 years. The education level of most employees was high school (53.2%). Twentythree (21.5%) workers completed only elementary school, while incomplete elementary school was the education level of 15 (14.0%) workers. The manufacturing activity involves the largest number of workers in the factory (n= 72; 64.82%) and covers the following areas: polishing, maintenance, glass factory, carpentry, sorting, warehouse and management. Other areas covered in the study are reception, administration, and projects and correspond to a total of 39 workers (35.18%). The Brazilian furniture branch consists predominantly of traditional familiar and national capital enterprises, counting about 50 thousand formal industries. In the 1990’s Brazil diversified its commercial ties and this branch was encouraged to modernize the industrial processes and imported machinery and equipment, mainly from Italy and Germany, with resources made available by the National Bank for Economic and Social Development,. The branch had an explosive growth of exportations, and Brazil is currently ranked #18 among furniture exporting countries, which represents 1.5% of world exports of that branch15 . According to the National Classification of Economic Activities, the furniture industry belongs to the Group c-6, wood, National Classification of Economic Activities 36 110, presenting degree of risk 3 in the Regulatory Standard no.4, in a 1 to 4 scale16 . In this study, 943 certificates were reviewed, being 775 (82.2%) medical and 168 (17.8%) dental documents. There was a predominance of males (n= 751, 79.6%) over females (n=192, 20.4%). In 2005, 137 (14.5%) medical and dental certificates were delivered to the Human Resource Department, in 2006 they were 242 (25.6%), in 2007, 325 (34.6%) and in 2008, 239 (25.3%). There was no statistically significant association between the number of certificates and the different months and years examined (p>0.005). The ICD code was not mentioned in 618 (65.5%) certificates. The remaining 325 (34.5%) certificates contained the ICD code, being 241 (74.1%) medical certificates and 84 (25.9%) dental certificates. Among the certificates with the ICD code, dentists were more concerned in providing this information (50%) compared to physicians (31.1%). In all dental certificates, a single ICD code was used, K-525-8, which means: “other diseases and disorders of the teeth and its support structures.” In the medical certificates four categories of ICD presented greater frequency: Group M-musculoskeletal system diseases and connective tissue (n=41, 17%), Group J – respiratory diseases (n=32, 13.3%), Group R – symptoms signs and abnormal in clinical examination and laboratory (n=27, 11.2%) and Group K – digestive diseases (n=17, 7%). Regarding the duration, most justified absences from work due to dental and medical reasons lasted up to 8 hours (n=846, 89.7%) and only 97 (10.3%) cases lasted over 8 hours to 5 days. The loss of working time was 7098.5 work hours and 887.3 work days considering an 8-hour working day. The types of documents presented to the Human Resource Department to justify sick leaves included consultation, ambulatory service and exam, vouchers (n=284, 30.1%), hospital vouchers (236, 25%), incomplete medical/dental certificates issued by he professionals (199, 21.1%), and recipes with fill full recipes syndicate category complete and incomplete as to fill totaled 224 (23.8%). There was a statistically significant association (p<0,001) between the sick leave duration and its cause. Dental certificates prevailed in absence duration up to four hours, whereas leaves of absence over four hours prevailed in the medical certificates (Table1). Discussion Whatever the driving economic activity of a developing country, the instrument for the final objectives pursued depends on the work carried out by humans. This fact reveals the interest of the authorities of the country in relation to the workers’ health, regardless of their level of work. The dental and medical certificates are the only legal instruments that justify sick leaves and ensure full payment of the wages. Distribution of absenteeism as regards age, gender, education level is required. Other important data are the duration and the cause of absences. The availability of such information is very important for planning the different strategies of prevention. In our study, we found in both the social demographic profile and the analysis of certificates, a prevailing population of young males with a high education level for the standards of a developing country. It is clear that the variables gender, age and education level, if considered alone, contribute to the understanding of absenteeism globally, depending on the type and workplace studied. On the other hand, they provide important information when the analysis is restricted to a specific enterprise, providing subsidies for searching solutions to decrease absence at the work place17 . Grzywacz and Butler18 (2005) rank the schooling as the most important component of the socioeconomic condition for determination of health-related behaviors. High levels of schooling are generally associated with better housing and employment, income and socio-economic position. In a study on absenteeism for dental and medical reasons in public and private services, in the city of Araçatuba, SP, Brazil, the dental certificates had little weight on the total certificates, both in the public (3.3%) and in the private (6.3%) services. Due to lack of ICD codes in almost all dental certificates, the reason for most worker absences in both public and private services was pain (ICD M 54)19 . The present study also found a predominance of medical rather than dental certificates, but a greater concern by the dentists relative to placing of the ICD code. In medical certificates the prevalent ICD codes were from Group M, which deals with diseases of the musculoskeletal system and connective tissue. Reisine and Miller20 (1985) analyzed the effects of dental conditions on social functioning by measuring the incidence of work loss days associated with dental problems and treatments. A longitudinal study of 1992 employed adults in the Hartford, Connecticut, USA, was conducted. Participants were interviewed at baseline to collect data on sociodemographic, health care and health status factors and were followed for 1 year to assess the incidence of dental work loss days. The results showed that 26.4% of the sample reported an episode of dentally-related work, with a mean of 1.26 hours per person per year. The results suggest that work loss days may be a useful population statistic in measuring oral health status because of the high prevalence of dental disease. Mazzili and Crosato21 (2005) published a survey to investigate the prevalence, incidence and the average absence from work for dental reasons, according to the variables of interest to healthcare, performed by nosologic group and in accordance with the International Classification of Diseases and related health problems. Data collection was held in the Medical Department of the administration secretary of São Paulo between December 1996 and December 2000. The results indicated greater prevalence of females, most often aged 20 to 29 years, and the main reasons were: dental extractions, pulp diseases periodontal diseases, temporomandibular joint disorders and extractions of included or impacted teeth. Requests for absence for dental reasons in the studied population were gender- and agedependent, according to the study in proportions. Acute conditions or post-operative were the most frequent causes. Chronic conditions represented, however, the greatest impact on total days of absence. In the conducted study it was not possible to assess the main reasons of absence by dental causes, because most of the evaluated certificates had a single ICD (525-8, other diseases and disorders of the teeth and their structures). In cooperation with the Fondazione Maugeri of and the Fondazione Ospedale Maggiore Policlinic, Milan, the local health unit in Italy, conducted a research project, sponsored in part by the Italian Ministry of Health about damages in work-related upper limb muscle-skeletal system in a specific sector of a manufacturing industry of upholstered furniture. This “Upholstered District” is widely represented approximately 14,000 workers in 500 factories over a large geographical area of southern Italy. Advanced technology of manufacturing process is combined with workers engaged in intensive tasks of hand and arm. The risk groups were: workers of preparation, operators of leather-cutting, sewing and workers assembling upholstery padding. Data collected in private companies of different size this extensive industrial area emphasize the importance of prevention through appropriate ergonomics solutions and the need to improve training program covering the entire area22 . There was no significant prevalence in the certificate analysis of the respiratory system diseases (n = 32, 13.3%). Workers in industries where wood is processed are exposed to mechanical activities employing different types of tools, machines and various chemical substances. An example related to working conditions is the trauma suffered by the mutilation of one of the members or other permanent impairment. Often insurance intended for protection of victims and ensuring a fair indemnity as the degree of the problem and results in revolt and exacerbates the feeling of less value because it does not match the actual loss both in their physical and psychological aspects. The loss of one of the fingers, for example, does not imply only in press movement’s inability, for example, but also implies a set of hand signals that can cause social constraints23 . Taking into consideration the risks in this segment of the industry, the following items are of extreme importance in medical certifications: proximity to rotating elements, noise, effects of chemicals or biological factors, including carcinogenic substances (wood dust). For these reasons the procedures involved in medical/dental examinations are very complex24 . Although influenza vaccine is considered effective in preventing influenza and its complications, there are controversies about the advantages of its use in healthy adults. This survey was developed to characterize the common occurrence of respiratory problems, particularly the flu, and evaluate a program of immunization against influenza between workers. It was a study of cross-sectional delineation with industry workers. Data were collected on sociodemographic and respiratory problems. Occurrence of the flu in the past year was characterized and the vaccine was assessed. Among the 446 respondents, 18.3% presented strong incidence of flu and 11.7% were dismissed from work due to influenza. Overall, 70% of the employees noticed that there was an improvement in the occurrence of flu after vaccination. The positive assessment of vaccination made by workers and the low occurrence of side effects support the maintenance of the current program against influenza. However, several questions still persist about the economic advantages of vaccine, indicating the need of further studies on this subject25 The developed societies reached the understanding that the preservation of health and physical integrity of workers provides personal well-being, family and social, as well as results in greater productivity for the company and reduce expenses with insurance and indemnities, etc. Ensuring the physical and mental health of the worker is no longer seen as an act of charity, and has assumed the international features of social obligation, insofar as the prevention of accidents and occupational diseases decrease absenteeism and collaborates to the increase of national production, reducing spending with social security affairs26 . The conducted study revealed that most of the sick leaves were up to 8 hours, which usually is not insufficient time to cure any disease. It can be a work day loss due to a simple lab test or minor procedure, but it can also be “disease caused”. Medical and dental licenses are often used by the worker as a form of aggression against the chiefs and the institution. It also represents an escape for social, economic and psychological tensions. It is a critical point to be attacked in the struggle against absenteeism27 The Federal Council of Medicine resolution no. 1.851/ 2008 that regulates the issuance of medical certificates11 has established that the physician should specify the granted leave of absence time required for the recovery of the patient; establish the diagnosis, when expressly authorized by the patient; inform legibly the date and his/her full name, sign the certificate and stamp or put in writing the number of registry in the Regional Council of Medicine11. When the certificate is required by the patient or his legal representative for the purposes of medical expertise it must contain: the diagnosis, the results of complementary examinations, conducted therapy, prognosis; consequences to the patient’s health, the estimated rest time necessary for recovery, legible certificate date, and full identify of the health professional. The employee may leave the service without loss of wage and with term provided for by the law for a period of up to 15 (fifteen) days in the case of absence by illness or accident by a medical certificate and observed the law tax benefit. Any type of medical certificates does not require the industry to receive their absence to the service, unless the hypothesis of employed pregnant woman which should be exempted from working hours for the time necessary for holding at least 6 medical consultations and other additional tests, according to art. 392, subparagraph II of Working Law Code. An expressive number of declaration variations (n=284, 30.1%) in the total of medical and dental certificates in our study were approved by the Human Resources Department. The loss of productivity and competitive capacity of industries are directly linked to the number of working hours lost compared to those that are planned. The absenteeism has long been simply treated by focusing on the certificates that justified the absences of workers. However, we know today that several factors within and outside the industry, affect the absenteeism. Some factors are manageable and may, with the due care, reduce significantly the risks in the planning of the companies. The first step is to quantify the losses and identify the factors that generate them. As an example of internal factor causing faults is the lack of clarity in the personnel management policies (what is the benefit and what is legal compliance is often not clear to the worker), the lack of comfort at the desk, valuation of the professional, the pace of work, the ranges, accidents and incidents. The Programs of Medical Control of Occupational Health, as described in NR-07, promotion and preservation of workers’health, are based on tracking and prevention, early diagnosis of grievances on the work-related health, in addition to noting cases of occupational disease or irreversible damage to the health of workers. All data obtained during medical examinations and diagnostic findings must be registered in individual clinical records and kept for a minimum of 20 years after the worker leaves the premises, according to the Regulatory standard 7.4.5.1 item No. 728 . Prevention programs of environmental risks –NR-09 must include the recognition of environmental risks (physical, chemical and biological agents) occurring in working environments and which are capable of causing harm to workers’health, as well as the implementation of control measures. Health promotion at work is valuable in ability to promote well-being and productive in terms of fewer absences on grounds of illness. Activities involving the exercise, the quality of life and the ergonomics are potentially effective. And psychological applied alone does not seem effective. Health promotion at work should have a joint action between the physical and psychosocial environment29 . Invest in the well-being of the worker is much more than putting social responsibility; it should be seen as a protection to the business, which may be slowing down due to improper observation of people management. Thus, it is understood that the management of human resources is a strategy and may be the great competitive differentiator in most industry branches30 . In conclusion, based on the obtained results and considering the applied methodology, is that: 1- The absenteeism in the furniture industry was more frequently due to medical rather than dental reasons; the fouls and long duration of absences from work lead to problems arising from the reduced number of employees to complete the tasks at the work place; 2- There were several certificates lacking the International Classification of Diseases; 3- The number of lost work hours due to medical and dental problems was found to be a significant economic factor. References
Copyright 2010 - Braz J Oral Sci The following images related to this document are available:Photo images[os10052t1.jpg] |
| |||||||||

{kind=link}