 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Braz J Oral Sci, Vol. 9, No. 4, October-December, 2010, pp. 475-480 Prevalence of periodontal disease in special needs patients at APAE-PF/RS and the effect of local prevention programs Micheline Sandini Trentin1, Soluete Oliveira da Silva2 , Maria Salete Sandini Linden3, Bruna Hickmann Motta4, Janaína Rigo Panazzolo4, João Paulo De Carli5 1 PhD, Professor, Departament of Oral Medicine, Dental School, University of Passo Fundo, Passo Fundo, RS, Brazil Received for Publication: August 3, 2010 Accepted: November 12, 2010 Code Number: os10058 Abstract Aim: The objective of this study was to assess the prevalence and severity of
periodontal disease and the efficiency of oral health programs in patients
with special needs under treatment at APAE/ PF-RS (Association of Parents and
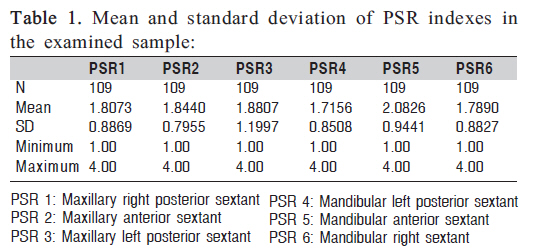
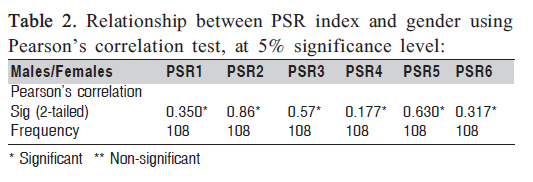
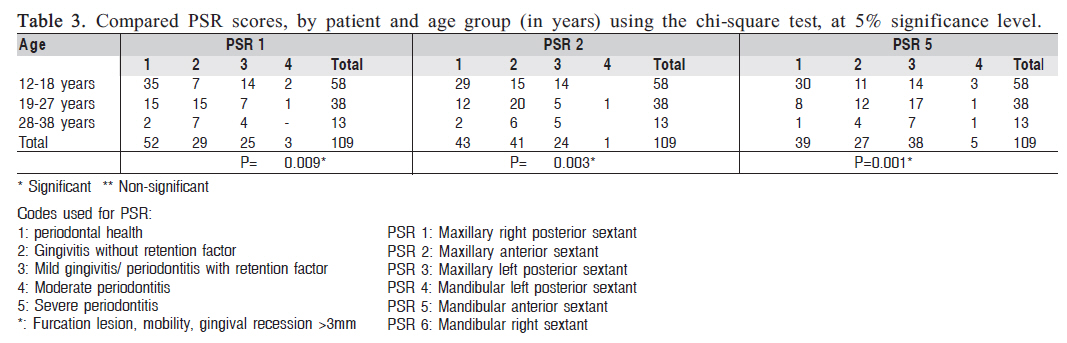
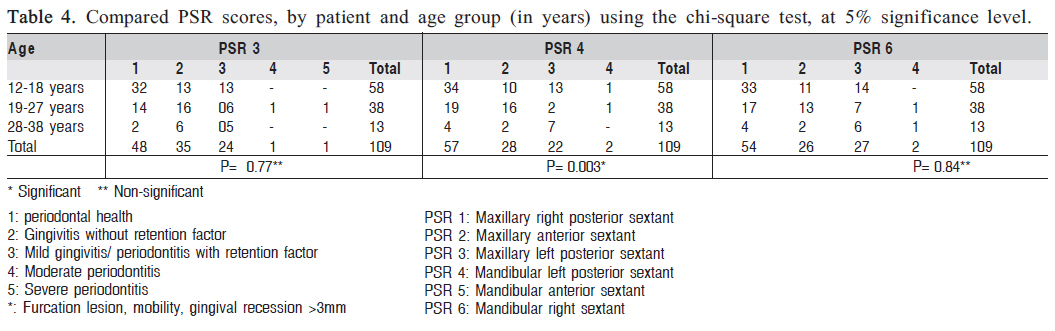
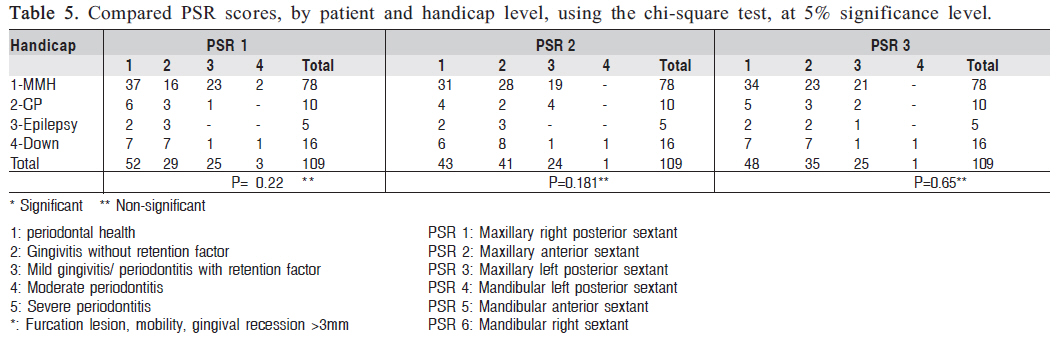
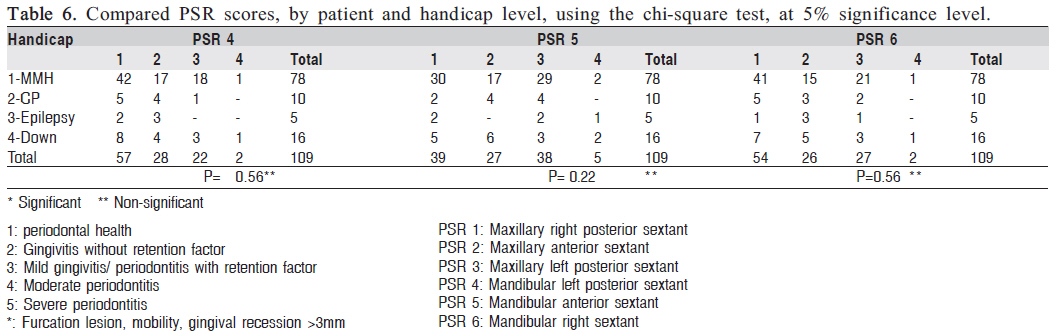
Friends of Special Needs Individuals - Passo Fundo/RS). Keywords: special patients, periodontal disease, PSR, prevention programs. IntroductionA special needs patient is every individual, adult or child, who deviates physically, intellectually, socially or emotionally from what is considered normal with regard to patterns of growth and development, and who therefore cannot receive a standard education, requiring instead special attention and supplementary instruction in an adequate manner for the rest of their lives1. In the context of dentistry, individuals with special needs are included in a segment of patients considered special because, due to their deviation from the standard of normality, they require special attention and specific approaches during a period of their lives or indefinitely2 . Studies have identified a high prevalence of periodontal disease in special needs patients2-5, with several factors that justify this occurrence. According to Carvalho and Araújo2 (2004), it is related to local and general factors, and can also be affected by the use of psychoactive medications, especially anticonvulsives2 . For Down syndrome, the occurrence is justified by a weakening in defenses associated with a reduction in the chemotaxis of neutrophils and monocytes, low neutrophil phagocytosis, and reduced T and immature T cell count6 . Moreover, local factors such as mouth breathing - which reduces the action of saliva, increases plaque accumulation and dehydrates gingival tissues, leaving individuals more susceptible to periodontal infection - and the composition of bacterial plaque microbiota can also influence the onset of periodontal disease7 . The lack of motor skills can also contribute to this high prevalence, but it is not the only justification, as the majority of these patients are not aware of the need for oral hygiene due to their intellectual limitations. Therefore, prevention programs against oral disease should have the goal of reestablishing not only oral health, but also the overall health of special needs patients. This should be done by raising awareness in each individual, the group and caregivers, and whenever possible, through motor skills training for oral hygiene as well as guidance on the alternatives for individuals with limitations. In addition, the integration of a multi-disciplinary team acting together is necessary not only to care for these individuals, but also to fulfill their citizenship2 . Furthermore, when considering activities at APAE (Association of Parents and Friends of Special Needs Individuals) and with special patients, it can be said that patients feel most unhappy when going to the dentist. Therefore, there is the need for preventive-educational programs, through the integration of dentist/special patient/family, in order to turn the visit to the dentist and oral health care into events with positive characteristics8 . The Continued Extension Project in Dentistry already exists for nearly 10 years at APAE/PF-RS, in the city of Passo Fundo, RS. It has been developed by volunteer third- and fourth-year dental students from the Dental School of the University of Passo Fundo. Once a week, the students work under coordination of the faculty members in order to provide instructions for oral hygiene and supervised toothbrushing. The group also gives lectures about different oral health issues to parents and teachers of the school, aiming at improving the oral health conditions of these patients. The objective of this study was to verify the prevalence and severity of periodontal disease in special needs patients who attend APAE/PF-RS in the city of Passo Fundo, Rio Grande do Sul, relating age, gender and handicap level to oral health prevention programs directed to these patients. Material and methodsThe present study was developed at the Dental Clinic of APAE/PF-RS, between 2006 and 2008, and was approved by the Research Ethics Committee of the University of Passo Fundo, under protocol number 320/2006. The students’ parents or guardians signed an informed consent form authorizing the students to take part in the research study. The cross-sectional study consisted of a convenience sample of 109 students, as the study attempted to examine all patients who regularly attended the school (n=250) and were over 12 years of age, in order to avoid a bias with regard to primary and permanent dentitions, as recommended by the World Health Organization9 (2002). The exclusion criteria consisted of patients under 12 and over 38 years of age, as well as patients with physical-motor disabilities, in order to obtain a homogenous sample. Periodontal clinical evaluations were done by two undergraduate students from the Dental School of the University of Passo Fundo-RS, previously calibrated for the Periodontal Screening and Recording (PSR) index, with 90% intra- and inter-examiner agreement, with 1 mm variation between measurements. The periodontal clinical exams were done using a dental mirror and a WHO periodontal probe (WHO-621), which is an especially designed lightweight metal probe with a 0.5 mm ball tip, with a band between 3.5 mm and 5.5 mm, specific for the evaluation of the PSR index10. The dental arches were divided into sextants for the periodontal clinical exams. Next, the highest code was recorded for each sextant, as well as for the patient. At least six regions were examined in each remaining tooth. The codes used for the PSR index were: 1: periodontal health; 2: gingivitis without retention factor; 3: mild gingivitis/periodontitis with retention factor; 4: moderate periodontitis; 5: severe periodontitis; and *: furcation lesion, mobility, gingival recession > 3mm. PSR sextants: PSR 1: Maxillary right posterior sextant A social-demographic questionnaire identified variables such as age, gender and handicap level: Age In order to recognize differences of age among the APAE students, the stratification by age has been performed. In this regard, the 12-year-old students are important for allowing an international comparison according to the oral health goals stated by the World Dental Federation and WHO 2002. The 19-year-old age group was chosen for allowing the comparison of its oral health conditions with the group aged 12 to 18 years. Data from students aged 2838 years will be also used for the same comparison, considering adult patients (aged 19-27 years). 1- Patients between 12-18 years of age; Gender: 1-Female Handicap level The classification of special patients from APAE was obtained through the medical records. These records were the same used by the physicians (neurologists) who work for that school. 1-Moderate mental handicap APAE/RS also conducts a continued extension project in Dentistry named “Promoting Oral in Special Needs Patients at APAE/RS”, in conjunction with FO-UPF and APAE-PF/RS, consisting of an oral health program for APAE students, where project volunteers promoted weekly supervised toothbrushing sessions under coordination of a dental school professor. There is also an institutional program performed by a dentist at the dental school’s outpatient clinic, where APAE students are weekly examined. This project has been conducted for 10 years at APAE and also counts on the support of teachers, physicians, nutritionists and psycholo-gists from the institution, forming a multidisciplinary team. The data collected were analyzed by SPSS 15.0 for Windows focusing on qualitative research. A descriptive analysis of data (percentile, frequency, mean and standard deviation) was performed, as well as a statistical analysis by chi-square at 5% significance level and Pearson’s t-test to verify the correlation of the variables age, gender, handicap level and PSR index. ResultsThe frequency and percentage of patients analyzed according to age were: age 1 (12-18 years), n=58 and 53.2%; age 2 (19-27 years), n=38 and 34.9%; age 3 (28-38 years), n=13 11.9%; totaling 109 patients (47 females and 62 males). Mean patient age was 19.79 ± 6.67 years, with minimum age of 12 and maximum of 38 years. Tables 1, 2, 3, 4, 5, 6 show the results obtained in the present study. Table 1 shows that the PSR indexes of the different analyzed sextants were very similar to one another. The lowest mean was reported for PSR 4 (mandibular left sextant): 1.7156; the highest mean was for PSR 5 (mandibular anterior sextant): 2.0826. Table 2 shows that the Pearson’s correlation test did not reveal significant differences between males and females as for the PSR index. Table 3 shows that in PSR 1 (maxillary right posterior sextant) of individuals between 12 and 18 years of age, there was a prevalence of periodontal health (35); in those over 18 years old, a prevalence of gingivitis without retention factors (15) (p=0.009) was observed, evidencing significant differences between these groups. In PSR 2 (maxillary anterior sextant), the value was significant (p<0.0032), with prevalence of periodontal health in patients between 12-18 years of age. In PSR 5 (mandibular anterior sextant), patients between 12 and 18 years of age showed better periodontal health than those in the older age bracket. Codes 2 and 3 (mild gingivitis/periodontitis with retention factor) were more prevalent in patients older than 18 years. These data were statistically significant by the chi-square test (p<0.001) Table 4 shows that in PSR 3 (maxillary left posterior sextant) of individuals between 12 and 18 years of age, there was a prevalence of periodontal health, and no individual showed periodontitis. In those aged between 1927, a prevalence of gingivitis without retention factor (16) and gingivitis with retention factor (06) was observed, and only one case of mild periodontitis (p=0.77), with no significant differences among groups. In PSR 4 (mandibular left posterior sextant), there was a greater prevalence of periodontal health (34), in patients between 12-18 years of age. In PSR 6 (mandibular right posterior sextant), patients between 12 and 18 years of age showed better periodontal health than those in older age groups. However, codes 2 and 3 (gingivitis without retention factor and gingivitis/ periodontitis with retention factor) were similar for the 1218 and 19-27 year old age brackets. No significant differences were observed in this study between the different handicap levels and the PSR index in the 6 sextants analyzed. It was observed, however, that individuals with Down syndrome, even in a smaller number, shower more advanced periodontal disease (code 4 – moderate) than patients with other handicaps. Patients showed the most difficulty with hygiene for PSR 5 and 6, given that the number of code 3 patients (mild gingivitis/periodontitis) was higher for those sextants (Tables 5 and 6). DiscussionThe objective of the present study was to assess the prevalence and severity of periodontal disease with regard to age, gender and mental handicap level of special needs patients at APAE/PFRS, as well as the effect of a preventive dental program at the site. This subject has been discussed in numerous clinical research studies. It can be observed in these works that special needs patients show higher prevalence and severity of periodontal disease compared to individuals without special needs7. Special needs individuals tend to show a more compromised oral health due to their physical, mental and social limitations, as well as to the use of systemic (psychoactive) medications, which can cause changes that lead to loss of oral integrity10 . In addition to patient-related factors, some of these studies correlate this high prevalence with socioeconomic conditions5 , as the families – often socially and emotionally marginalized –usually do not receive adequate oral health instructions, increasing the probability of developing oral diseases11-13 . The PSR used in this study is a system that allows for the examination of periodontal structures in a simplified and efficient manner to diagnose and evaluate the severity of periodontal disease, especially in this group of special patients. Most patients analyzed in the present study showed good oral hygiene conditions, and low levels of plaque and calculus, regardless of the handicap level. These data are in accordance with studies by Forseg et al.3 (1985) and Pregliasco et al.14 (2001), who showed that institutionalized patients have better oral health conditions that of non-institutionalized ones. These factors (low PSR indexes) compared to nationwide studies may be related to the interdisciplinary work that takes place at APAE/PF, featuring on-site dental assistance for over 15 years, and the Extension Program for Oral Health Prevention of FO/UPF, which has been conducted for 8 years. It is also important to mention the care given by the neurologists in the institution, who do not prescribe highdosage medications and restrict the use of phenytoin (anticonvulsive) in epileptic patients, in order to avoid gingival hyperplasia. Moreover, the work of speech therapists helps correcting aggravating factors such as mouth breathing, a work that has played a key role in the low rates of periodontal disease in this local population. Highlight is also given to the work of the school’s nutritionists, along with the multidisciplinary team, in devising a nutritive diet, reducing the levels of sugar in juices, chocolate drinks and porridges in order to avoid the development of caries and periodontal diseases. Most patients analyzed in this study showed moderate mental handicap and relatively low mean PSR index (1.742.08), average age of 19.79 years (47 females and 62 males). These results are also justified by the fact that most examined 54% of the students have attended the institution for over 20 years and 46% of them for 10 years. They are thus familiar with the school’s system. With regard to age, a greater prevalence of periodontal disease was observed in individuals older than 18 years, especially in those aged 30 years or more, for certain sextants (maxillary right posterior, maxillary anterior, mandibular anterior), as it is known that special needs patients in this age range presents rapid and extensive progression of periodontal disease when compared to those without special needs, especially those patients who do not have access to periodical treatment16-19 . Other factors that could be related with higher prevalence of periodontal disease are the fact that patients over 30 years of age receive less oral hygiene guidance and supervision than younger patients, and the fact that some of these patients are mouth breathers, which could cause dryness of mucosa and an increase in the levels of plaque and calculus in the mandibular anterior region. It is also known that depending on the type of handicap, for instance, neural-psycho-motor disturbances, severe occlusal problems may occur, resulting especially from reduced muscle tone (flaccidity), leading to changes in the maxillomandibular relationship11. For patients with Down syndrome, motor and neurological handicaps, macroglossia, along with reduced muscle tone, make oral hygiene more difficult, leading to greater susceptibility to periodontal disease. Nonetheless, a proven immunological deficiency may likely be the most contributing factor to the evolution of periodontal disease, as in these cases the body has difficulties combating the bacteria present in dental biofilm. Moreover, these patients present periodontal pathogenic bacteria such as Porphyromonas gingivalis, Bacteroides forythus, Provetela intermedia and Actinobacillus actinomycetemcomitans6-7,13,17,20-23. In this study, no significant differences were observed between the many different handicaps and the PSR index; however, when analyzed alone, individuals with Down syndrome showed more severe levels of periodontal disease than other patients; the fact that this was non-significant is perhaps due to the smaller sample of patients with moderate mental disability. According to Haddad11 (2007), because special needs patients are difficult to monitor, not only the effort in eliminating the source of periodontal infection, but also the control of the disease, must be regarded as a key factor due to its proven morbidity. The patients’ motivation with regard to oral hygiene should be valued, and the improved efficacy of at-home mechanical removal of dental biofilm should be requested by professionals. Carvalho and Araújo2 (2004) have stated that periodontal disease is the most prevalent oral pathology in institutionalized mentally handicapped people, especially as a result of their poor oral hygiene, justified by their motor and intellectual disabilities and by the incapacity of their patients in performing the mechanical removal of bacterial plaque correctly. The results of this study are encouraging, as there was prevalence of periodontal health in the majority of sextants. This is due in part to the existence of the extension program for oral health prevention, conducted weekly at APAE/PF-RS, with the objective of guiding the students about toothbrushing through practical and educational activities. According to Glassman & Miller23 (2003), these preventive programs that include videotapes and manual training for special needs patients, the regular professional assistance, control of dental plaque and diet, fluoride in water and sealant application, are effective measures to prevent dental disease in these individuals. Pregliasco et al. 14 (2001), in a study with 219 special needs patients, concluded that there is a need for special dental programs for institutionalized individuals with mental retardation, in order to reduce the rates of cavity and periodontal disease. Likewise, Martens et al. 24 (2000), in studies with 12-year-old special needs children, concluded that there is a need to train educators and parents on oral health programs. It is also important the implementation of educational programs on oral health directed to these patients, while integrating a multidisciplinary team, acting together, not only the care of these individuals, but also to fulfill their citizenship2 . It may be concluded from this study that the patients evaluated at APAE/PF-RS have a good level of oral hygiene, as in most analyzed sextants there was a prevalence of periodontal health, followed by gingivitis without retention factor, and only a small number of patients showed more severe levels of periodontal disease. These results can be attributed, in part, to the fact that the sample was homogenous and the individuals showed similar standards of oral hygiene and motor skills. Furthermore, we highlight another important factor: the existence of Extension and Interdisciplinary Programs for Oral Health Promotion, linked to the University of Passo Fundo (UPF), at APAE/PFRS. Due to their multidisciplinary nature, these programs can serve as models and be expanded to other similar institutions, making adaptations according to peculiarities. References
Copyright 2010 - Braz J Oral Sci The following images related to this document are available:Photo images[os10058t5.jpg] [os10058t6.jpg] [os10058t4.jpg] [os10058t3.jpg] [os10058t2.jpg] [os10058t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}