 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Braz J Oral Sci, Vol. 9, No. 4, October-December, 2010, pp. 481-487 Knowledge, practice and awareness of oral hygiene among three different age populations of same ethnic group –a community based study Mohd. Abdullah1, MD. Hassan Ali2, Shaik Rahiman3 1M.Sc, Department of Microbiology, College of Medicine, Al-Jouf University Correspondence to: Mohd. Abdullah, Department of Microbiology, College of Medicine, Al-Jouf University, Sakaka, Al Jouf, Kingdom of Saudi Arabia, PO Box 2014, Sakaka, Al-Jouf, Saudi Arabia. Phone: 00966535912208 E-mail: gulshanmicro@gmail.com Received for publication: May 10, 2010 Code Number: os10059 Abstract Aim: The objective of this study is to compare the knowledge, practice and awareness
of oral hygiene among three different age groups (15-30, 30-45 and 45-60-year-olds)
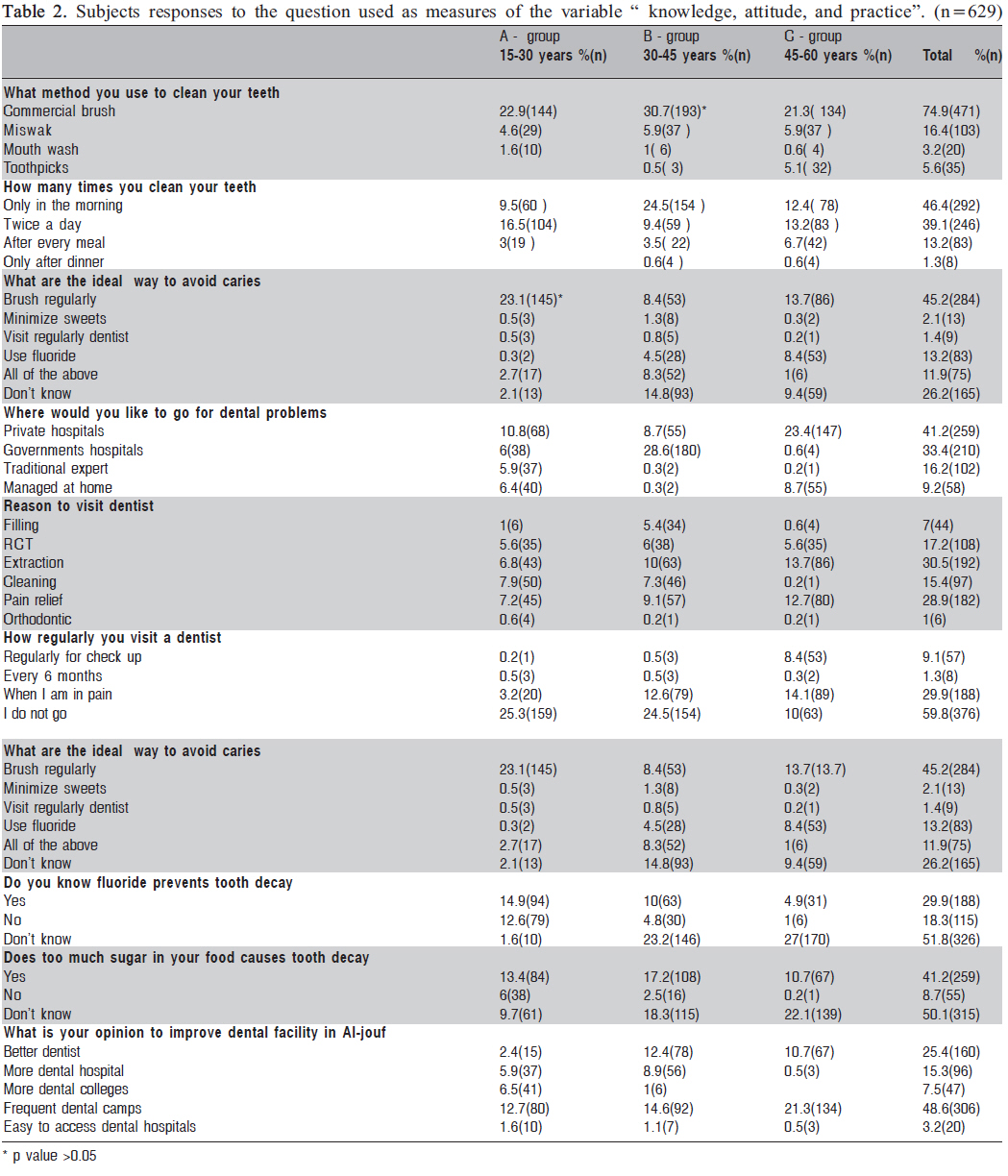
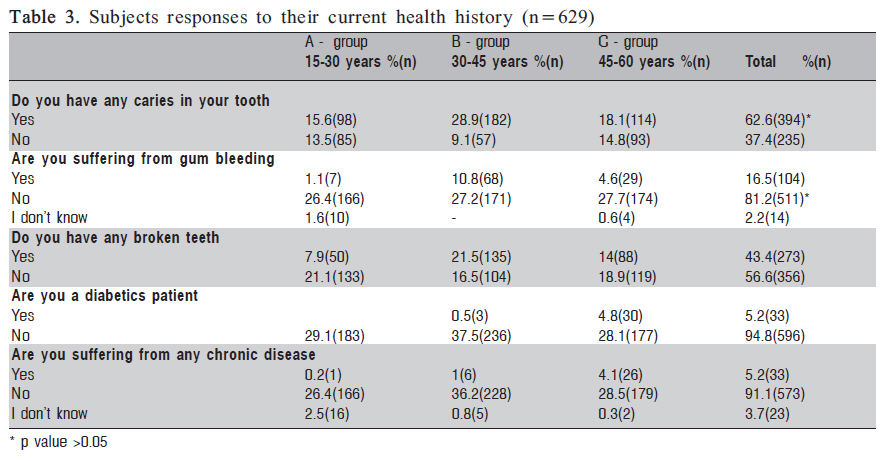
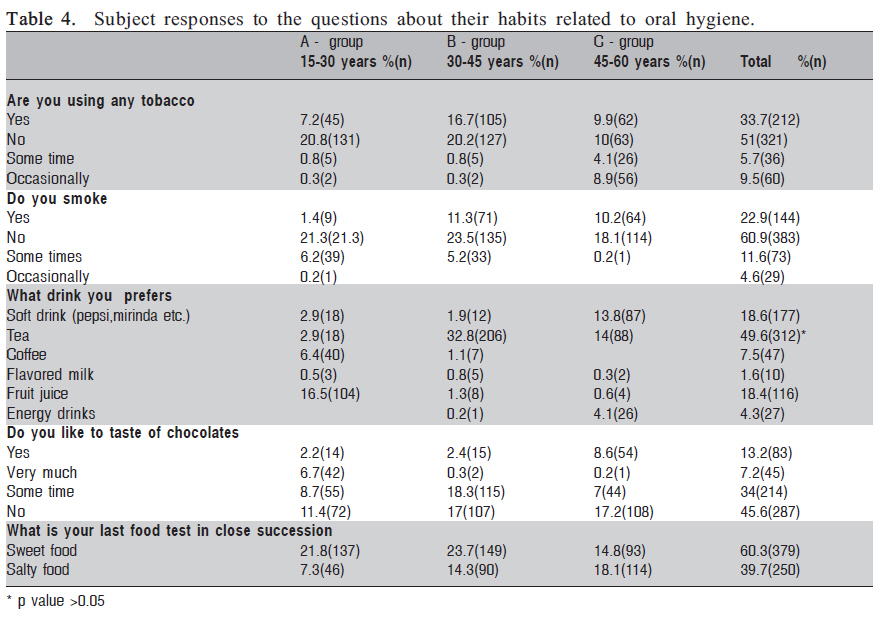
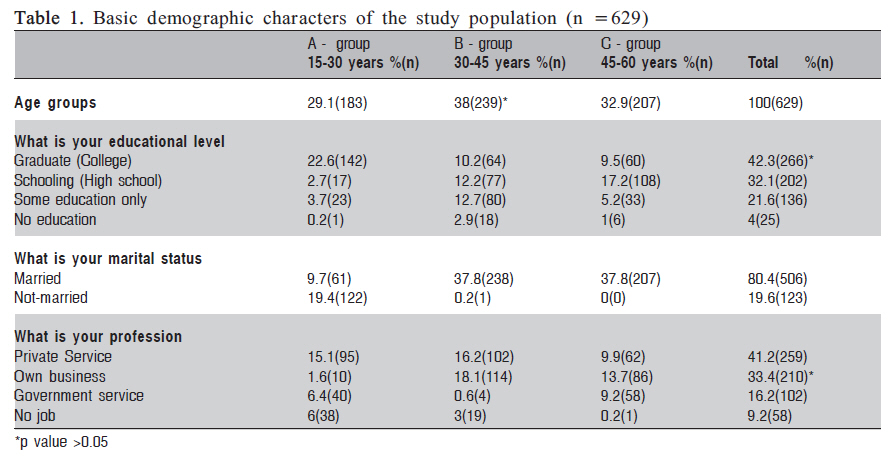
of the Saudi population in Sakaka. Keywords: knowledge, habits, dental caries, tooth brushing Saudi Arabia, ethnic group. Introduction The dental profession has limited resources to overcome barriers to oral health such as lack of oral health knowledge, access problem, and dental anxiety. Members of other health care professions are often in an appropriate position to give oral health counseling and help overcoming at least some of the barriers1. Oral diseases are the most common public health problems worldwide2. Their impact on individuals and communities in terms of pain and suffering, functional impairment and reduced quality of life is considerable and are the fourth most expensive to treat in most industrialized countries3 . One of the most common of the oral diseases is dental caries. Dental caries is an infectious and transmissible disease that results in the gradual destruction of enamel, dentin and cementum by acid forming biofilm microorganisms in the presence of sucrose4. It is one of the most common oral diseases showing marked geographical variation and severity of distribution all over the world5 . The prevalence is reported to be on the increase as a result of excessive sugar consumption especially in the developing countries6. In socioeconomically developing countries, the change from a traditional lifestyle to a Western lifestyle has, among other things, led to an increase in sugar consumption from food and beverages, and in the form of chocolate and candies7 Oral diseases are clearly related to behavior, and the prevalence of dental caries and periodontal disease has decreased with improvements in oral hygiene and a decrease in the consumption of sugar products. This general favorable trend in reducing dental caries, however, has not been seen in several developing countries8 or in the Middle East9 . While twice-a-day tooth brushing seems to be an established practice in several industrialized countries such as the United Kingdom10 and Norway11 , this goal is still very far from being achieved in several other countries, including Saudi Arabia9 and Turkey12. Numbers of factors have been put forward to explain the variation in prevalence and severity of dental caries and periodontal disease that can be found between developing and technically developed countries, and also between rural and urban communities. However, this relationship appears to be reversed in the developing countries13 . A number of studies have been documented on the oral health status and awareness towards oral health knowledge among the Saudi Arabian population14 . Oral health knowledge is considered to be an essential prerequisite for health-related behavior15 , although only a weak association seems to exist between knowledge and behavior in crosssectional studies16 . Nevertheless, studies have shown that there is an association between increased knowledge and better oral health. The present study evaluated the knowledge, practice and awareness about oral hygiene among three different age populations of same ethnic group (15-30, 30-45 and 45-60year-olds) of the Saudi population in Sakaka. Sakaka, is the capital city of the Al-Jouf province is located north east of Al Jouf province. The total population of Sakaka is 122,686 (as per last 2004 survey records). It is famous for agriculture and it is a central hub for commercial market in Al-Jouf province. Material and methodsA sample size of 850 male Saudi subjects aged between 15 and 60 years were chosen by simple random sampling technique. There age groups were formed as follows: group A: 15-30 years old, group B: 30-45 years old; and group C: 45-60 years old. The age intervals between the groups were 15±1 years. The instruments for collecting the data required for this study were a self-structured questionnaire and face to face interviewed method for those who were not educated. The content of the questionnaire was guided by review of literature on ways of maintaining dental health and reviewed by subject experts and dental specialists and medical specialists in Al-Jouf university, Sakaka, Al-Jouf , Kingdom of Saudi Arabia. The participation was voluntary and the answers were anonymous. The questionnaire was pre-tested on a convenience sample of 50 subjects, selected studied population. The questionnaire was modified based upon responses and the survey format was finalized. The questionnaire was organized into 4 sections. Section A had 4 questions elicited information on demographic attributes of respondents (age, marital status, profession and education level). Section B elicited information on dental health knowledge, practice and attitude. In this section, 10 questions were used to elicit their awareness towards oral-hygiene and the response followed by selection of one of the multiple answers. Section C had 5 questions related to their daily habits and the responses followed by selection of one of the multiple answers. Section D also had 5 questions to elicit information towards dental current health history and other health problems with a Yes / No response format. The questionnaires were administered with the assistance of three faculty members of the College of Medicine, Al-Jouf university, Sakaka, Aljouf, Saudi Arbia. On the spot administration and collection of questionnaire was adopted. The research work was carried out between January and March 2010. At the end of the survey, we collected 629 questionnaires with all filled questions. The remaining questions were incomplete, so we excluded those questionnaires for the sample. Data analysisThe data were analyzed using the statistical software SPSS for Windows version 17.0. The chi square (x2) test was used to examine the association between two categorical variables. Z test was used to assess the difference between the two proportions. Analysis of variance (ANOVA) was used for evaluation of the statistical significance. A p-value of 0.05 was used as a cut-off level for statistical significance. The multiple logistic regression analysis was performed to study the factors independently associated with the toothbrushing frequency. ResultsA total of 629 subjects responded this survey, most of the respondents belonging to B group (38%), while groupA had the smallest number participants (29.1%). The basic demographic data of respondents showed that 37.8% (238) of total were married subjects, and most of the respondents were aged between 30 and 45 years (x2 test, p<0.001). Most respondents had graduate level education 42.3% (x2 test, p<0.001) and only 4% were illiterates. Own business people responded more (18.1%) than private (15.1%) and government employees (9.2%) in the 3 age groups (x2 test, p<0.001). Table 2 summarizes the knowledge and oral hygiene among the three age groups in our sample. As regards practice to oral hygiene, 30.7% (B group; p<0.001) of total 74.9% (471) subjects preferred commercial brushes to clean their teeth; 5.9% (B and C groups) of 16.4% (103) choose Miswak for cleaning. Only 5.6% (35) used toothpicks in all age groups. Most of the B group people brushed their teeth only in the morning (24.5%). Regarding brushing twice a day, A group subjects were in higher ranking (16.5%). Only 1.3% of the subjects brushed only after dinner from all age groups. 23.1% (145) of A group subjects responded that brushing regularly was the ideal way to avoid caries (p<0.05). It is followed by 8.4% (53) C group subjects chose fluoride use as an ideal way to avoid caries. Most of the people (48.6%) preferred frequent dental camps in response to their opinion to improve dental facilities in Al-Jouf. 25.4% (160) subjects wished to have better dentist. Only 7.5% (47) people selected the variable of more dental hospitals and 3.2% (20) subjects liked to have easy access of dental hospitals. Table 3 presents the current dental health history of the respondents. Among the 62.62% (394) that reported having carious lesions, most were B-group subjects (28.9%) (p<0.05), while 37.4% subjects had no carious lesions. 81.2% (511) of the respondents were free from gingival bleeding (p<0.05); whereas only 16.5% (104) reported this problem. 43.4% (273) had fractured teeth and 56.6% (356) did not have. Table 4 shows that 60.9% (383) subjects were nonsmokers, whereas 22.9% (144) respondents were smokers from all 3 age groups. In response to preferable drink question, most of the respondents selected tea as the favorite drink (49.6%, p<0.001) and it was followed by the second preferable drink as soft drink (18.6%). 45.6% (287) of the subjects disliked chocolates whereas 34% (214) respondents desired to taste chocolates sometimes only. Regarding last food taste in close succession, 60.3% (379) subjects preferred sweet food whereas 39.7% (250) of the respondents choose salty food. DiscussionCaries was a disease of the economically developed countries with their refined carbohydrate consumption, and was of relatively insignificant in the poorer developing countries that subsisted mainly on natural farming products17-18 . Caries experience with age advancement might be due to mere exposure of teeth to the oral environment19 . The presence of caries in the B group subjects was significant (28.9%; p<00.5) compared to the other two age groups respondents. The use of tobacco (16.7%) and the smoking habit (11.3%) was highly prevalent in group B subjects (p<0.05). In addition to the effect of smoking on the oral hygiene, it is also associated with a variety of changes in the oral cavity and related to DIS in complete denture wearers. Cigarette smoke has effect on saliva, oral commensal microorganisms and opportunistic fungal infection in the oral cavity20 . As much as 23.7% of B group respondents selected sweet food as their last food taste in close succession (p<0.05). This showed a close relationship between their caries in teeth and their habits (p<0.001). There was in fact a more pronounced increase in tea consumption among 3045 age group subjects than other aged groups (p<0.001). When looking at the response concerning periodontal health, it is interesting to note that most of the respondents reported absence of gingival bleedings (81.2% ), mainly at the age between 30-45 years old, which is supported by previous studies21 . This might be due to their habit of tea consumption. Since, tea contains several naturally occurring substances that help prevent plaque and thus gum disease. The significance of broken teeth also highly reported in age group between 30-45-year-olds, while it was less reported in people aged 15-30 years. This paper focuses on describing differences among male subjects of three age groups in relation to their knowledge, practice and habits toward oral health. Concerning knowledge, most of subjects knew that the use of toothbrush help preventing periodontal disease. The findings on oral hygiene habits must be viewed with caution. Given the general state of living as observed during the study, the high response rate (74.9%, p>0.001) of those reporting using a toothbrush to clean their teeth in this study might not be accurate due to other external factors as suggested by Tijmstra22 . He states that other factors may have an influence in the findings of social sciences research. Amongst these factors is the problem of social desirability whereby respondents tend to answer questions on dental health and dental health behavior in a socially desirable way. A clinical oral examination may have been a useful tool to validate such findings. However, this concept of toothbrush method was also shared by others23. The present study revealed that most of the 15-30-year-old subjects performed the recommended practice of brushing twice a day. This level is similar to that observed in some industrialized countries of east Europe24 , but low as compared with most western industrialized countries25 . The same age group subjects responded that brushing regularly was the ideal way to avoid dental caries. The importance of regular brushing as a means of prevention is well documented26 . On the other hand age group C respondents had lack of knowledge towards oral hygiene practice. This is due to poor awareness of dental caries. Only 16.4% respondents were practicing miswak as their second method for tooth cleaning from all age groups. Because of the scientific merit of using miswak and the emphasis of using miswak as a cultural and religious belief among the Saudi population, the right method of using miswak as a cleaning technique to achieve maximum benefits should be stressed through various interventions27 . However, only 7% of subjects had filled teeth. This finding suggests that extraction of teeth (30%) was the main reason to visit dentist. It was supported by previous studies28 Such basic treatment procedures were reported in other studies in developing countries where few dental personnel and resources were available29 . Generally most of the respondents that visited dentists for extraction of teeth belonged to the age group of 45 60 years old. This was statistically significant (p<0.005). Dental pain was found to be the second reason for visiting the dentist among all the older groups, but it was the main reason among those aged 15-30 years old, which is supported by previous studies30 . Most of the C group subjects preferred private hospitals (23.4%) when they feel pain only. But B group respondents preferred government hospitals when they had the same problem. This denoted that the respondents tended to be satisfied with their own dental health and the appearance of their teeth, which may partly explain why most of them visited a dentist only when they felt a real need and not for regular examinations. This finding is similar to that reported in earlier studies31 . Only 1.3% respondents visited for dental check up every 6 months Although dental check-ups every 6 months are commonly recommended in many countries, there is no scientific evidence to justify this high frequency of dental visits, which can sometimes lead to unnecessary dental treatment32-33 . Although oral health knowledge does not necessarily relate to better health behavior, people who have assimilated this knowledge and feel a sense of personal control over their oral health are more likely to adopt self-care practices34 . This study revealed that only 14.9% of age group A respondents (14.9%) had an idea that fluoride prevent tooth decay, whereas knowledge of sugar in food causing dental caries was only 17.2% among 35-40 years old respondents. Interestingly half of the respondents in this survey had lack of knowledge of the effects of fluoride and sugar on dental caries (p<0.001). The low level of knowledge about fluoride use found among respondents might be the result of the limited emphasis placed on this preventive method by dental professionals35 . In this survey, 48.6% of total studied population responded dental camps to improve their dental health; the major of respondents for this option was aged between 45-30 years age old, followed by necessity of better dentists (25.4%), while the least option selected by study population was easier access dental hospitals (3.2%). The present study shows that a poorer knowledge and oral health conditions among 30-45 years aged subjects (Bgroup) compared to the other two groups. Generally, it might be due to the economic status, family and social environment, educational level, and also a change from a traditional lifestyle to a Western lifestyle along with the country development. An increase in the knowledge of risk factors for oral disease is important in oral health campaigns that aim to promote healthy habits. This will be achieved only if we have well aware subjects with number of oral health awareness camps and provide easy access to the advanced dental facilities. These data may be uttermost important in the evaluation of the past and planning of future oral health prevention and treatment programs targeting the high risk groups. Further studies are necessary to assess more effective . modalities of controlling dental caries in this population. AcknowledgementThe authors are thankful to Dr. Abdul Haleem, MD Ministry of Interior, Sakaka, Saudi Arabia, Dr. Hemant Bashkar, Asst. Prof, College of Dentistry, Jamia Millia Islamia, New Delhi, India who assisted in the preparation of questionnaire and helps in the evaluation of survey data and all the participants for their cooperation in this study. References
Copyright 2010 - Braz J Oral Sci The following images related to this document are available:Photo images[os10059t4.jpg] [os10059t3.jpg] [os10059t1.jpg] [os10059t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}