 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Braz J Oral Sci, Vol. 9, No. 4, October-December, 2010, pp. 493-497 Short implants with single-unit restorations in posterior regions with reduced height –a retrospective study Jamal Hassan Assaf1, Agenor Montebello Filho2, Fabricio Batistin Zanatta3 1DDS, MS, São Leopoldo Mandic Research Center, Dental School, Campinas, SP, Brazil Received for publication: July 15, 2010 Accepted: December 7, 2010 Code Number: os10061 Abstract Aim: Previous studies have shown excellent prognosis with short implants. However,
evidence of short implants rehabilitated with single-unit restorations is scarce.
The purpose of this study was to evaluate the percentage of success of short
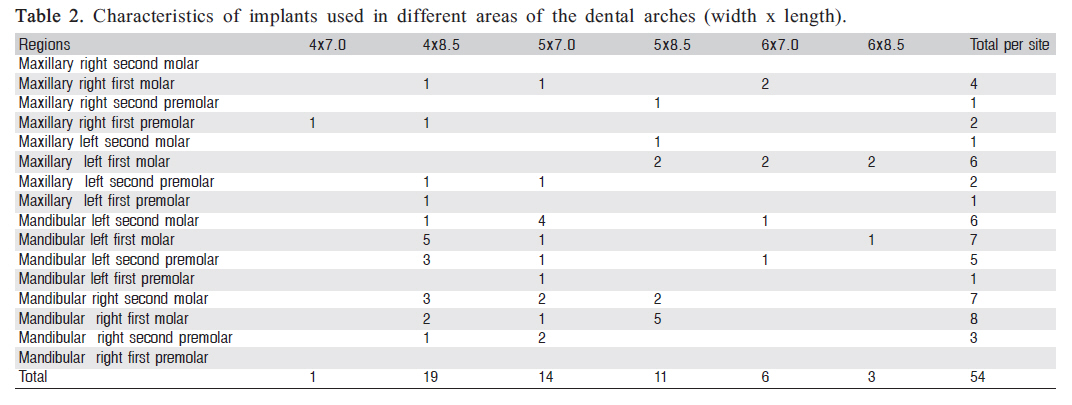
implants in posterior maxillary and mandibular regions with single-unit restorations. Keywords: short implants, single-unit restorations, success, retrospective study. IntroductionThe clinical use of several types of dental implants has been highly predictable in the last decades. However, its use may be restricted in the presence of limitations related to the morphology and volume of the bone ridge. These limitations are usually more common in the posterior maxillary and mandibular regions1. When the morphology and volume of bone ridge are insufficient for the placement of conventional implants, the treatment of choice comprises anatomical modification of the surgical site by the use of surgical techniques for bone augmentation. In the mandible, in some cases, the alveolar nerve must be displaced to allow the subsequent placement of long implants. This approach requires more complex surgical procedures with high morbidity rate, higher cost and longer time for final treatment2. Within this context, the placement of short implants in existing anatomical sites may be considered an appropriate option. The rationale for the use of short implants is that the osseointegrated interfacecontacting the bone tissue distributes a greater amount of occlusal load to the most coronal portion of the implant, compared to the middle and apical thirds1 . Some studies on short implants demonstrated greater occurrence of failure compared to long implants, with lower success rates for short implants3-5. Other studies revealed adequate success rates of short implants after 1 to 5 years of follow up6-9, ranging from 90 to 94.7%. These studies demonstrated that the posterior maxillary region exhibited the highest percentage of failures. However, no study described if single-unit restorations had been placed and the type of antagonist tooth. This information would be important, since there are doubts on whether short implants may support occlusal loads; if the implant is joined to another short or long implant, evaluation of the short implant as an isolated prosthetic unit is not possible10 . Regardless of that, it should be mentioned that the highest percentage of failure of short or long implants occur during the osseointegration period, in addition to a small percentage during the first year of load1,5-6,9,11-12. This study retrospectively analyzed short implants with single-unit restorations in posterior maxillary and mandibular regions with insufficient bone volume for the placement of long implants. Material and methodsUsing a retrospective design, this study included all patients attending a private dental office between June 2004 and June 2009, who were submitted to clinical and radiographic examination and required single-unit prosthetic rehabilitation in posterior maxillary and mandibular regions using short implants, due to reduced bone quantity in the sites of implant placement. All such cases were considered eligible for inclusion in the sample. Additionally, the following inclusion criteria were considered: no history of severe cardiac disorders, immune diseases, coagulation deficiencies, psychiatric and neurological disorders, severe metabolic diseases, bleeding on probing in any site of the mouth; radiotherapy and/or chemotherapy, smoking, or alcohol or drug addiction. Patients who did not attend the consultations after placement of the prostheses were excluded. The research protocol reviewed and approved by the Institutional Review Board (IRB) of São Leopoldo Mandic Research Center, Campinas, SP, Brazil (in accordance with Resolution n. 196/96 of the Ministry of Health National Council), under protocol #2008/0295. Data of 41 patients (17 males and 24 females), who attended the dental office of the investigator JHA, were reviewed by the analysis of records clinical interviews and clinical examinations had been conducted by the investigator. All patients evaluated were operated by the investigator with the aid of the same team, and all followup consultations were performed by the same investigator. ImplantsThe study analyzed clinical and radiographic data of Osseotite® 54 implants with treated surfaces (3i Implant Innovations, Inc., Palm Beach Gardens, FL,USA), being 17 implants in the maxilla and 37 in the mandible. Data on the characteristics of implants were obtained from individual forms containing identification of the series number, batch and specifications of all implants. Surgical stage and healing stageAll cases in the sample were performed according to the general surgical guidelines established by Branemark et al.13 , with specific indications as recommended by Buser et al.14 , Summers15-17 and Martinez et al.18. All surgeries were performed by an experienced surgeon (JHA) and the healing period ranged from 3 to 6 months. Prosthetic stageAll prosthetic reconstructions were performed by experienced professionals. The antagonist teeth were either restored or intact natural teeth, except for 6 mandibular implants whose antagonist teeth were conventional removable dentures and implant-supported dentures. Radiographic examinationsThe pre and postoperative radiographic examinations were conducted in radiology centers, and the computed tomography scans of preoperative examinations were obtained with a hospital tomography machine (Phillips®, Aura model, Pembroke Pines, FL, USA) and analyzed by the software Dentascan® , GE Medical Systems Milwaukee, WI, USA). The measurements were obtained from the bone crest of the maxillary sinus floor in the maxilla, and from the bone crest of the upper portion of the mandibular canal in the mandible. In some cases, measurements in the mandible were obtained from the bone crest of the submandibular notch. Clinical and radiographic evaluationEvaluation of the success of implants by analysis of the records followed the success criteria suggested by Esposito et al.19, including the following clinical and radiographic criteria: a) Absence of pain and sensitivity during placement of healing and prosthetic abutments, ruling out the possibility of pain due to the presence of gingival or mucous tissue between the implant platform and these devices; absence of pain during mastication and absence of pain and/or permanent sensitivity due to aggression to the inferior alveolar nerve; b) Absence of horizontal and vertical mobility. The occurrence of sensitivity during manual placement of provisional or healing abutments was carefully considered and the healing period was extended. In these cases, the provisional restorations were performed after this sensitivity had disappeared. In these cases, the final torque was applied after 6 months of function with the provisional restorations. The case was considered as successful when there was no pain or sensitivity during this period, and also when rotation mobility did not occur after final torque (20 to 30 N) of the definitive restoration; c) Maintenance of osseointegration during the load period; d) Absence of periimplantitis, or periimplantitis diagnosed and successful treated. In the presence of periimplantitis, the same investigator performed the treatment following the diagnostic and therapeutic guidelines established by Mombelli and Lang20. Mucositis was not included in the criteria for definition of success or failure of the implants analyzed. ResultsThe sample comprised 41 patients with 54 implants. Among these, 17 were placed in the maxilla and 37 in the mandible. Table 1 describes the characteristics of the sample. The mean age was 52.1 years, ranging from 18 to 78 years (Table 1). Table 2 describes the number and distribution of implants placed in posterior maxillary and mandibular regions. It is observed that 39 implants were placed in the region of first and second molars, 11 in sites of second premolars and 4 in regions of first premolars. Table 3 presents the mean height of implant sites assessed by topographic examination, with the minimum and maximum height, related to the mean length of implants placed, as well as to the minimum and maximum length of implants. In the maxilla, the mean length of implants was 1.10 mm greater than the mean bone height of implant sites, i.e. the height of the alveolar ridge was extremely affected, requiring use of the Summers technique in some cases. In the mandible, the mean length of implants was 1.39 mm smaller than the mean bone height available on the implant sites, i.e. the implants were placed very close to the inferior alveolar nerve. The success in the osseointegration period was 96.3%. Two implants were lost from the total 54 implants evaluated (one in the mandible and one in the maxilla). Both losses occurred during the healing period, and no loss occurred during the load period. Failure in the maxilla was detected after 6 months, on reopening. In the preoperative evaluation, the alveolar ridge at this region exhibited bone height of 4.7 mm (evaluated on the tomography) and low bone density, as evaluated during drilling by the surgeon. This site received another implant, which presented successful osseointegration and constitutes one of the short implants in the sample. The other failure occurred in the mandible. This site was submitted to immediate implant placement. Due to the anatomical characteristics, the surgical site was damaged after tooth extraction. The implant had low primary anchorage obtained manually. After 3 months, on reopening, the implant did not present osseointegration. This site received another implant, which had successful osseointegration and is one of the short implants in the sample. Table 4 presents the percentage of success of loaded implants in different periods. There was no loss to followup. However, due to different periods of implantation and prostheses, of the duration of follow-up was not similar for all implants. Fifty-one implants were followed from 7 to 12 months, 43 implants from 13 to 24 months and 35 implants from 25 to 38 months. There was no failure of the 51 implants followed up to 12 months. The implants evaluated in this period presented few complications. Two implants exhibited periimplantitis, which was treated and responded favorably. DiscussionThe present results revealed a high success rate after the use of short implants. Previous studies evaluated the success of short implants and reported favorable outcomes21-24 . However, these studies did not describe the presence of antagonist teeth, and the number of short implants with single-unit restorations was small. One of the limitations of retrospective studies is the possibility of biases, which may impair the validity of the results. In the present study, the outcome analyzed was the implant loss, which reduces the possibility of measurement errors by the examiner. The method for data collection should also be highlighted, which allowed the achievement of results from all patients considered as eligible during the study period. There are studies that reported excellent prognosis with short implants1,25-29. These investigations were conducted on posterior regions rehabilitated with single-unit restorations with follow-up periods of 32 months to 6 years, revealing success rates of 94.5% to 100%. However, even though these studies reported alveolar ridges with reduced height, they did not specifically describe the extent of damage of the alveolar ridges. Concerning the presence and type of antagonist tooth, Fugazzoto et al.27 described the antagonist teeth, which yet were highly variable, including restored or intact natural teeth, fixed dentures, conventional complete dentures, removable partial dentures and implant-supported dentures. All implants in this study received single-unit restorations and were placed in the posterior region. Also, data on the bone height available before implant placement are also presented, evidencing that the alveolar ridge was actually impaired. In the posterior maxillary region, the mean bone height assessed on the tomographic examination was 6.53 mm, ranging from 4.0 to 9.0 mm; many implants were placed using the Summers technique15-17. In the posterior mandibular region, the mean bone height was 9.28 mm, ranging from 7 to 11.2 mm. The mean length of implants was 7.63 mm (7.0-8.5) in the maxilla and 7.89 mm (7.0-8.5) in the mandible. Most implants occluded with restored or intact natural teeth, and only 6 implants occluded with removable acrylic dentures. Considering the present results, it may be concluded that short implants constitute a treatment option for partially edentulous patients with need of single-unit restorations in sites with reduced bone height, with a success of 96.3% in the osseointegration period and 100% in the load period. These results corroborate those of previous studies1,25-27,29. It should be highlighted that all implants in this study presented surface treatment, which enhances the quality of contact between bone and implant, increasing the resistance to removal30 . When planning the placement of implants in posterior regions with reduced bone height, professionals should consider a systematic review31, in which the success of long implants in regions submitted to traumatic maxillary sinus lift ranged from 61.7 to 100% (mean of 91.8%), similar to the success of short implants. Considering these outcomes, it may be stated that the use of short implants in posterior regions may be considered an option, even when the short implant is indicated for single-unit restorations. It may also be assumed that these results are similar to those observed in long implants placed in these surgical sites (posterior maxillary and mandibular region), with success rates ranging from 93 to 98% using implants longer than 10 mm2,8,1011,32. It should be noticed that, in these studies, long implants were placed in regions with adequate bone volume and height that were not submitted to bone augmentation techniques. Comparison of the success of single-unit short and long implants in posterior maxillary and mandibular regions by a randomize clinical trial would not be the most adequate experimental design, since it should include sites that might receive either long or short implants, which would not reproduce the clinical situation with better indication of short implants, i.e. sites with reduced bone height. Conversely, it would be interesting to compare short and long implants with single-unit restorations (in impaired sites submitted to bone augmentation techniques), analyzing the percentage of success obtained in surgeries or bone augmentation associated with the percentage of success of long implants placed in these sites, to allow comparison of both treatment options. Although further research is necessary, the use of short implants should be considered a viable option with good prognosis; besides reducing the cost and time required for the procedures, it also involves a much lower human cost. According to the present clinical and radiographic findings, it may be concluded that short implants with treated surfaces presented adequate success for single-unit restorations in posterior maxillary and mandibular regions in nonsmoking, systemically health patients. AcknowledgementsThe authors wish to thank the radiography center of DIX (Caridade Hospital, Santa Maria, RS, Brazil) for the support related to tomography exams. Dr. Assaf, Montebello References
Copyright 2010 - Braz J Oral Sci The following images related to this document are available:Photo images[os10061t3.jpg] [os10061t1.jpg] [os10061t4.jpg] [os10061t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}