 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 10, No.1 Jan-Mar, 2011, pp. 12-16 In vivo Evaluation of different techniques for establishment of proximal contacts in posterior resin composite restorationsPaula de Carvalho Cardoso1, Alessandra Reis Bastos de Oliveira2, Letícia Vilela Lopes3, Sabrina Caetano Cabral2, Maria Beatriz R. G. Oliveira4 1PhD in Operative Dentistry at Dental School of Federal University of Santa Catarina; Coordinator of the Operative Dentistry graduate program of FUNORTE.GO.Brazil Received for publication: May 30, 2010 Accepted: March 03, 2011 Correspondence to: Paula de Carvalho Cardoso, Rua 3, n. 691 Setor Oeste, CEP: 74115-050, Goiânia, GO, Brazil. Email: paulaccardoso@hotmail.com Code Number: os11003 Abstract Aim: To evaluate the re-establishment of proximal contacts on class II resin composite
restorations by means of 4 different in
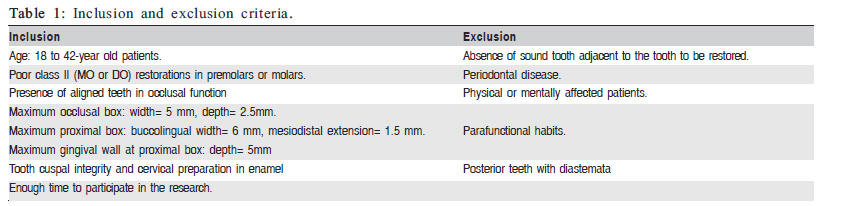
vivo techniques. Keywords: composite resins, definitive restorations, interdental matrix, dentistry. Introduction The evolution of dental materials properties and adhesive systems along with patients' esthetic requirements has increased the use of resin composite restorations for posterior teeth1-5. However, resin composite restorative procedures present some technical difficulties, such as the establishment of proximal contacts6-9. A correct proximal contact enables balanced mesiodistal forces and provides resistance against food impaction at marginal interproximal ridges10-11. One of the limitations of posterior resin composite restorations is the establishment of an effective correct proximal contact12. Some techniques have been proposed for resolution of this problem: the use of pre-polymerized resin composite inserts1,10-11 or ceramic inserts1,13 within restorations, the use of a special instrument for matrix pressuring against the adjacent tooth (Contact +, TDV, São Paulo, SP, Brazil), special polymerization tips (Light- tip)7 and even the development of compactable resin composites14. In addition, preformed matrices and separating rings combined with wedges have produced good results, with adequate contour and form to the restoration15. Proximal contact strengths can be measured using: the Tooth Pressure Meter, analysis of proximal contact strength during dental floss passage and analysis of mesiodistal tooth diameter15-19. Due to the limitations of in vitro studies by the lack of clinical periodontal behavior evaluation, in vivo studies seem more relevant. The aim of this work was to evaluate the re-establishment of proximal contacts on class II resin composite restorations by means of 4 different in vivo techniques. The tested null hypothesis is that there is no difference among resin composite restorative techniques for the establishment of proximal contacts. Material and methods After Ethics Committee approval (Federal University of Goiás, #017/2009), patients were included in this study, receiving all necessary information and signing an informed consent for their participation. Selection of Patients Restorative requirements based on inclusion/exclusion criteria (Table 1) were used for the selection of patients. Cavity preparation Forty class II restorations were prepared in human permanent premolars or molars for this study (MO or DO). Cavity dimensions were accessed with a periodontal probe. Occlusal box isthmus was limited to 3 mm, with 2.5 mm in deepness. Proximal box were limited to 6 mm buccolingual width and 1.5 mm mesiodistal width, with a 5 mm-deep gingival wall (Table 1). One expert operator performed all preparations after an anesthetic shot. A #329 carbide bur (KG Sorensen, Barueri, SP, Brazil) was used at high-speed rotation under constant air-water spray. Internal angles were all rounded. Dental caries were removed with spherical steel burs in low speed. A new bur was used after every 5 preparations. If an old restoration was to be replaced, a cavity preparation was created after its removal. The following clinical standardized protocol was employed:
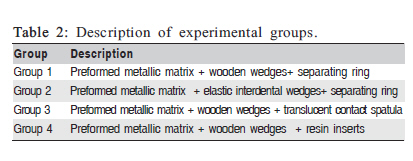
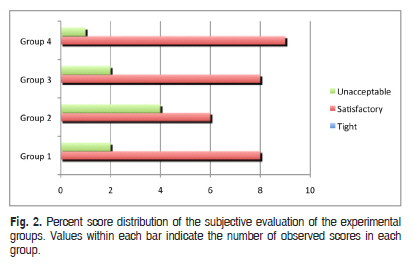
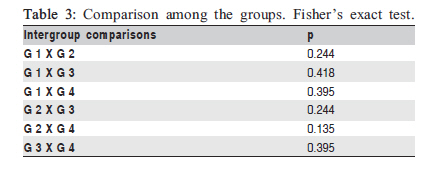
Description of the experimental groups Ten restorations per group were evaluated (N=10, Figure 1 and Table 2). Group 1 (G1) (n=10) performed metallic matrix (Unimatrix, TDV Dental Ltda, Pomerode, SC, Brazil), kept into position with a woodgen edge (Cunhas anatomicas, TDV Dental Ltda, Pomerode, SC, Brazil) combined with a seperating ring (Unimatrix kit, TDV Dental Ltda, Pomerode, SC, Brazil) Group 2 (G2) (n=10): preformed metallic matrix (Unimatrix), kept into position with elastic interdental wedges (Danville Materials Inc., San Ramon, CA, USA) combined with a separating ring (Unimatrix Kit). Group 3 (G3) (n=10): preformed metallic matrix (Unimatrix), kept into position with a wooden edge (Cunhas anatômicas). Before light polymerization of the first resin composite increment, a translucent contact spatula (Contact +, TDV Dental Ltda) was pressed over the matrix, against the adjacent tooth. Group 4 (G4) (n=10): preformed metallic matrix (Unimatrix), kept into position with a wooden edge (Cunhas anatômicas). During the first light polymerization cycle of the resin composite, a resin composite insert (3M ESPE, St. Paul, MN, USA) was inserted within restoration. Restorative procedures Forty cavities were restored according to described techniques. The nanoparticle resin composite Filtek Z350 and the adhesive system Scotchbond Multi-purpose were used (3M ESPE). Restorative procedure for Group 1 A preformed metallic matrix was inserted in the interdental space with the convex surface in contact with the adjacent tooth, kept into position with a wooden edge. For all restorations the wooden wedge was prepared with a #12 surgical blade according to the interdental space. With the exception of restorations that involved the distal surface of superior premolars or mesial surface of inferior first molars, wedge insertion was performed through the lingual side. After acid etching with 37% phosphoric acid (Scotchbond Etchant, 3M ESPE, St. Paul, MN, USA) for 30 s (enamel) and 15 s (dentin), cavities were sprayed with water for 60 s, gently dried with absorbent paper and received 2% chlorhexidine application. Then, the primer was applied, following a gently drying and adhesive application (Scotchbond Multi-purpose), which was light polymerized for 20 s. Light polymerization was performed with Optilux (Demetron Research Corporation, Danbury, CT, USA) at 450 mW/cm2, as checked with an internal radiometer. Three 2-mm-thick resin increments (FilteK Z350) were inserted at the proximal box with metallic spatula (Hu-Friedy mini 4 Goldstein Flexi, Hu-Friedy do Brazil Ltda, Rio de Janeiro, RJ, Brazil), according to the following scheme: first horizontal increment and second plus third ones in an oblique direction. Each increment was light polymerized by 10 s. The occlusal box was restored with 2-mm-thick increments until completion of the occlusal anatomy. After that, an additional light exposure of 40 s was performed in the entire restoration. Restorative procedure for Group 2 The restorative procedure for Group 2 was similar to Group 1, with the exception that a green elastic interdental wedge was inserted after placement of the metallic matrix in the occlusogingival direction. After completion of the restoration, the elastic wedge was removed by cutting it with a scissor and lateral removal in separate portions. Restorative procedure for Group 3 A preformed metallic matrix was inserted in the interdental space with the convex surface in contact with the adjacent tooth, kept into position with a wooden edge. Next, a contact creator translucent spatula (Contact +, TDV, SP Brazil) was pressed against the adjacent tooth during the first layer insertion. After 20 s light polymerization, the spatula was removed and restoration completed. Restorative procedure for Group 4 A preformed metallic matrix was inserted in the interdental space with the convex surface in contact with the adjacent tooth, kept into position with a wooden edge. Next, resin composite insert was pressed against the adjacent tooth during the first layer insertion. The insert was made with Z-350 (3M, ESPE), A2 shade. A resin composite sphere corresponding to 4D 10 of proximal box width was created on a glass slab. A resin composite increment was applied to the proximal box and after that the resin insert was positioned over it and pressed with a metallic spatula against the adjacent tooth until the end of the 20 s polymerization cycle. The spatula was removed after that and restoration completed. Occlusal adjustment was performed with 16- and 30-blade carbide burs following finishing with sandpaper strips (3M ESPE) at the proximal surfaces and abrasive tips at restoration/tooth interfaces (Jiffy Polisher, Ultradent Products). After 30 days, the final polishing was performed with Jiffy Regular Brushes (Ultradent Products). Subjective evaluation of proximal contact re-establishment Six metallic inlays were made on dental models (P-Oclusal Produtos Odontológicos Ltda, São Paulo, SP, Brazil) representing one of the following types of proximal contacts: tight (T) for heavy contacts; satisfactory (S) for acceptable ones; and unacceptable (U) for the absence of proximal contact16. The subjective evaluation or restored proximal surfaces was performed by two previously calibrated examiners, through a direct comparison with standard patterns defined on metallic inlays. After calibration, evaluation was accomplished by passing a dental floss (Expasion Plus Johnson & Johnson, SP, Brazil) between each restored tooth and the adjacent one, following the same direction during insertion and removal. The classification was guided by the previously adopted criteria for metallic inlays at tooth models [tight (T); satisfactory (S) and unacceptable (U)]. A consensual decision was done in cases where doubts impaired a direct conclusion. All evaluations were performed immediately after restoration (L0) and 30 days after it (L1). Before each clinical evaluation, teeth were cleaned with water spray, dried with air and visually examined with the aid of a #5 clinical probe explorer. Additionally, an interproximal radiographic examination was performed before and after the restorative procedure. Fisher's exact test was used to verify differences among the techniques for establishment of proximal contacts in posterior resin composite restorations. Statistical significant differences were computed with pd"0.05. Results Figure 2 shows that the performance of the four groups was statistically similar. Table 3 shows paired comparisons for the groups (Fisher's exact test at p > 0.05). At the second evaluation (L1), results were similar to the first evaluation Discussion Direct resin composite restorations in posterior teeth represent a clinical challenge due to the difficult in establishing an effective proximal contact, which is an important parameter for periodontal health, mesiodistal stability, absence of food impaction and patient comfort20-21 However, few studies have investigated the influence of different restorative techniques on the re-establishment of adequate proximal contacts. Several techniques have been proposed to enable better proximal contacts, e.g., special contact creation instruments22, use of resin or ceramic inserts23, and use of different resin viscosities19,24-25. In vivo study seems more meaningful, being used in the present study for the clinical evaluation of the proximal contact re-establishment with four restorative techniques using matrices and wedges, eventually analyzing the difficulties and facilities of each technique. Two evaluations were performed in the present study: immediate after restoration (Lo) and 30 days after restoration (L1). The reason for the 2 evaluations is related to the period necessary for periodontal accommodation since during restorative procedures teeth are subjected to lateral forces at placement of wedge, claps and matrices26. According to Loomans et al. 2006, the restoration of class II cavities tend to alter the original proximal contact due to tooth extractions, mesiodistal tooth movements under forces produced by progressive eruption of third molars, or unbalanced occlusal forces. However, they did not found any alteration during 18-month follow up in patients with restored class II cavities16. Results from Figure 2 and Table 3 show that the null hypothesis was accepted since no differences were found among all clinical techniques. Although group 4 showed a larger number of acceptable contacts there was no statistically significant difference in relation to the other groups. No tight proximal contact was observed in any restoration of all groups. It was not found any scientific explanation for this observation. In face of the obtained results, the use of elastic wedges and special contact creator instruments seems questionable since dentists would spent more money on new devices and practicing lessons, with no significant benefits. According to the employed methodology, it is possible to conclude that there was no difference among techniques for proximal contact reconstruction with composite resin. References
The following images related to this document are available:Photo images[os11003t3.jpg] [os11003f1.jpg] [os11003f2.jpg] [os11003t2.jpg] [os11003t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}