 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 10, No.1, Jan-Mar, 2011, pp. 37-41 Comparison of root canals obturated with ProTaper gutta-percha master point using the active lateral condensation and the single-cone techniques: a bacterial leakage study Anizabele Milet do Amaral Mercês1, Carlos Menezes Aguiar2, Neide Kazue Sakugawa Shinohara3,Andréa Cruz Câmara4, Jose Antonio Poli de Figueiredo5
1Private Practice, Recife, Brazil
Received for publication: August 26, 2010 Correspondence to: Carlos Menezes Aguiar Rua Aristides Muniz, 70/501, Boa Viagem, Recife PE 51020-150 Brazil. Phone: (+55) 81 3467 6821. E-mail: cmaguiar.ufpe@yahoo.com.br Code Number: os11008 AbstractAim: The aim of the present study was to assess the recontamination time of root canals filled
with ProTaper gutta-percha master point using the active lateral condensation and the
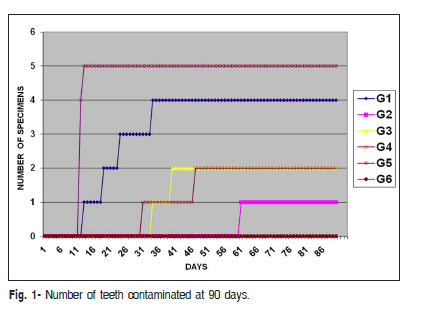
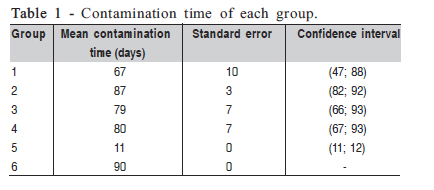
single-cone techniques. Keywords: gutta-percha, microleakage, ProTaper gutta-percha master point, ProTaper Universal, single-cone technique. Introduction Successful root canal treatment requires proper cleaning and shaping of root canal, as well as hermetic sealing of root canal space with an inert, dimensionally stable, and biologically compatible material1. When the coronal portion of the root canal is exposed to the oral environment, the root canal is a potential route for microorganisms to gain access to the periapical tissue. This situation may lead to endodontic failure2. From a clinical standpoint, coronal exposure of the root canal obturation might be considered an indication for endodontic retreatment3. The influence of the quality of the coronal restoration is an important factor in achieving success in root canal treatment. The teeth with a satisfactory coronal restoration displayed significantly better periapical healing than those with an unsatisfactory restoration4-5. Radiographically, the technical quality of endodontic treatment is significantly more important than the technical quality of the coronal restoration when the periapical status of ally treated teeth is evaluated6. The biomechanical preparation with nickel-titanium (NiTi) rotary system was considerably quicker than the hand instrument series7. It would appear that rotary NiTi instruments have the potential to prepare root canals more efficiently, and to shape root canals with greater safety8, achieving a three-dimensional obturation of the root canal over its whole length without the time spent on lateral condensation9. Cleaned and shaped root canals must be filled three-dimensionally, eliminating the empty space, which has the potential to be infected or reinfected10. The aims of the root canal sealer are to prevent penetration of bacteria and eliminate the risks of infection or reinfection of the root canal system3. Given the importance of the root canal filling and the control and prevention of endodontic infection, several studies have been published on the subject10-12. Coronal leakage has been evaluated by different tests, among which is the analysis of bacterial penetration through the filling material. This method has been used because it has reached results similar to those obtained in daily practice13. The purpose of this study was to investigate the time required for recontamination of root canals sealed with ProTaper gutta-percha cones after obturation with two different techniques and exposure to a simulated oral environment. Material and methods Specimen Selection and Preparation and Root Canal Filling Fifty intact, caries-free, human mandibular premolars with single roots and mature apices (mean length of 21 mm) were used. The teeth were obtained from the Tooth Bank of the Department of Prosthodontics and Oral and Maxillofacial Surgery of the Federal University of Pernambuco, after approval of the Research Ethics Committee of the University's Center of Health Sciences. Buccolingual and mesiodistal were radiographs were taken to confirm the presence of a single canal. Once coronal access had been established, a K-File #10 (Dentsply/Maillefer, Ballaigues, Switzerland) was inserted into the root canal until the tip was just visible beyond the apex. The working length (WL) was determined at 1 mm short of this length. The root canals were prepared by the ProTaper Universal™ rotary system (Dentsply/Maillefer, Ballaigues, Switzerland). In groups 1 and 2, the root canals were instrumented up to instrument F4, and in the groups 3 and 4 the canals were prepared up to instrument F5. A single operator instrumented all root canals. The root canals were irrigated with a freshly prepared 1% sodium hypochlorite solution (Roval, Recife, Brazil) in conjunction with ethylenediaminetetraacetic acid (Biodinâmica, Paraná, Brazil) as a chelating agent for irrigating the root canals, as well as the 3-mL FCF syringe system (FCF, Sao Paulo, Brazil) with a 30-gauge needle (Injecta, Diadema, Brazil). The irrigation was performed at the beginning of the instrumentation, between the changes of instrument, and at the end of the biomechanical preparation. The specimens were stored in glass test tubes and were individually sterilized in an autoclave at 121°C for 30 minutes. Ten samples were randomly chosen and immersed totally in bottles containing 10 mL autoclaved brain heart infusion (BHI; Acumedia, Lansing,MI). They were kept in an incubator at 37°C for 96 hours to check the sterilization's efficacy. After preparation, the specimens were randomly divided into six groups as follows: - Group 1: 10 specimens were filled using the single cone technique with the gutta-percha master point F4 (Dentsply/Maillefer, Ballaigues, Switzerland) and AH Plus sealer (Dentsply DeTrey, Konstanz, Germany). - Group 2: 10 specimens were filled using the active lateral condensation technique with the gutta-percha master point F4 and 10 FF accessory cones (Dentsply/Maillefer, Ballaigues, Switzerland) and AH Plus sealer . - Group 3: consisted of 10 specimens filled using the single cone technique with the gutta-percha master point F5 and AH Plus sealer. - Group 4: 10 specimens were filled using the active lateral condensation technique with the gutta-percha master point F5 and 10 FF accessory cones and AH Plus sealer. - Group 5 (positive control group): consisted of 5 specimens that did not have the canal filled. - Group 6 (negative control group): consisted of 5 specimens that did not have the canal filled but was rendered impermeable by receiving an epoxy resin coating (Araldite,Brascola, São Bernardo do Campo, Brazil) along its entire length. Three blinded endodontists evaluated the root fillings on radiographs in accordance with the criteria of Eckerbom and Magnusson14. Leakage Apparatus Preparation The apparatus used to evaluated saliva leakage was prepared as previously described by Gomes et al.11, with modifications. Glass vials with rubber stoppers were adjusted for use in this experiment. Using a heated instrument, a hole was made through the center of every rubber stopper in which each tooth was inserted under pressure up to its cementoenamel junction, so that its crown lay outside and its root inside the vial. The teeth were sealed with three layers: a layer of cyanoacrylate (Henkel Ltda, São Paulo, Brazil), a layer of epoxy resin (Pulvitec S.A. Indústria e Comércio, São Paulo, Brazil) and a final layer of cyanoacrylate were applied at the interface between the tooth and rubber. Thereafter the roots were sealed with two layers of cyanoacrylate, except for the apical 2 mm around the apical foramen. The cylinders prepared from 5-mL plastic syringes (Plascap, São Paulo, Brazil) were adapted on the external surface of the stoppers to create a chamber around the crown of the tooth. The junction between the plastic cylinders and glass tube was sealed as described above. The apparatus was then sterilized with ethylene oxide gas (Galdi Produtos Hospitalares, Paulista Brazil) for 12 h. The chamber of each apparatus was filled with BHI, so that approximately 2 mm of the root apex was immersed in the broth. To ensure sterilization, no growth was observed after the whole apparatus was incubated at 37ºC±1 for four days. Any test apparatus that showed signs of turbidity in the BHI broth was discarded. Bacterial Leakage Test The bacterial stains used for analysis were Pseudomonas aeruginosa (American Type Culture Collection ATCC 9027), Enterococcus faecalis (ATCC 19433), Escherichia coli (ATCC 8739) and Staphylococcus aureus (ATCC 6538). The microorganisms used in this study were selected because of their clinical importance and association with the endodontic infection10,15. The chamber of each apparatus was filled with 3 mL of sterile artificial human saliva (Farmácia Roval de Manipulações, Recife, Brazil) and mixed in BHI broth in a 3:1 (v/v) ratio. The saliva was replenished every 3 days for 3 months. The turbidity of the inocula was adjusted to approximately 108 UFC/mL, this concentration being obtained using the Neubauer Chamber technique16. The apparatus was incubated at 35°C ± 1 and checked daily for the appearance of turbidity in the BHI broth over a period of 90 days. The number of days it took for bacterial growth to appear was indicative of the total recontamination of the root canal by bacteria from the saliva. Following the appearance of broth turbidity, aliquots were removed and sowed in BHI, Agar blood, Agar Levine, Agar MacConkey and Agar Chapman, and the plates were incubated in a cabinet at 35oC ± 1 for 24 hours. The bacterial identification was based on colony features, Gram-staining and cell morphology: catalase production test, Triple Sugar Iron Agar test (TSI), growth in 6.5% NaCl BHI broth, Esculin Bile Agar, and Hugh-Leifson's test, constituting the complementary identification tests17. Statistical Analysis The statistical analysis was performed using the KaplanMeier test for survival analysis, which includes calculation of the median time leakage and pairwise comparisons of groups. The Long-Rank test was used to compare the survival curves of the groups. A level of significance of .05 was adopted. Results All specimens in the positive control group showed broth turbidity within 13 days of incubation. By contrast, none of the negative control specimens leaked during the experimental period (90 days), confirming the efficacy of rendering the whole root surface waterproof (Figure 1). Four specimens in group 1 showed contamination at 36 days. The first specimen that showed microbial leakage was observed at 13 days. In group 2, 1 sample showed contamination at 61 days. Two specimens in group 3 showed contamination at 41 days. The first specimen that showed microbial leakage was observed at 34 days. In group 4, 2 samples showed contamination at 46 days. The first specimen that showed microbial leakage was observed at 34 days. There was no significant statistical difference among the tested techniques. The results of the Kaplan-Meier test are shown in Table 1. The Long-Rank test revealed no statistically significant differences between the root canal filled techniques and the diameters of the gutta-percha master points employed. Discussion Methods to measure microleakage have included the use of dyes18, human saliva19, microorganisms20 and bacterial toxins21. The inadequacies of each of these methods have been highlighted and their clinical significance questioned. Although the use of dyes, radioisotopes, fluid filtration, bacteria, and endotoxins penetration techniques to evaluate sealing capacity of endodontic materials, the bacteria leakage model has proved to be the most clinically important one12,22. Facultative anaerobic and aerobic microorganisms have been used, although they are found in only 10 to 20% of root canals with a chronic periapical reaction. Such microorganisms are found interacting with strict anaerobes, causing changes in nutritional relationships, shifts in redox potential and oxygen tension, thereby establishing the microbial survival relationship23. Determining the sealing capacity of endodontic materials against these microorganisms is essential. The endodontic sealers showed degradation with oral fluids. AH Plus showed the smallest weight loss in water and artificial saliva with different pH values24. This is because AH Plus is an epoxy resin-based sealer, and provides a tight seal of the root canal system1. These properties justified its choice and use in this study, corroborating the findings of Tronstad et al.6. Complete obturation of the root canal system is an important factor in achieving success in root canal therapy. Ideally, root canal filling should be a complete, homogenous mass that fills the prepared root canal completely. The conventional root-filling technique taught in most dental schools25 and used by dentists26 has been the cold lateral compaction technique using the .02 tapered gutta-percha point as the master cone, supplemented with accessory cones. However, several practitioners regard it as time-consuming and difficult to master. The alternative to root canal filling is the single-cone technique9. This tendency to optimize endodontic treatment led to the evaluation of the sealing capacity of these techniques, using the ProTaper gutta-percha master points. The teeth obturated using the vertical compaction technique exhibited a dense fill throughout the canal space with the aim of preventing the leakage of microorganisms20. The results of the present study showed no statistically significant differences between the methods employed. Although the cold lateral compaction of gutta-percha has been regarded as the gold-standard obturation technique, the results of the research were in agreement with those of Britto et al.27, which showed microleakage of microorganisms. Yücel et al.3 demonstrated that all samples obturated with cold lateral compaction showed bacterial penetration after 60 days of observation. Their results are at odds with those observed in the present study, in which 15% of the specimens showed bacterial leakage after 60 days. The reason for the discrepancies between the two studies was determined by enlarging the apices. At 90 days, bacterial penetration was observed in 22.5% of all the specimens, in contrast with the results of Ricucci and Bergenholtz28, who demonstrated that well-prepared filled root canals resist bacterial penetration even after long-standing oral exposure to caries, fracture or loss of restoration. Although West29 stated that apical enlargement with #40 or #50 files ensures maximum cleaning of the foraminal constriction and increases apical sealing, the results of the present study showed no significant differences between apical enlargement and apical seal. The present study demonstrated that there is no filling material or root canal filling technique able to completely prevent the entry of microorganisms into the root Comparison of root canals obturated with ProTaper gutta-percha master point using the active lateral condensation and the single-cone techniques: abacterial leakage study canal space when the teeth are in an oral environment. These results are in agreement with the findings of Timpawat et al.1, Britto et al.27, Yücel et al.3, and Monticelli et al.22. This study showed that an increased apical diameter did not hinder bacterial penetration, neither did it minimize root canal recontamination time. The cold lateral compaction and single-cone technique appears to be effective in prevent the leakage of microorganisms. It may be concluded that there was no difference in bacterial penetration between the root canal filling techniques. The mean root canal contamination time was 67 days. Acknowledgements This study was supported by grants from Conselho Nacional de Desenvolvimento Científico e Tecnológico-CNPq-Brazil. The authors wish to express their special thanks to Professor José Luiz de Lima Filho and Professor Maria Elizabeth Cavalcante Chaves, from LIKA (Laboratório de Imunopatologia Keizo Asami) for their valuable technical support. References
The following images related to this document are available:Photo images[os11008f1.jpg] [os11008t1.jpg] |
| |||||||||

{kind=link}
{kind=link}