 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 10, No.1, Jan-Mar, 2011, pp. 55-59 Effect of the smear layer on the filling of artificial lateral canals and microleakage Andréa Gonçalves Moretti1, Carlos Augusto de Morais Souto Pantoja2, Danna Mota Moreira2, Alexandre Augusto Zaia3, José Flávio Affonso de Almeida3 1Undergraduate Student, Department of Restorative Dentistry, Endodontics Division, Piracicaba Dental School, University of Campinas, SP, Brazil Received for publication: November 10, 2010 Correspondence to: José Flávio Affonso de Almeida Department of Restorative Dentistry, Endodontics Division, Piracicaba Dental School, University of Campinas. Av. Limeira, 901, 13.414-903 Piracicaba,SP, Brazil. Phone: +55 19 2106 5344 Fax: +55 19 2106 5218 E-mail: jfalmeida@fop.unicamp.br Code Number: os11011 AbstractAim: To evaluate the influence of the smear layer on the filling and prevention of microleakage
in artificial lateral canals after use of different irrigating solutions.
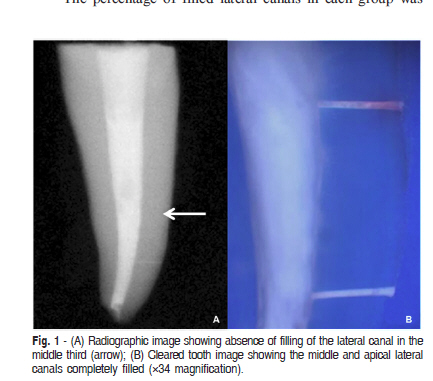
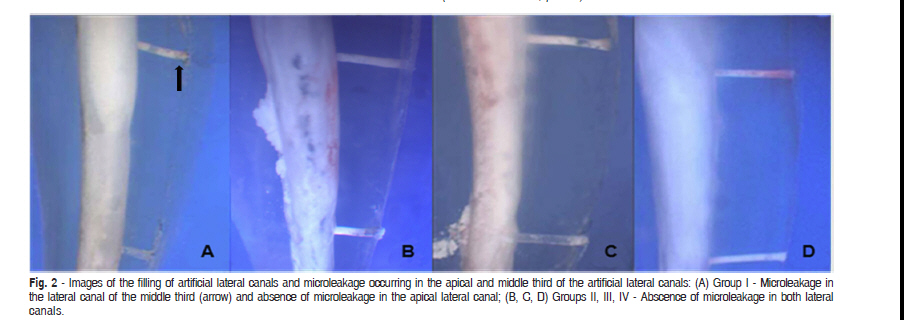
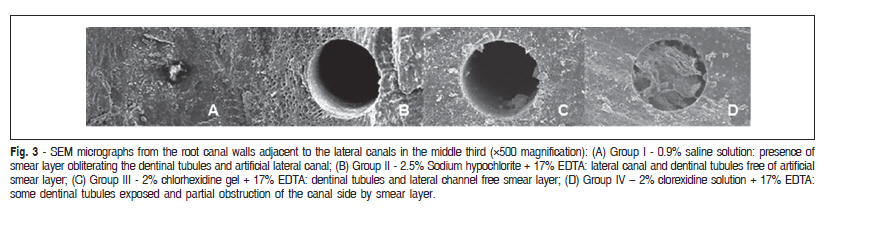
Keywords: endodontics, root canal obturation, smear layer. Introduction The smear layer consisting of dentin shavings, cell debris and pulp remnants1-5, includes two separate strata: a loose superficial deposit and an attached stratum that extends into the dentinal tubules and forms occluding plugs6. Several studies have shown the effect of smear layer on the filling and adhesive procedures7-9. The removal of the smear layer promotes an increase in dentin permeability, thereby allowing greater penetration of filling materials inside the root canal system10-12. Considering that lateral canals have small diameters, equal to or higher than 0.1 mm ranging from of 43.6%13 to 69.3%14, the removal of smear layer could enrich the filling of these structures. The use of different irrigating regimens during endodontic treatment can improve both antimicrobial activity and the removal of the smear layer from the dentin walls. According to Goldberg et al.15 (1986), removal of the smear layer using 15% EDTA can improve the filling of lateral canals, when compared to the use of 5% NaOCl and distilled water. However, Villegas et al.16 (2002) evaluated the filling of accessory canals using cleared teeth and the warm obturation technique. Different irrigating solutions were used and the authors observed no differences between 6% NaOCl alone or in association with 15% EDTA. This result was similar to that of Bertacci et al.17 (2007) who found no influence of EDTA on the filling of lateral canals. Although a warm gutta-percha filling can cross over the smear layer, there is still no consensus on whether the smear layer can affect lateral condensation, one of the most commonly used filling techniques18-19, or AH Plus in the filling and prevention of microleakage in lateral canals. Thus, the aim of this study was to evaluate the ability of lateral condensation and AH Plus to fill and prevent microleakage in the presence or absence of the smear layer in artificial lateral canals. Material and methods Fifty-two recently extracted human maxillary anterior teeth were selected after the approval of the Human Research Ethics Committee of the Piracicaba Dental School, University of Campinas, Brazil. The crowns were removed using a low-speed diamond disc under running water and a standard length of 15 mm was achieved for each root. Digital buccolingual radiographs (Digora, Orin Corp., Soredex, Helsinki, Finland) was obtained and teeth with resorption, fracture or incompletely formed apices were excluded from the study. The artificial lateral canals were prepared, one in the middle and the other in the apical third, perpendicular to the longitudinal axis of the teeth using 0.10 mm cylindrical drills (Unio Tool Europe S.S., Marin, Neuchâtel, Switzerland) according to Almeida et al.20. The penetration of the drill into the root canal was checked by introducing a size 06 K-file (Dentsply Maillefer, Ballaigues, Switzerland) into the perforations and another digital radiograph was exposed. If the file did not penetrate into the main root canal, the tooth was discarded. Initially, the teeth were instrumented with Largo drills #3-2 and Gates Glidden drills #5-2 (Maillefer, Ballaigues, Switzerland). The working length was established 1 mm short of the apex. All teeth were instrumented at the working length to a #40 file and the apical patency was checked with of a # 25 file. The irrigation protocols were carried out as follows (n=10): Group I - Irrigation with 3 mL of 0.9% saline solution after the use of each instrument. Group II The root canal was filled with 3 mL of 2.5% sodium hypochlorite (NaOCl), instrumented, and finally irrigated with 3 mL of saline after each instrument. The root was refilled with NaOCl. Finally, 3 mL of 17% EDTA was used to remove the smear layer for 3 min, and 3 mL of 0.9% saline solution were used as the final irrigant. Group III - The canals were filled with 2% chlorhexidine gel (CLX gel), instrumented and finally irrigated with 3 mL of 0.9% saline solution after the use of each instrument. Then, 3 mL of 17% EDTA was used to remove the smear layer for 3 min, and 3 mL of 0.9% saline solution were used as the final irrigant. Group IV - As in Group III, but using 2% chlorhexidine solution (CLX sol) instead of 2% chlorhexidine gel (CLX gel). Before root canal filling, the teeth were mounted in alginate blocks (Dentsply, Petrópolis, RJ, Brazil) to confine the sealer after it had flowed through the artificial lateral canals, in an attempt to simulate the periodontal ligament according to Almeida et al.20. The root canals were dried using paper points (Tanari, Manacapuru, AM, Brazil) and were obturated by lateral condensation of the gutta-percha and AH Plus sealer mixed according to the manufacturer's instructions and placed in the canal roots with a size 40 spiral Lentulo (Maillefer). A standardized gutta-percha cone #40 (Tanari) was fitted as the master cone. Lateral condensation was performed using a size 30 endodontic finger spread (Dyna, Bourges, France) and B7 and B8 accessory gutta-percha cones (Tanari). Following obturation, the excess gutta-percha was removed with a heated instrument (3 mm inside the canal), and cold pluggers (Duflex-S.S. White; Rio de Janeiro, RJ, Brazil) were used to vertically condense the coronal gutta-percha. The coronal access was filled with temporary cement (Coltosol; Vigodent SA, Rio de Janeiro, RJ, Brazil). The filled teeth were stored at 100% humidity at 37 °C for 48 h to allow the sealers to set. The digital radiographs were taken and the images were assessed using the Image Manager Program (IM50; Leica Microsystems, Wetzlar, Germany). The total length of the lateral canal and its filling was measured and the values obtained were converted to the percentage of canal filled. The external root surface was sealed with two layers of red nail varnish, except for the area over the lateral canals. Four unfilled teeth were used as positive and negative microleakage controls. The positive control was sealed like the other teeth and the negative control was sealed completely including the lateral canal orifices. Images of two additional teeth for each group were taken in a scanning electronic microscope (JEOL; Model JSM 5600 LV, Tokyo, Japan) to examine the cleanness of the root canal walls in the middle and apical third illustratively. The roots were then immersed in Indian ink (Royal Talens, Apeldoorn, The Netherlands), submitted to vacuum for 30 min and stored in the ink for 24 h. Following exposure to the dye, the roots were rinsed in tap water and the nail varnish was removed completely. The teeth were decalcified in 5% hydrochloric acid for 72 h and cleared in methyl salycilate according to the protocol reported by Zaia et al.21. The extent of filling, dye penetration and the total length of the lateral canals were measured on the buccal and lingual root surfaces, under a magnifying microscope (×34) (Leica Microsystems, Wetzlar, Germany). The obturation of the lateral canals was measured linearly, using a scale in millimeters. The values obtained were divided by the total length of the lateral canal and multiplied by 100 to obtain the percentage of obturation after the use of each irrigant solution. Similarly, the leakage of dye between the sealer and the wall of the lateral canal was measured and the values were divided by the amount of sealer in the lateral canal. The Kruskal-Wallis test was used to compare the values of dye microleakage obtained in the middle and apical third of the root canal with different irrigating solutions. ANOVA and post hoc Tukey's test was used to evaluate the values of filling obtained between experimental groups considering the same third. The Wilcoxon test was used to compare the values obtained from the different thirds of the root canal after the use of each irrigation protocol. Results The radiographic analysis failed to identify filled lateral canals in 20% of specimens, although these were visible using the clearing technique (Figure 1). Thus, the parameters for establishing the filling results were based on the clearing technique and dye microleakage, when partially filled or unfilled lateral canals were shown by x-rays. The percentage of filled lateral canals in each group was statistically similar, regardless of the location of the lateral canals or the presence/absence of the smear layer (Figure 2, Table 1). SEM micrographs revealed smear layer along almost all root canal walls and covering the artificial lateral canal openings in group I (saline solution without EDTA). The other groups (with EDTA) presented root canal walls almost clean and artificial lateral canals partially or totally opened (Figure 3). The linear analysis of microleakage between the sealer and dentinal walls revealed variability among the groups of auxiliary chemical substances and the presence/absence of the smear layer (Figure 2). However, no statistically significant differences were found (p = 0.1283 Kruskal-Wallis test - Table 2). Discussion Although some studies have shown that lateral condensation results in less filling of lateral canals when compared with the thermoplasticized gutta-percha22-23, others have shown no significant differences between the two techniques24-25, or that lateral condensation is able to efficiently fill the natural root ramifications15,20,26. Analysis of the specimens via digital radiography, clearing and dye leakage showed no significant differences in the filling of artificial lateral canals in the presence or absence of the smear layer, regardless of the location of the lateral canals. According to Villegas et al.16 (2002) irrigation with 2.5% sodium hypochlorite alone or combined with EDTA gives better sealing of natural accessory canals compared with instrumentation without irrigation or with irrigation with distilled water. These results are attributed to the fact that EDTA in combination with other irrigating solutions removes inorganic tissues during irrigation, resulting in better penetration of the filling material15-16. The ability to remove the smear layer presented by sodium hypochlorite alone or associated with EDTA can be observed with the use of 2% chlorhexidine gluconate gel. This auxiliary chemical substance is able to eliminate anaerobic microorganisms and decrease the formation of smear layer in the root canals walls27. The divergence of the results of this study from those described above can be explained by the fact that the smear layer formed during instrumentation, especially in Group I, was not able to totally obliterate the previously empty artificial lateral canals, or even to prevent the compression of filling materials. It should be emphasized that the smear layer is not an organized structure28 and does not offer any resistance when the filling material is compressed into the natural ramifications, which are much larger than the dentinal tubules. Kasahara et al.29 (1990) showed that about 90% of ramifications present on 510 maxillary central incisors had thick less or equal than 150 µm. In this study, the diameter of artificial lateral canals was 100 µm. Bertacci et al.17 (2007) reported that the thickness of the endodontic smear layer is probably 1-5 µm and can easily be pushed with enough pressure by warm gutta-percha inserted inside the root canal. Like warm gutta-percha, lateral condensation and AH Plus could cross over the smear layer into artificial lateral canals. Although group IV presented higher rates of dye penetration, the results of this study showed no significant differences after the use of different irrigation protocols. Similarly, after the use of different irrigants such as saline solution, 5.25% sodium hypochlorite and 0.12% chlorhexidine digluconate to prepare the root canal, there was no difference in microleakage in the apical region of the root canal30. However, removal of the smear layer using 5.25% NaOCl associated with 17% EDTA had a positive effect on reducing apical and coronal leakage5. It is likely that in artificial lateral canals the thickness of the smear layer is not sufficient to obstruct the penetration and reduce the sealing ability of filling materials. The physical and chemical properties of sealers or the root filling techniques may be more important for filling and preventing microleakage than the presence of smear layer in artificial lateral canals. According to Wu et al.31 (1994) some endodontic sealers with a thinner film thickness, between 0.25 to 0.05 mm, can seal tightly the root canal filling. In this study, the AH Plus sealer and the diameter of ramifications were able to prevent microleakage. Twenty-nine natural ramifications were found in 13 teeth, comprising lateral, secondary and accessory canals. Almeida et al.20 (2007) used lateral condensation, as in this study, and found 18 ramifications in 13 teeth. Other studies showed a total of 100 filled lateral canals in 84 teeth32, 130 filled lateral canals in 40 teeth17 and 318 filled ramifications in 64 teeth33. These divergent results are probably due to the group of teeth analyzed or the filling technique used in each study. In conclusion, the presence or absence of the smear layer did not affect the ability of lateral condensation and AH Plus to fill and prevent microleakage in artificial lateral canals. The radiograph images were not able to demonstrate artificial lateral canal filling in approximately 20% of cases, but their filling was confirmed using the clearing technique. References
The following images related to this document are available:Photo images[os11011t1.jpg] [os11011t3.jpg] [os11011t4.jpg] [os11011f1.jpg] [os11011f3.jpg] [os11011f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}