 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 10, No. 1, Jan-Mar, 2011, pp. 65-68 Dental arch morphology in normal occlusions Luiz Renato Paranhos1, Will A. Andrews2, Renata Pilli Jóias3, Fausto Bérzin4, Eduardo Daruge Júnior4, Tarcila Triviño5 1 DDS, MS, PhD, Full Professor, Department of Orthodontics, School of Dentistry, Methodist University, Brazil Received for publication: November 14, 2010
Correspondence to: Luiz Renato Paranhos Rua Padre Roque, 958 Centro / Mogi Mirim São Paulo Brasil 13800-033. Phone: 55 19 3804-4002 E-mail: paranhos@ortodontista.com.br Code Number: os11013 Abstract Aim: The aim of this study was to identify the prevalence of 3 different mandibular dental
arch morphologies in individuals with natural normal occlusion.
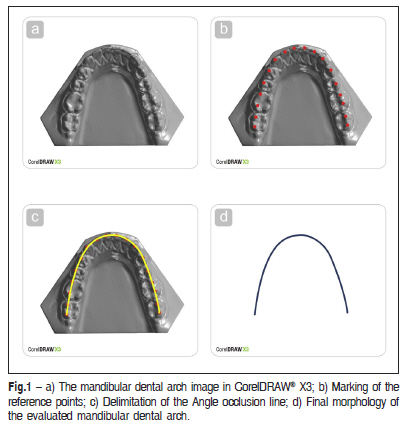
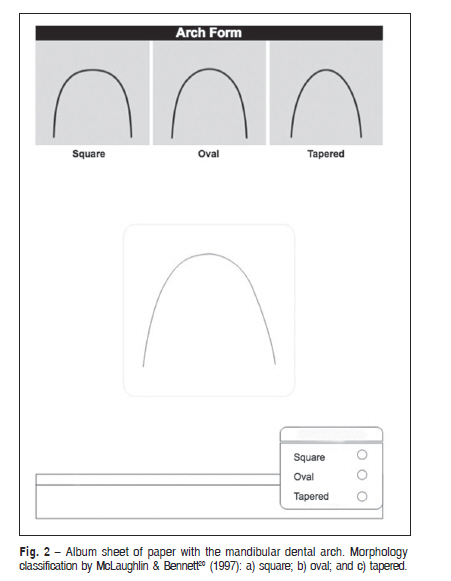
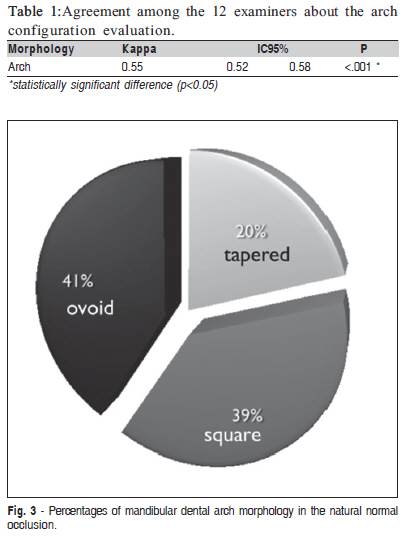
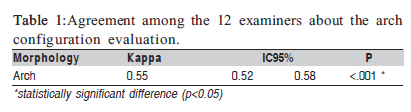
Keywords: normal occlusion, dental arch morphology, mandibular dental arch, anatomy. Introduction Dental arch morphology is an important consideration in orthodontic treatment of dentofacial deformities. For over one century dental arch morphology has been studied in hopes of defining proper goals for tooth position, esthetics, function and long-term stability1-4. Because the mandibular dental arch is one of the main references for orthodontic treatment planning, many studies have strived to define its ideal size and morphology5-8. According to the literature9, human dental arch morphology shows wide individual variation. Descriptions range from elipsoid6, parabolic6,10, a segment of circle joined to lines10, a segment of circle11 caternary curve, etc… Diagrams were subsequently designed to aid orthodontists in forming wires to shape the dental arches during the treatment12-13. The use of standardized diagrams has been contested by some authors6,14-16, who suggested instead to use mathematical formulas17 to find a more individualized shape for arches. The aim of this study was to verify the prevalence of three different morphologies of the mandibular dental arch in natural normal occlusions and then correlate those findings to other variables that may help guiding Material and methods This study was approved by the Research Ethics Committee of the School of Dentistry of Piracicaba, University of Campinas (Protocol # 149/2008). Sample The study sample consisted of 51 mandibular dental casts from Caucasian individuals with natural normal occlusion. The ages ranged from 15y2m to 19y4m, with a mean age of 16y6m. There were 21 (41.2%) males and 30 (58.8%) females in the sample. Individuals with craniofacial and/or dental anomalies or asymmetries were excluded. All subjects had no previous preventive and/or corrective orthodontic treatment. Each cast presented at least four of the six keys to normal occlusion described by Andrews18. The first key (molar Class I of Angle10) bilaterally was required on all casts. All the permanent teeth were in occlusion, except the third molars. Plaster model digitizing The mandibular dental casts were individually digitized on a scanner dw5-140 (Dental Wings®; Montreal, Quebec, Canada), previously calibrated as instructed by the manufacturer. The image acquisition was processed by points (accuracy: 20-50 microns), according to the cast Cartesian axes. The images were automatically generated by a software program (Dental Wings®), generating a volumetric archive (.stl) for each cast. Attainment of the images After digitizing the casts the computer "Print Screen" resource was used to convert the images into figures. These figures had been transferred to the vectorial software CorelDRAW® X3 software, in which they had been cropped and prepared for evaluation. The control points in each mandibular cast were: the incisal edges of the incisors, the canine cusp tips, and the premolar and molar buccal cusp tips. When connected, these points formed Andrews' "perimeter line"19, which assisted in the determination and evaluation of the dental arch morphology (Figure 1). Subjective determination of the morphology of the mandibular dental arch The dental arch 3D images were printed on white paper (90 g/m2). Each image was individually arranged in the center of a sheet of paper, below a guide, with three different dental arch configurations: square, oval and tapered20 (Figure 2). An album containing the 51 images, with one image on each sheet of paper, was distributed to each appraiser. The examiners (5 male and 7 female) were dentists with at least a master's degree in orthodontics. Each examiner was instructed to subjectively pick one, and only one, match for the shape of the arch relative to the 3 given categories. Statistical analysis To test the level of agreement of the dental arch subjective classification among the examiners, the modified Kappa statistical test21-22, at 5% significance level was used. The Kappa values range from -1 to +1. +1 establishes a perfect agreement. After a 15-day interval, the examiners reclassified all the images to evaluate the reliability of the measurement method and the operator's calibration. The systematic error was calculated by the paired Student's t test, at a significance level of 5%. Dahlberg's method was used to calculate the casual error23. The inter-examiner level of agreement was tested by the modified Kappa statistical test21-22 at a significance level of 5%. To evaluate the measurement method reliability and the operator's calibration, all the images were reclassified by all examiners after a 15-day interval. The systematic error was calculated by the paired Student's t test, at a significance level of 5%, and to calculate the casual error, it was used the Dahlberg's method23. Results It was not verified any systematic or casual error (p<0.05), showing the reliability of the used methods. The Kappa results showed statistically significant agreement for the arch configuration between the examiners (Table 1). According to Landis and Koch21 the agreement value (0.55) was "moderate". The percentages of mandibular dental arches morphology in this sample of natural normal occlusions are shown in Figure 3. (Table 1) Discussion The purpose of orthodontic treatment is to correct, intercept and/or prevent incorrect dental positions and dentofacial deformities, so that teeth and bone structures can be in harmony. The changes achieved during treatment should not disrupt the balance between teeth, bone structures and muscles. Early orthodontic philosophies advocated expansion of the dental arches, without consideration to the balance among other stomatognathic structures. Later philosophies discovered that dental expansion over a certain limit could be unstable1-2. However, some dental arch expansion or contraction might be stable in growing patients if the tooth positions did not significantly modify physiological muscles function1,3,5. Since mature patient's teeth tend to return to their original positions because orthopedics is not possible to be applied, the transverse dental movement should be as minimal as possible during the orthodontic therapy. Orthodontic movement will be more stabile if there is a satisfactory balance between the muscles, bone structures and teeth3. Some authors claim that some buccolingual tooth movement is necessary during treatment in order to correct buccolingual inclinations and improve occlusal interfacing. Such movement is limited by alveolar bone and periodontal tissues1,5,18 called by Andrews as the WALA ridge19. The new positions of teeth are mainly determined and limited by the mandibular morphology, which is established around 8.5 weeks of intra-uterine life8. It is believed the maxillary arch shape is determined by the mandibular teeth5,8 due to the similarity between mandibular and maxillary arches morphology and their morphogenesis11. As such, in pursuit of defendable, evidence-based treatment results, orthodontists should first consider the anatomic limits of the mandibular arch. In the beginning of orthodontic treatment, in the leveling and alignment phase, elastic-alloy-wires (such as Ni-Ti), as a standard, or average shape and size (i.e. oval, which is the most prevalent) could be utilized. After this phase, maintaining the dental arch configuration, as it relates to basal bone, is essential to the success of the orthodontic therapy because of its great influence on stability12,20. It has been suggested5 to use reference models, called "diagrams", to assist in forming orthodontic wires or in the selection of pre-formed archwires. The diagrams are based on measures of the dental arch elements, mainly, the inter canines distance and can provide parameters about the pre-treatment arch wire shape. Choosing a personal diagram for the patient, the metallic arches would be contoured in a standard shape and dimension, allowing the maintenance of the transverse dimension during treatment. There are several studies suggesting different methods for the attainment of optimum arch shape. Some authors have suggested using photocopies of the occlusal aspect of the dental casts to select the arch configuration, based on pre-contoured arches4. Another option is the application of a Cartesian system to the cast photocopies, identifying x and y axes, to facilitate the visual evaluation of the arch morphology among three preselected shapes (square, tapered, oval)17. Recently, some authors presented the digitization of natural normal occlusion casts followed by the application of sixth-degree polynomials, establishing the six most preponderant arch configurations, guiding the orthodontist to choose visually, among these shapes, the one best fit to each patient8. Thus, it was observed that, independent of the complexity of the methodology used to determine and choose the dental arch shape, the final choice is made by the orthodontist in a visual way, and so, subjectively. Searching in literature, it was observed that several authors had found more than one dental arch shape6,20, but there is not a consent about the amount of joined forms. According to a previous study9, the dental arches of natural normal occlusion individuals presented the anterior region in semicircle and the posterior teeth in straight-line, while the malocclusion arches were represented by four distinct forms. However, other authors, evaluating a sample comprised of normal occlusion and malocclusion casts had found five to six8 different geometric configurations to the mandibular dental arch. Despite the authors' agreement about the diversity of morphologies that best described the dental arch, some differences might have occurred because of the kind of methodology used. The use of three dental arch shapes was initially classified in 193413, looking for the improvement, customization, and simplification of treatment planning. The square morphology is indicated to large dental arches in which it is necessary to preserve morphology after rapid or slow expansion treatment. It presents the anterior region of the arch flat, arranging the central and lateral incisors in straight-line and the posteriors teeth almost vertical in the alveolar bone. In this study, this configuration was found in 39% of the sample, data different from other studies4,17-18. The tapered configuration, unlike the previous one, is usually used in atrophic arches, presenting a smaller intercuspal distance. This shape could be proper to adult patients, because it minimizes the relapses and the periodontal problems happening, in special in patients with thin periodontal profile. The present study showed 21% of tapered arch morphology, similar to other study findings4 and different from others17,20. The oval shape, used often by orthodontists, shows a little greater intercuspal distance than the tapered arches. It was the most common arch morphology in the present sample (41%) as in other studies13,20, and when the ovoid shape was not the majority, it showed significant percentages21. In conclusion, the shape of the mandibular dental arch with highest prevalence was the oval (41%), followed by the square shape (39%), which showed very similar in results. The tapered shape was the lowest prevalent (20%). As a clinical application, at the beginning of the orthodontic treatment, during leveling and alignment phases, elastic-alloy-wires are greatly used and, in order to facilitated orthodontist work, any of the studied arch shapes could be used, once the prevalence of all of them was similar. After this, the orthodontist should observed the patient's dental arch morphology and choose an archwire shape that best fits. References
© Copyright 2011 Braz J Oral Sci The following images related to this document are available:Photo images[os11013f2.jpg] [os11013f1.jpg] [os11013t1.jpg] [os11013f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}