 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
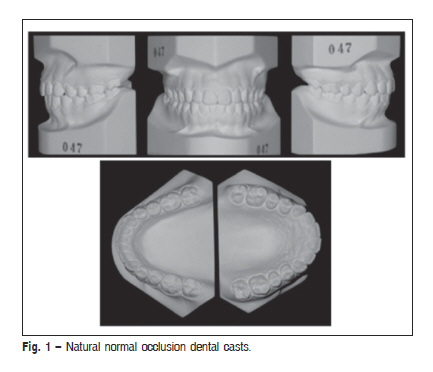
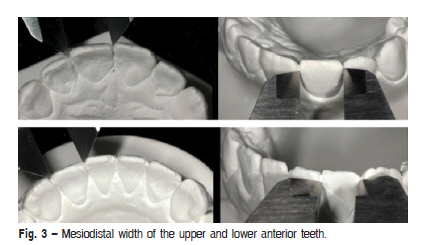
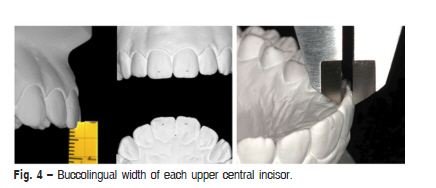
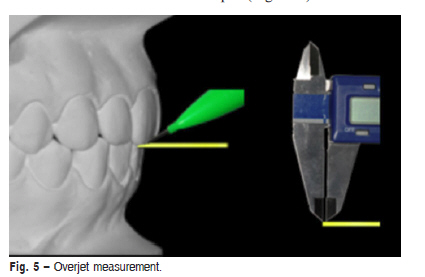
Brazilian Journal of Oral Sciences, Vol. 10, No. 2, Apr-Jun, 2011, pp. 69-73 Factors related to Bolton's anterior ratio in Brazilians with natural normal occlusion Renata Pilli Jóias1, Marco Antonio Scanavini2 1 DDS, MS, Department of Orthodontics, School of Dentistry, Methodist University of São Paulo (UMESP), Brazil Received for publication: November 21, 2010 Correspondence to: Renata Pilli Jóias Universidade Metodista de São Paulo Faculdade da Saúde - Departamento de Pós-Graduação em Odontologia-Ortodontia Rua do Sacramento, 230 Edifício Lambda sala 250 - 09640-000 Phone: 55 11 4366-5826, 55 11 9697-9517 E-mail: pillijoias_renata@yahoo.com.br Code Number: os11014 AbstractAim: To verify whether some factors could be related to Bolton's anterior ratio:
buccolingual thickness of upper incisors, mesiodistal tipping of upper incisors, overjet and overbite, and if
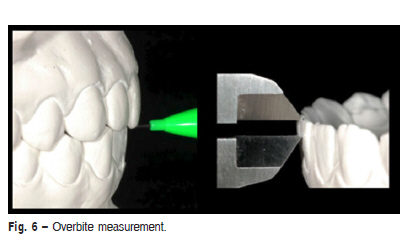
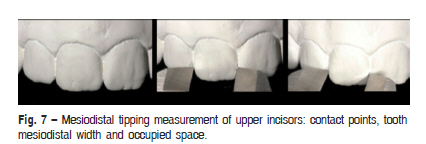
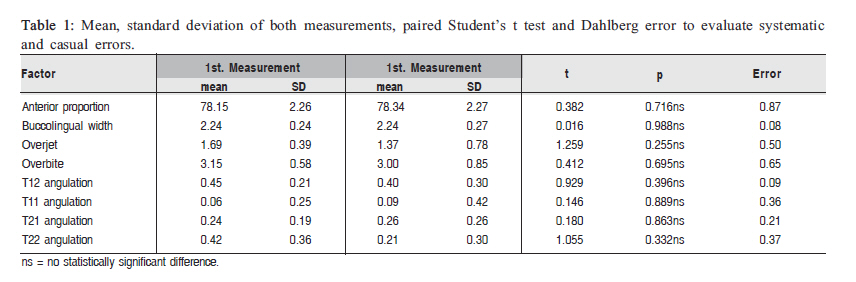
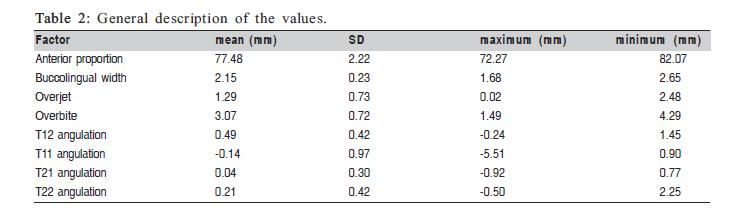
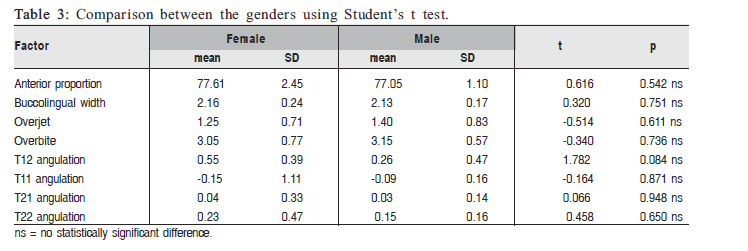
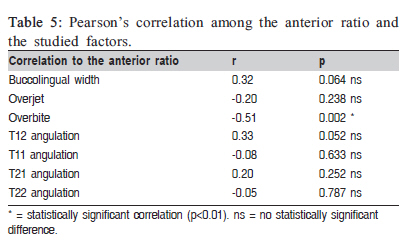
there is gender dimorphism. Keywords: orthodontics, dental occlusion, dental crown. Introduction The orthodontic treatment attempts to reproduce natural normal occlusion's features that just became possible after carefully observing and recognizing the common ones among them, which were responsible for these occlusion's harmony, beauty, good function and stability. Thus, aligned teeth, tight contacts, and appropriated overjet and overbite1, should be contemplated at the treatment planning to avoid problems on intercuspation caused by some occlusal disharmonies, similar to tooth size discrepancies. Since the beginning of 20th century, human tooth size has been studied2 and the differences between the mesiodistal width of right and left teeth have been observed3. Neff4 was the first author who introduced the importance of upper and lower tooth mass correct relationship, and Bolton5-6 proposed ratios in order to correlate them without contemplating bone discrepancies. Other studies followed questioning Bolton's ratios in different racial groups7-9, types of malloclusions10-12 and gender10-11, and their correlation with overjet, overbite, upper incisor buccolingual thickness and arch form13-15, without reaching a conclusion. Considering that 30%8,16 of the people who seek orthodontic treatment have anterior tooth size discrepancy and that in 35% of them there are more than a 2 mm17 excess, the objectives of this study were to evaluate whether Bolton's anterior ratio for Caucasian Brazilians with natural normal occlusion is similar to the Bolton's anterior ratio for North-Americans; if there is correlation between Bolton's anterior ratio and buccolingual thickness of upper incisors, mesiodistal tipping of upper incisors, overjet and overbite; and if there is gender dimorphism. Material and methods Sample Thirty-five pairs of dental casts from Caucasian Brazilians with natural normal occlusion, aged between 13 years old and 17 years and 4 months (mean age: 15y8m), 27 females and 8 males, were selected as reported in a previous study18. After being carefully evaluated by a specialist, the occlusions were considered normal when presenting ideal static (maximum intercuspation similar to centric relation) and dynamic occlusal features (left and right lateral excursions and straight protrusion without any interference) (Figure 1). Measurements A lead pencil (0.5 mm), a ruler and a digital caliper (Mitutoyo 500-144b, Brazil) with 0.01 mm accuracy were used to make the measurements. A 2-mm piece of the ruler was cut to facilitate some measurements (Figure 2). The greatest mesiodistal distance of each anterior tooth, from right to left canine, was taken with the digital caliper perpendicular to tooth's long axis (Figure 3). The buccolingual width of each upper central incisor (right and left) was obtained to find the mean value. Using the ruler, a point was marked at the buccal face of the tooth and another at the lingual face, 2 mm far from the incisal border15. The caliper was positioned on both points to obtain the buccolingual width (Figure 4). In order to obtain overjet and overbite, it was first verified the relationship between the right upper and lower central incisors, and the same for the left ones. To measure the overjet, the piece of ruler touched the lower incisor buccal face perpendicular to it, tangent to the upper incisor incisal border. The distance between the upper incisor border and the lower incisor buccal face was verified with the piece of ruler and measured with the caliper (Figure 5) (Fig. 1). Statistical Analysis The unpaired Student's t test was used to compare the original Bolton values to this study's anterior ratio, and to identify possible differences between genders. The association between Bolton's anterior ratio and the buccolingual thickness of upper incisors, mesiodistal tipping of upper incisors, overjet and overbite, and gender dimorphism, was evaluated by the Pearson's correlation. A significance level of p < 0.05 was applied for these tests.to the first molars, which will not change the Angle molar relation either. In this way, it is believed that repeating the measurements of this study in Classes I, II or III malocclusion groups is not necessary, which allows the values established for normal occlusion to be applied to everyone, since the goal of orthodontic treatments is to turn malocclusions into normal occlusions. After a 20-day interval, 7 dental casts were measured again to evaluate the reliability of the measuring method. Systematic error was calculated using the paired Student's t test at p < 0.05, and casual error was evaluated by the Dahlberg test. Results The systematic and the casual errors are shown in Table 1. Table 2 presents the maximum and minimum values, mean and standard deviation to the dental ratio and to each factor. Gender dimorphism in relation to the anterior ratio and the factors studied are shown in Table 3. Table 4 shows the mean and standard deviation achieved in this study compared to Bolton's values. The correlation among the factors and the anterior ratio are shown in Table 5. Discussion Upper and lower tooth mass excesses may possibly impair a desired orthodontic finalization. Upper excess causes a large amount of overbite and overjet, upper anterior crowding, spaces among lower anterior teeth, lingual tipping of upper incisors and buccal tipping of lower incisors14. Otherwise, lower excess could bring about not enough overjet and verbite, lower anterior crowding, spaces among upper anterior teeth, buccal tipping of upper incisors and lingual tipping of lower incisors14. Comparing Classes I, II and III malocclusions, the Bolton's tooth size discrepancy (DTSD) did not show statistically significant difference16 nor gender dimorphism12,15-16. Other authors11 informed a greater anterior ratio in natural normal occlusions than in Class III, but they did not detailed the inclusion criteria to be considered as normal occlusion and did support that Bolton's ratios were the same among all malocclusion groups. Therefore, as they stated that among malocclusions the Bolton's ratios did not show a statistically significant difference, how could the anterior ratio be smaller only in Class III in relation to normal occlusion? If the anterior ratio is similar to all malocclusions, in case the normal occlusion anterior ratio is greater, shouldn't it be greater than all the malocclusions ratios? Although the DTSD is related to other dental features in Classes I, II and II individuals, it does not induce bad molar relationship10, justifying the sample choice of the present study. It means that since the presence of DTSD is not responsible for the molar bad position, management of the tooth mass needs to be done in the teeth located anterior to the first molars, which will not change the Angle molar relation either. In this way, it is believed that repeating the meaurements of this study in Classes I, II or III malocclusion groups is not necessary, which allows the values established for normal occlusion to be applied to everyone, since the goal of orthodontic treatments is to turn malocclusions into normal occlusions. The anterior ratio obtained in this study is similar to the ratio obtained by other authors7,19, including Bolton, whose sample was comprised of both normal occlusion (n=11) and malocclusion individuals (n=44). Thus, judging the value found in this research reliable for the anterior ratio makes it possible to associate it to the other factors. Regarding to the anterior ratio related to the gender, it was not found a statistically significant difference, which allows the assumption that the gender dimorphism found in crown size9,19 is not a sufficient amount to cause this dimorphism in the anterior ratio. It was found that the buccolingual thickness of incisors had a similar value to those reported in the literature14, but a correlation with the anterior ratio was not observed. Conversely, other studies13-15 has stated that thicker upper incisors bring about a smaller anterior ratio. It may not be just because of the incisor thickness, but because of the tooth size in general, we mean that if an incisor is thicker, it is bigger in all its other faces as well, like length and width, so it will increase the maxillary tooth mass and create a smaller anterior ratio. It means that, a thicker tooth would probably be larger even in the mesiodistal and occlusogingival widths. Thus, it may be speculated that the anterior ratio would increase because of larger upper incisors, in general, needing more research studies to scientifically prove this fact. It was found an overjet similar to that reported in previous studies, with values from 0mm to 3.7mm (mean=1.6mm)1, and 1.17mm to 3.75mm (mean=2.77, SD±0.65)14. In this study, a correlation between the overjet and the anterior ratio was not found, although, some authors14-15 explained that when the overjet is increased, the overbite also is increased. Other authors13 have stated that 1 to 3-mm-ticker central incisors, in straight arches would compensate for 1-mm-excess overjet when a decreased anterior ratio exists. On the other hand, thinner incisors would contribute to increased overjet in curve arches with increased anterior ratio. The Pearson's test showed a 99% reliable correlation between the overbite and the anterior ratio. Neff4 established an ideal anterior coefficient of 20% based on orthodontically treated patients. However, this author affirmed that the study should be performed on natural normal occlusion patients, which he had not done due to the difficulty in composing the sample. The measurements of this study showed a mean occlusogingival size of the lower incisors around 9.01 mm. Applying the Neff's index, a mean overjet of 34.07% would be found, greater than Neff's4 and similar to Bolton's6 values (11.8% and 53.9%, mean=31.3%). According to Lavelle19, when compared to melanoderms and xanthoderms, Caucasians present the smallest anterior ratio (77.15% ± 1.55) and the greatest overbite (30.6% ± 9.18). The anterior ratio value is similar to the one found in this study, and probably smaller to the other racial groups' due to their tendency to have larger teeth. The overbite verified in this study is greater than Lavelle's19 value for Caucasians, which may be explained by the fact that Caucasians have larger upper central incisors in relation to their other teeth, which usually does not happen to melanoderms and xanthoderms. Considering the overbite in millimeters, this study's value would not be so different from those found by other authors. Steadman1 proposed an overbite of 3.1 mm ± 1.91, in a range from 0.5 to 4.3 mm. Another study14 described a mean overbite of 2.49 mm ± 0.86, varying from 1.05 to 4.60 mm, at the post-treatment period. The mesiodistal tipping of incisors was idealized by this study's supervisor to subjectively identify smooth angulations, which are welcome in good occlusions. Hence, studying a normal occlusion sample, these gentle angulations could be visualized and taken in order to know whether they interfere or not on the attainment of the teeth mesiodistal width, used for the anterior ratio calculation. Since only the overbite showed inversely proportional relation to Bolton's anterior ratio, it is believed that if the anterior ratio is increased (mandibular tooth mass excess or lack of maxillary tooth mass) the overbite could be decreased and if the anterior ratio is decreased, the overbite may be increased. In those cases with normal anterior ratio, but deep overbite, the overbite could result from thinner upper central incisors with larger crown because, even though the upper central incisors appear larger in relation to the other teeth, it is common to observe smaller upper lateral incisors, balancing the anterior tooth mass and not incurring in anterior tooth size discrepancy. In this study it was not found statistically significant difference between Bolton's anterior ratio and the ratio found in this sample; the overbite was inversley proportional to Bolton's anterior ration, being that: when the anterior ratio is increased, the overbite could be decreased and vice-versa; and there was no gender dimorphism. References
© Copyright 2011 Braz J Oral Sci The following images related to this document are available:Photo images[os11014f5.jpg] [os11014f1.jpg] [os11014t1.jpg] [os11014f3.jpg] [os11014t4.jpg] [os11014t5.jpg] [os11014f4.jpg] [os11014f7.jpg] [os11014f2.jpg] [os11014t2.jpg] [os11014f6.jpg] [os11014t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}