 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
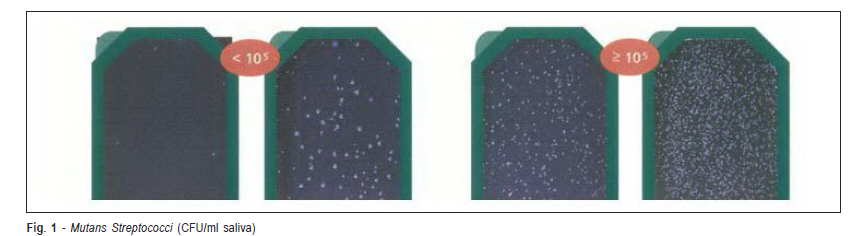
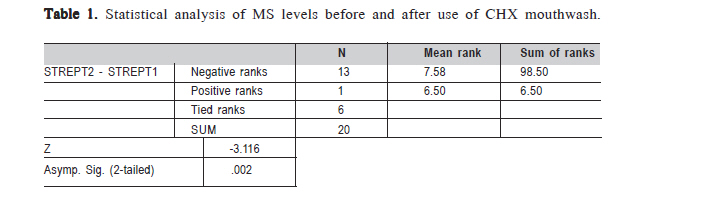
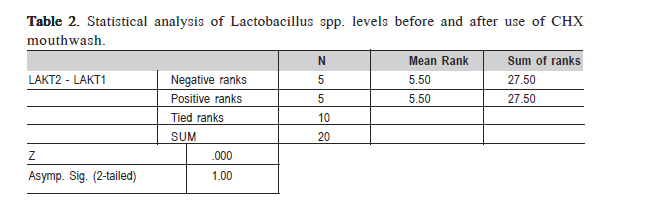
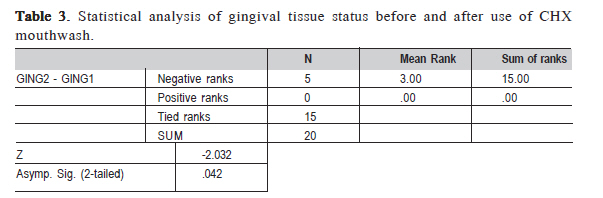
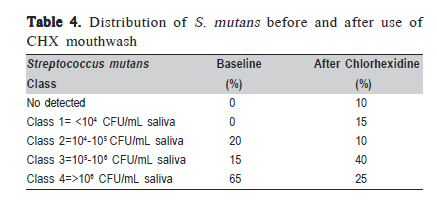
Brazilian Journal of Oral Sciences, Vol. 10, No. 2, Apr-Jun, 2011, pp. 79-82 Antimicrobial activity of chlorhexidine in patients with fixed orthodontic appliances Nakas Enita1, Vildana Dzemidzic1, Alisa Tiro1, Enes Pasic2, Sanja Hadzic2 1DDS, Msc, Senior research assistant, Department of Orthodontics, School of Dentistry, University of Sarajevo, Sarajevo, Bosnia and Herzegovina Correspondence to:Nakas Enita Department of Orthodontics, School of Dentistry, University of Sarajevo Bolnièka 4a , 71 000 Sarajevo, Bosnia and Herzegovina Phone: ++ 387 61 10 02 29 E-mail: enitta@gmail.com Received for publication: January 01, 2011 Accepted: April 19, 2011 Code Number: os11016 AbstractAim: Oral environment of orthodontic patients undergoes changes, such as pH reduction, larger number of sites available for Streptococcus mutans collection, and increased accumulation of food particles, which may lead to an increased number of S. mutans colony-forming units (CFU) in saliva. Chlorhexidine gluconate (CHX) is the most potent documented antimicrobial agent against Mutans streptococci and dental caries. The aim of this work was to assess efficiency of CHX-based mouthwashes in patient with fixed orthodontic appliances. Keywords: chlorhexidine, Streptococcus mutans, orthodontic treatment. IntroductionBonded orthodontic appliances increase the number of plaque retention sites,reduce the possibility self-cleaning on vestibular areas and impede oral hygiene.As of result of this, the oral cavity of orthodontic patients undergoes changes,such as pH reduction, larger number of sites available for Streptococcus mutanscollection, and increased accumulation of food particles, which may lead to anincreased number of S. mutans colony-forming units (CFU) in saliva1. Dental plaque is a multi-species biofilm consisting of more than 700 speciesof oral bacteria on tooth surfaces, and mutans streptococci (MS) are the majorgroup of early primary colonizers2. MS are microorganisms that primarily colonizedental surfaces. At concentrations of 104-105 CFU/mL in saliva, S. mutans is able to colonize clean, smooth surfaces of teeth. The presence of MS on tooth surfacesincreases the possibility of caries development3. Due to some of their vital characteristics, MS are regarded potentially highly cariogenic4. Therefore, preventiveefforts in these risk groups have concentrated on direct suppression of the cariogenicmicroflora by chemotherapeutics as an adjunct to improved oral hygiene. Chlorhexidine gluconate (CHX) is the most potent documented antimicrobialagent against MS and dental caries5. Mouth rinsing with a chemical agent could be a useful clinical adjunct for reducing the bacterial plaqueaccumulation during the active phase of orthodontictreatment. Chemical agents also help orthodontic patientswho have difficulties in maintaining plaque control bymechanical means alone. The aim of this work was to assess efficiency of CHX-based mouthwashes in patients with fixedorthodontic appliances. Material and methodsTwenty patients with fixed appliances were selected forthis study. The following criteria were used for selectingpatients who were undergoing full-banded non extractiontreatment with metal brackets (Roth 0.22, Dentaurum GmbH & Co., Ispringen, Germany) on their teeth and bands on theirmolars who: were at least 13 and no more than 18 years oldwith complete permanent dentition including second molars;had no evidence of decalcification on their teeth; had no active caries lesion; had no known medical problem or currentantibiotic therapy; had anterior composite fillings; had noknown hypersensitivity to CHX. Each patient was provided with a toothbrush, atoothpaste and a leaflet with brushing instructions; Allpatients were instructed to brush for a minimum of 3 min. The same protocol was followed for each patient. First,the gingiva of individual teeth was examined and scoringwas performed, according to the following scoring system: 0: Normal gingiva; 1: Slight inflammation - a minor changein color, consistency (no bleeding on probing); 2: Averageinflammation - redness, swelling (bleeding on probing); 3:Severe inflammation - strong redness and swelling(spontaneous bleeding). Final score was obtained when thetotal score was divided by the number of examined teeth. After collection of stimulated saliva sample for the purpose of establishing the quantities of S. mutans and Lactobacillus spp.. Saliva samples were collected at twotimelines for each patient: 1. Before use of CHX (at least 1month after bonding); 2. After 2 weeks of use of CHX. Forsuch purpose, colony counting test kit (CRT Bacteria, IvoclarVivadent, Liechtenstein) was used, according to manufacturer's instruction. Patients were given a piece of (factory-made)wax, which they chewed for 5 min in order to collect enoughstimulated saliva. While chewing, they collected saliva intodisposable sterile plastic cups. After 5 min, disposable pipettes were used to take salivaand seed it on slides for Streptococci mutans and Lactobacilli spp. The protective coat from sterile slides was removed, 5drops were neatly dripped on the slide (until its entire surfacewas covered in saliva), which was held under a slight angle,taking special care not to damage the surface of the slidewith the sharp edge of pipette. Once the procedure was over,a tablet of NaHCO3 was put in slide boxes, and then theboxes were closed and placed into an incubator at 37°C.Forty-eight hours later, the results were read as indicated inthe manufacturer's scheme, according to the following scale:Class 1= <104 CFU/mL saliva; Class 2=104-105 CFU/mLsaliva; Class 3=105-106 CFU/mL saliva; Class 4=>106 CFU/mL saliva (Figure 1.) The mouthwashes were used by patients according to themanufacturer's directions 15 min after toothbrushing: 5 mLof 0.2% CHX (Corsodyl, GlaxoSmithKline) was applied for60 s in the morning and at bedtime for 2 weeks. The patientswere instructed not to consume any liquid or food or at least30 min after using the prescribed mouthwash. All patients areasked to bring the mouthwash bottle, so we could determinepatient compliance based on how much liquid was left. The data were analyzed using the nonparametricWilcoxon signed rank test (SPSS software, SPSS Inc., Chicago,IL, USA). Statistical significance level was set at p <0.05 ResultsThe results of the statistical analysis of MS levels,Lactobacillus spp. levels and gingival tissue status beforeand after use of CHX mouthwash are presented in Tables 1,2 and 3. The distribution of S. mutans before and after use of CHX mouthwash is given in Table 4. The findings of the present study indicate that the useof CHX mouthwashes reduced S. mutans levels (p = 0.002)in patients with fixed orthodontic appliances. Thirteenpatients presented lower S. mutans while in 6 patients S. mutans counts remained the same regardless of use of theantimicrobial agent. CHX-based mouthwash had no significant impact on Lactobacillus spp. levels, as 5 patients presented highercounts, 5 presented lower counts while in 10 patientsLactobacillus spp. counts remained the same regardless ofuse of the antimicrobial agent. Discussion The findings of the present study regarding the effect of the CHX mouthwash on the microbial counts are in accordance with those of other authors. Oltramari-Navaro et al. (2009)6 suggested that the use of dentifrices withlower CHX concentration can reduce the risk of tooth staining without compromising its effectiveness incontrolling gingivitis and bleeding in orthodontic patients.Masek et al. (2008)7 found that Cervitec® caused a reduction of S. mutans and Lactobacillus spp. saliva countsin patients with previously identified high level of these bacteria. Sari (2007)8 reported that 0.2% CHX mouthwash decreased S. mutans levels, but had no effect on lactobacilli levels. Olympio et al. (2006)9 observed that the use of dentifrices containing CHX seems to be effective for thetreatment of gingivitis in orthodontic patients. Beyth(2003)10 found a significant reduction of S. mutans CFU in 10 patients after use of CHX oral rinse10. According toEldridge (1998)11, the use of CHX mouthwash reduces the levels of S. mutans, gingival index and gingival bleeding.Anderson (1997)12 found that the use of CHX oral rinse contributes to improving oral hygiene in patients withfixed orthodontic appliances12. In the present study, 6 patients reported discolorationof teeth as a result of the treatment, which is a possibleside effect o CHX. Eldridge (1998)11 described the appearance of brown color tongue that spontaneouslyresolved after cessation of the use of CHX, which, however, was not observed in the present study. Anderson (1997)12 observed discoloration of teeth and increase in dental calculus formation, but they did not determine thesignificance of these phenomena. Our results corroborate previous findings about theinfluence of CHX on S. Mutans levels, oral hygiene andgingival condition13-14. In the present study, the use ofCHX-based mouthwashes reduced S. mutans counts and improved the gingival index, but had no significant impacton Lactobacillus counts. References
Copyright © 2011 - Brazilian Journal of Oral Sciences The following images related to this document are available:Photo images[os11016t1.jpg] [os11016t4.jpg] [os11016f1.jpg] [os11016t3.jpg] [os11016t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}