 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 10, No. 3, Jul-Sept., 2011, pp. 189-192 Microhardness of nanofilled composite resin light-cured by LED or QTH units with different times Ana Isabelle Salvador Groninger1, Giulliana Panfiglio Soares2, Robson Tetsuo Sasaki3, Glaucia Maria Bovi Ambrosano4, José Roberto Lovadino5, Flávio Henrique Baggio Aguiar6
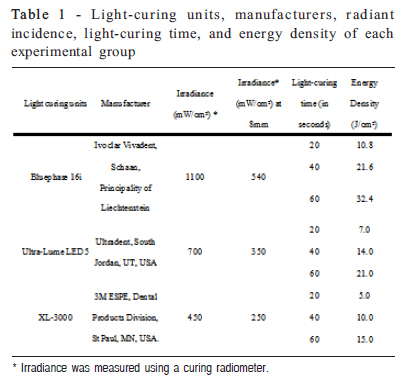
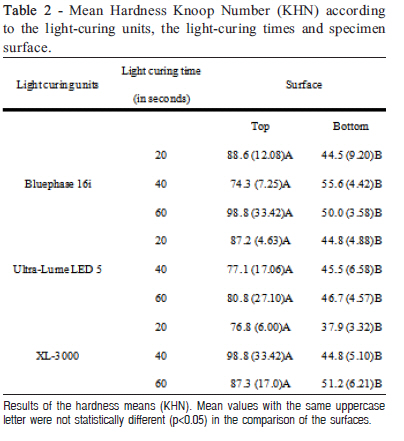
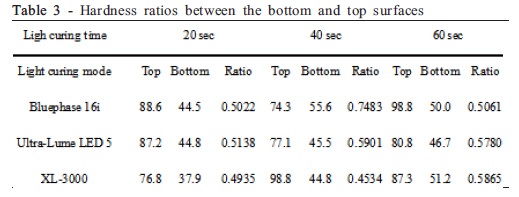
1Undergraduate student, Department of Restorative Dentistry, Piracicaba Dental School, University of Campinas, Brazil, 2DDS, MS, PhD student, Department of Restorative Dentistry, Piracicaba Dental School, University of Campinas, Brazil, 3DDS, MS student, Department of Restorative Dentistry, Piracicaba Dental School, University of Campinas, Brazil, 4DDS, MS, PhD, Assistant Professor, Department of Community Dentistry and Statistics, Piracicaba Dental School, University of Campinas, Brazil, 5DDS, MS, PhD, Chairman, Department of Restorative Dentistry, Piracicaba Dental School, University of Campinas, Brazil, 6DDS, MS, PhD, Assistant Professor, Department of Restorative Dentistry, Piracicaba Dental School, University of Campinas, Brazil Abstract Aim: To evaluate the influence of light-curing units and light-curing time on the microhardness of a nanofilled composite resin. Keywords: composite resins, hardness. Introduction Composite resin has been described as an esthetic restorative material with excellent physical and mechanical properties1 when adequate polymerization is obtained2. However, many variables affect the amount of light energy received on the top and bottom surfaces of a composite resin restoration, such as the design and size of the light guide, distance of the light guide tip from the composite resin, power density, exposure duration, shade and opacity of the composite resin, increment thickness, and material composition3-5 . If the restoration does not receive sufficient total energy, various problems may arise, e.g., reduced degree of conversion, increased cytotoxicity, reduced hardness, increased pigmentation, decreased dynamic elasticity modulus, increased wear, increased marginal leakage and weak a bond among the tooth, adhesive, and restoration3-4,6 . Clinically, deficient polymerization can occur in deeper cavities due to the dispersion of light energy that occurs because of the distance between the light-curing tip and the first composite resin increment7. In a deeper cavity, the interface between the composite resin and the tooth structure may be less polymerized, and exposure of this interface to the oral environment can generate marginal discolorations, restoration fractures, and composite resin and adhesive solubility, leading to microleakage and secondary caries7 . However, few studies have been conducted with the purpose of testing the depth of composite resin curing in situations where the light-curing tip is distant from the filling material, as in the aforementioned clinical situations. Thus, it is important to evaluate the minimum light-curing time required for correct polymerization in accordance with the light-curing unit used. The aim of this in vitro study was to evaluate the influence of the light-curing time using LED or QTH on the hardness of the top and bottom composite resin surfaces in a clinical simulation when the light-curing tip was at distance of 8 mm and the material thickness was 2 mm. Material and methods A nanofilled composite resin, Z350 (3M-ESPE Dental Products, St. Paul, MN, USA), was used in this study. Fortyfive cylindrical specimens were prepared using Teflon ring molds (4.0 mm internal diameter and 2 mm depth) held between two glass slabs separated by Mylar matrix strips and then pressed with a 500 g static load. The cavities were randomly filled in one resin increment and polymerized according to the nine experimental groups (n=5): three polymerization units (conventional - 450 mW/cm2; 2nd generation LED - 1100mW/cm2; 3rd generation LED -700mW/cm2) and three light-curing times (manufacturer’s recommended time - 20s; twice the manufacturer’s recommended time - 40s; and thrice the manufacturer’s recommended time - 60s). Polymerization was performed with a source-to-specimen distance of 8 mm, checked with a digital caliper (Mitutoyo, USA). Irradiance of the light curing units was measured using a curing radiometer (Demetron Research Corp., Danbury, CT, USA). The energy density was calculated according to the product of the irradiance of the light curing unit (mW/cm2) X exposure duration (s) (Table 1). Each specimen was removed from the mold and stored in a lightproof container at 37C and 95 ± 5% relative humidity for 24 h. After this period, the specimens were washed and the Knoop hardness on the bottom and top surfaces was tested using a Knoop hardness indenter (FM -Future Tech Corp., Japan) under a 10 g load for 10 s. Five measurements were made at the approximate center of the specimen4. The values, obtained in micrometers, were converted to Knoop Hardness Number (KHN) using computer software (Microsoft Excel for Windows®). The Knoop hardness values obtained on top and bottom surfaces were subjected to the subdivided parcel ANOVA (Split-Plot) test (p=0.05) and Tukey’s test at the 5% Table 1 -Light-curing units, manufacturers, radiant incidence, light-curing time, and energy density of each experimental group significance level. The light-curing unit and light-curing time factors were considered in the parcels, and the factor surface (top and bottom surfaces) was considered in the sub-factor. Results The ANOVA results showed no statistically significant differences among the light-curing units (p=0.3007) or among the light-curing times (p=0.1819). The interactions of the light-curing mode x light-curing time (p=0.2224), light-curing mode x surface (p=0.3136), surface x lightcuring time (p=0.1036), and light-curing mode x light-curing time x surface (p=0.0705) also were not significant. There was a significant difference between the surfaces (p <0.0001) in that, for all the experimental conditions, the top surface showed higher hardness values than the bottom surface (Table 2). Considering the ratio between the bottom and top surface hardness values (Table 3), the highest ratio was obtained by Bluephase 16i with 40 s light-curing time (@ 0.75). In the other experimental conditions, the ratio was lower than 0.6. Discussion The present study evaluated the influence of light-curing units and light-curing times on the microhardness of top and bottom nanofilled composite resin surfaces. The results showed that, for the top and bottom surfaces, there were no statistically significant differences among light-curing units or among lightcuring times. For all experimental conditions, the top surface showed higher hardness than the bottom surface. The depth of cure for composite resin can be affected by several factors associated with the source of light polymerization, including the spectral emission (wavelength distribution), light intensity, exposure period, and irradiation distance4,8-11. Among these factors, the radiant incidence of light given out by different light-curing units and the lightcuring times were analyzed in this study. The results showed that these two factors were not able to significantly affect the microhardness of polymerization on the top and bottom surfaces. In other words, when the light-curing time recommended by the manufacturers (20 s) was doubled or tripled, the hardness values did not increase. Regarding the light-curing units used (Bluephase 16i - Vivadent, Ultra-Lume LED 5 - Ultradent, XL 3000 - 3M ESPE), there were no statistically significant differences among them, independent of the light-curing time used and of the energy density at the tip of the light-curing units (Table 2). Energy dispersal can take place when polymerization happens with the tip of the light-curing unit at a distance from the surface of the composite resin, and this approximate irradiance that reaches the surface is independent of the irradiance released by the light-curing unit12 (Table 1). Similarly, in a study conducted by Aguiar et al.12, there were no statistically significant differences between the top surfaces of the specimens. The study also showed that when the lightcuring time recommended by the manufacturer was tripled, higher hardness values were obtained on the bottom surface. However, Gomes et al.13 and Awliya14 obtained different hardness values when comparing the light-curing of LED and halogen lights. In the present study, there was no significant difference for the studied factors on the bottom surface. The difference in the results between the present study and the studies mentioned above can be explained by two hypotheses: 1) light penetration on the bottom surface of the nanofilled resin might have happened in a similar way, regardless of the light-curing mode or photoactivation time; and 2) nanofilled resin presents better physical properties when compared with other resins15-16 and, due to its high load content (78.5% by weight), the degree of polymerization was not the main factor in the hardness values obtained. In a recent study17, light-curing units with different irradiances did not result in significant hardness differences on the bottom surface when a nanofilled composite with similar translucency was used. In the same study, higher radiant exposure increased the hardness of the bottom surface only for the composite resins with higher opacities (dentin shade). Thus, although the hardness of the bottom surface was significantly lower than that of the top surface for all groups in the present study, increased radiant exposure did not improve the hardness of the bottom surface for composite resins with translucent characteristics. In addition, the nanofilled composite resin used in the present study showed an adequate entanglement between the resin components and the nanofillers, which improves the physical properties of the material18. Thus, possibly even with a lower degree of conversion, the bottom surface of the specimen may have showed similar hardness due to the filler system used. Another finding of this study was that, for all the experimental conditions, the top surface showed higher hardness values than the bottom surface. This could be due to the capacity of the composite resin to reduce light penetration, which causes a reduction in the irradiance and, consequently, the efficiency of polymerization of the bottom surface7,12,19-21. Furthermore, on the top surface, high irradiance photoactivation initiated a multitude of growth centers of polymers with higher cross-linking density22-23 . Low irradiant energy reached the bottom surface, decreasing the cross-linking density and the hardness of the composite resin24-25 . Yap et al.20 affirmed that the hardness ratio between the bottom and top must be 1 to consider the polymerization completely efficient, but even a proportion of “approximately 0.8” can be considered an appropriate polymerization. In this study, the results showed that the proportion was between 0.50 and 0.74 for groups in which the Bluephase 16i lightcuring unit was used, between 0.51 and 0.59 for groups in which the Ultra-Lume LED 5 light-curing unit was used, and between 0.45 and 0.59 for groups in which the XL-3000 lightcuring unit was used (Table 3). This shows that, although not presenting a ratio between 0.8 and 1.0, as suggested by Yap et al.20, the ratios obtained in the present study were higher in relation to the study of Aguiar et al.12 So it may be suggested that the nanofilled composite resins showed higher hardness on the bottom surface than the micro-hybrid resins. It may be concluded that the mode of polymerization and the light-curing time did not affect the hardness of the nanofilled composite resin and that increasing the light-curing time did not improve the hardness of the bottom surface of the composite resin. Further studies must be carried out to compare the best efficiency of the nanofilled resin compared with other resins used for subsequent teeth and to determine whether the degree of conversion of the compound nanofilled resin interferes with the superficial hardness. Acknowledgements This study was supported by FAPESP (grant # 06/61136-3). References
Copyright © 2011 - Brazilian Journal of Oral Sciences The following images related to this document are available:Photo images[os11038t2.jpg] [os11038t1.jpg] [os11038t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}